Right Click and Choose Save-as to Download the Podcast.
PHARM Podcast 223 Fear of flying in aeromedical retrieval and a dedication to Loretto Harvey
Aug 31, 2019
The colleagues of Loretto Harvey, who died while competing in the Townsville Triathlon Festival last weekend say she was caring and selfless. The 50-year-old was well known for her nursing role at the Rural Flying Doctor Service. Report on 7NEWS at 6pm. #7NEWSpic.twitter.com/mVIhEwxPLk
Right Click and Choose Save-as to Download the Podcast.
PHARM Podcast 218 The Women Doctors who fought to serve
May 01, 2019
Vera Scantlebury (later Scantlebury-Brown) and Rachel Champion (later Shaw) were two of the first women graduates of the University of Melbourne Medical School. They are pictured here serving at London’s Endell Street Military Hospital, in WW1. Picture: Imperial War Museum . This image and contents of podcast are reproduced here under this Creative Commons licence Hi folks! A reading of an essay from University of Melbourne on Australian Women Doctors in World War One Show Notes: THE WOMEN DOCTORS WHO FOUGHT TO SERVE
Right Click and Choose Save-as to Download the Podcast.
From Sedation Death We learn
Jan 27, 2017
Hi folks
THis is a sedation related death of a suicidal patient under the involuntary section of the Mental health act. This should never happen but it does and I have written and spoken about this before . Colleagues such as Tim Leeuwenburg and Casey Parker have also documented such issues on their respective sites in the past. It has and still is the impetus for our creation and promotion of the Surviving Sedation Guidelines
There has also been a 2016 ketamine sedation death from America since many believe that ketamine cannot kill you. It can.
Hi folks, I chat to MICA paramedic Matt Shepherd on CPR induced conciousness. yes its a real thing and yes you should know what to do about it if it happens .
A ketamine protocol & intubation rates for psychiatric aeromedical retrieval
Minh Le Cong, MBBS, FRACGP, FACRRM, FARGP, GDRGP, GCMA, and Ian Humble, BSc MBChB
Royal Flying Doctor Service, Mount Isa Base, Mount Isa, Queensland, Australia Cairns Hospital Emergency Department, Cairns, Queensland, Australia Address for correspondence: Minh Le Cong, MBBS, FRACGP, FACRRM, FARGP, GDRGP, GCMA, Royal Flying Doctor Service, Mount Isa Base, 11 Barkly Highway, Mount Isa, QLD, Australia 4825, mlecong@rfdsqld.com.au
(This is the accepted manuscript to Air Medical Journal and available here under their licensing/authorship rights listed here. A free download link to the published article is available here until January 12th 2016
Abstract
Objective
The aeromedical transfer of psychiatric patients with acute agitation is a regular requirement in only a few countries, with ours (Australia) as one of them. The optimal strategy has yet to be well described, ranging from physical restraints to general anesthesia with endotracheal intubation. In an Australian aeromedical service, Royal Flying Doctor Service (RFDS), Queensland Section (QLD), rates of endotracheal intubation required for patient management were retrospectively compared prior to and following implementation of a ketamine sedation protocol for this patient population
Methods
A systematic retrospective review was performed, utilizing 9 years of data in the RFDS QLD electronic database (2004 – 2013). Coding for mental health as primary diagnosis and intubation were search criteria.
Results
A total of 1478 patients were transferred during the study period, with 44 requiring intubation. This equates to intubation rates of 3.5% prior to protocol utilization, compared to 2.3% following protocol implementation.
Conclusion
In an Australian aeromedical service, implementation of a ketamine sedation protocol for management of the acutely agitated patient requiring air transfer has reduced the number of intubations in this patient group.
Introduction
The aeromedical transfer of psychiatric patients with acute agitation is a regular requirement in only a few countries, with ours (Australia) as one of them. Sedation of the agitated patient in the course of aeromedical transport is challenging due to the high degree of agitation that may exist, the large doses of sedative medications that may have been used prior to transport, and the risks involved if inadequate sedation is achieved during the flight. The optimal sedation strategy for the air transport of psychiatric patients remains unclear. At times, this has resulted in starkly divergent approaches taken by aeromedical providers ranging from use of physical restraints, or refusal to transport at all, to tracheal intubation and general anesthesia with chemical paralysis. Many patients with acute agitation can be transported safely using conventional benzodiazepine therapy. There is, however, a small subset of agitated patients who do not respond adequately to these first line sedating agents, and who require urgent air transport to progress their mental health care. In this situation, the resort to intubation and general anesthesia has often occurred despite its attendant risks.
The Queensland section of the Royal Flying Doctor Service of Australia has a total of 7 operational bases for aeromedical missions that cover an area the size of 1,852,642 km² – a combined territory equivalent to three times the land area of France. A population density of 2.70/km² means that long distance aeromedical retrieval is often warranted. It is not uncommon for transfer times of up to 3 hours with Far North Queensland.
Rural and remote communities rely upon the Flying Doctor for emergency and primary health care. When these remote sites have any residential health services at all, they are generally small community health centres staffed by remote-area nurses and visited by RFDS medical staff for several days each week. These clinics are not staffed after-hours, except for emergencies, and have no facilities to deal with acute presentations of major psychotic disorders. The exceptions are the small rural hospitals, which have several doctors and an after-hours ward, but no facilities for the acute mentally disturbed patient and no secure areas. As a result, even a single presentation of a psychotic or suicidal patient places great strain on the local resources, especially if they require constant restraint and supervision after-hours. Due to safety concerns, nationwide guidelines require transfer of all involuntary high-risk mental health patients to a facility with inpatient specialist mental health teams . Annually, an average of 161 patients with a primary mental health diagnosis require aeromedical transfer for acute assessment and management.
Where a patient is so acutely unwell that they are deemed a risk to themselves or others such that they require inpatient medical care or locked ward supervision, they are clearly a serious in-flight risk to aeromedical staff and the safety of the aircraft. Any patient that is deemed a risk to themselves or others such that they require transfer to a psychiatric facility is not, by definition, safe for travelling on an aircraft. As noted previously, management of these patients has varied greatly, up to and including intubation and chemical paralysis.
A recent meta-analysis has shown pre-hospital RSI is associated with first pass success rate of 90%. Unsuccessful endotracheal tube insertion can result in significant morbidity and mortality, such as esophageal intubation, hypoxia, and cardiac arrest. If a strategy avoiding resort to tracheal intubation could be implemented safely in the aeromedical setting, this could potentially improve overall patient care.
A ketamine sedation protocol was first introduced by Dr Minh Le Cong in Cairns RFDS Base in 2007. As a sedative of choice for prolonged pre-hospital psychiatric retrieval, ketamine has a number of unique advantages. The dissociative nature significantly reduces the in-flight risk to patient and staff. Long term review and more recent studies suggest that Ketamine may in fact be beneficial in acute suicidality and depression. Airway reflex retention and cardiopulmonary stability make this an ideal agent for use in austere environments with limited staff and possibly skill mix. A move towards pre-hospital RSI and procedural sedation has been advocated by a number of worldwide helicopter emergency medical services owing to the safety profile of Ketamine
After publication of a case series of 19 retrievals without adverse event, the protocol was rolled out across Queensland in 2010. Uptake was greatest in Cairns, Mount Isa and Charleville. These bases are manned by both RFDS medical and nursing staff. The other bases employ RFDS retrieval specialist nurses and outsource medical assistance to other retrieval companies such as Careflight.
Research Question
We had 2 objectives: (1) to compare the incidence of tracheal intubation rates before and after introduction of a ketamine sedation protocol for psychiatric patients requiring aeromedical transfer, (2) to compare the number of intubated patients between RFDS bases.
Methods
Study design
A retrospective analysis of the RFDS Queensland electronic database was performed, utilizing statistical data involving primary diagnosis of a mental health condition and the use of intubation and ventilation during aeromedical retrieval.
Any patient coded with a primary mental health diagnosis, in accordance with the International Classification of Diseases version 10, regardless of age, was included. The study timeframe covered a nine year period from Jan 2004 to December 2013, allowing for review of 3 years historical data, prior to and following introduction of the ketamine sedation protocol. Ethics approval for the study was granted by the Queensland Health Human Research Ethics Committee (Cairns, Queensland, Australia).
Those patients transferred that did not include a primary mental health diagnosis were excluded; for example, those intubated due to post-hanging airway obstruction resultant from their suicide attempt secondary to schizophrenia.
Results
A total of 1472 mental health patients were transported during the specified time period, a mean of 163 per year. Of these, 44 required intubation, or 4.9 per year. The total number requiring intubation was 44 or 3%.
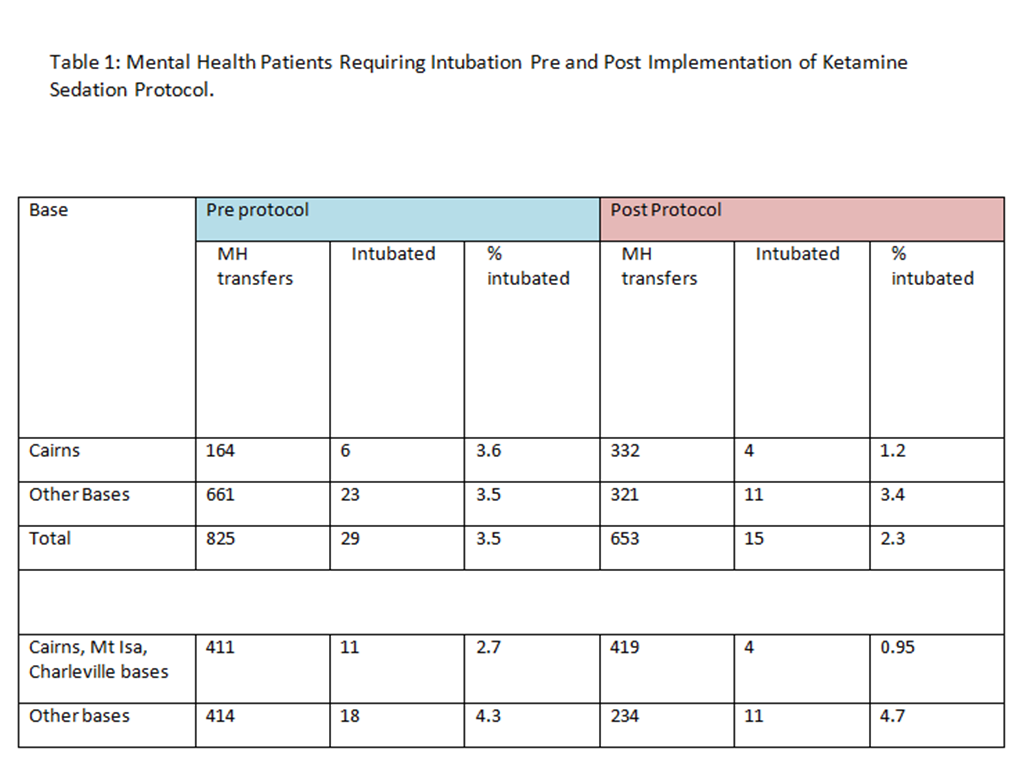
The breakdown and comparison of mental health (MH) patients transferred and the numbers requiring intubation can be found in Table 1. The table has been divided into pre and post protocol integration, with further delineation between bases that have resident RFDS doctors (Cairns, Mt Isa & Charleville) vs those without such doctors (Brisbane, Townsville, Rockhampton & Bundaberg). In the latter case, flight doctors are provided by Careflight Medical Services, working with RFDS flight nurses and pilots.
Cairns RFDS base implemented the Ketamine sedation protocol in 2007. It has consistently performed the highest number of psychiatric related aeromedical retrievals in Queensland, followed by the other bases.
Table 1: Mental Health Patients Requiring Intubation Pre and Post Implementation of Ketamine Sedation Protocol.
Discussion
To our knowledge, this is the largest review of ketamine sedation and tracheal intubation in mental health aeromedical retrievals to date.
Prior to implementation of the ketamine sedation protocol, the Cairns Base intubated 6 of 164 patients, and post 2007 (implementation), intubation for safe transfer was required in 4 of 332 retrievals, reflecting a reduction from 3.6 % to 1.2 %. This trend was noted in other bases staffed by RFDS doctors (Mount Isa, Charleville) after the 2010 rollout of the ketamine package. Cairns, Mount Isa and Charleville intubated 11 (or 2.7%) of 411 patients transferred pre- 2010. Post 2010, 419 patients were retrieved, with intubation rates reduced to 4 of 419 patients (or 0.95%).
Intubation rates have not changed in the bases without any resident RFDS doctors. , 18 of 414 patients transferred (or 4.3%) pre-protocol were intubated, while post-protocol, this actually rose to 11 intubations in 234 patients (4.7%). These bases are staffed with flight doctors from Careflight Medical Services, and adoption of the ketamine protocol was the slowest to be implemented in these bases.
The other significant aspect of this study is for the first time ever to our knowledge, a statistical benchmark key performance indicator for psychiatric aeromedical retrieval care can be extrapolated from this data. Tracheal intubation as a means of patient restraint has no known published data regarding the aeromedical setting, although it is a frequently utilized method anecdotally. The data suggests that a benchmark percentage of 5% of all aeromedical patients with a primary mental health diagnosis, be considered as the threshold for flagging inappropriate or excessive use of such a restrictive means of patient care. This study also suggests that it is feasible to achieve a performance of less than 3% reliance upon tracheal intubation, using a standardized ketamine sedation protocol.
Limitations of Study
This electronic database required accurate coding of entries. It is possible that not all cases were coded correctly. We cannot establish causality from this type of study i.e. other reasons for reduction in intubation rates post protocol. For example, increased awareness and focus on improving sedation care may have resulted in higher rates of adequate preflight oral sedation, leading to reduced arousal prior to air transfer and hence reduced requirement for deep sedation and tracheal intubation.
Recommendation and Implications for Emergency Medicine
Ketamine sedation has been successfully implemented in a large aeromedical patient population, reducing the need for intubation by half in those managed by RFDS medical staff. Inter-hospital Emergency department transfer of acutely agitated patients using a ketamine sedation protocol should be considered.
Conclusion
This study has demonstrated that in our setting, the implementation of clear guidelines and a protocol-based approach can reduce the number of intubations required for aeromedical retrieval of the acutely agitated mental health patient.
Further work
Future study could examine complication rates over this same study period
No competing interests are declared.
This study has in part been funded by the Flying Doctor Retrieval Sedation Registry by RFDS QLD.
Lahti AC, Warfel D, Michaelidis T, Weiler MA, Frey K, Tamminga CA. Long-term outcome of patients who receive ketamine during research. Biol Psychiatry. 2001 May 15;49(10):869-75.
Murrough JW, Charney DS. Cracking the moody brain: lifting the mood with ketamine. Nat Med. 2010 Dec;16(12):1384-5.
Ballard ED, Ionescu DF, Vande Voort JL, Niciu MJ, Richards EM, Luckenbaugh DA, Brutsché NE, Ameli R, Furey ML, Zarate CA Jr. Improvement in suicidal ideation after ketamine infusion: relationship to reductions in depression and anxiety. J Psychiatr Res. 2014 Nov;58:161-6.
Covvey JR, Crawford AN, Lowe DK. Intravenous ketamine for treatment-resistant major depressive disorder. Ann Pharmacother. 2012 Jan;46(1):117-23.
Scheppke KA, Braghiroli J, Shalaby M, Chait R. Prehospital use of im ketamine for sedation of violent and agitated patients. West J Emerg Med. 2014 Nov;15(7):736-41.
Jennings PA, Cameron P, Bernard S. Ketamine as an analgesic in the pre-hospital setting: a systematic review. Acta Anaesthesiol Scand. 2011 Jul;55(6):638-43.
Bredmose PP, Lockey DJ, Grier G, Watts B, Davies G. Pre-hospital use of ketamine for analgesia and procedural sedation. Emerg Med J. 2009 Jan;26(1):62-4.
Sibley A, Mackenzie M, Bawden J, Anstett D, Villa-Roel C, Rowe BH. A prospective review of the use of ketamine to facilitate endotracheal intubation in the helicopter emergency medical services (HEMS) setting. Emerg Med J. 2011 Jun;28(6):521-5.
Mental Health Act 2000, http://www.health.qld.gov.au/mha2000/ Pritchard A, Le Cong M. Ketamine sedation during air medical retrieval of an agitated patient. Air Med J. 2014 Mar-Apr;33(2):76-7.
Lossius HM, Røislien J, Lockey DJ. Patient safety in pre-hospital emergency tracheal intubation: a comprehensive meta-analysis of the intubation success rates of EMS providers. Crit Care. 2012 Feb 11;16(1):R24.
von Vopelius-Feldt J, Benger JR. Prehospital anaesthesia by a physician and paramedic critical care team in Southwest England. Eur J Emerg Med. 2013 Dec;20(6):382-6
Davis DP, Dunford JV, Poste JC, Ochs M, Holbrook T, Fortlage D, Size MJ, Kennedy F, Hoyt DB. The impact of hypoxia and hyperventilation on outcome after paramedic rapid sequence intubation of severely head-injured patients. J Trauma. 2004 Jul;57(1):1-8; discussion 8-10.
Bernard SA, Nguyen V, Cameron P, Masci K, Fitzgerald M, Cooper DJ, Walker T, Std BP, Myles P, Murray L, David, Taylor, Smith K, Patrick I, Edington J, Bacon A, Rosenfeld JV, Judson R. Prehospital rapid sequence intubation improves functional outcome for patients with severe traumatic brain injury: a randomized controlled trial. Ann Surg. 2010 Dec;252(6):959-65.
Le Cong M, Gynther B, Hunter E, Schuller P. Ketamine sedation for patients with acute agitation and psychiatric illness requiring aeromedical retrieval. Emerg Med J. 2012 Apr;29(4):335-7.
PHARM PODCAST 112 : So that others may learn, so that others may live – Martin Bromiley & Nicholas Chrimes
Dec 13, 2014
Hi Folks
On today’s show, we chat to our good friends Martin Bromiley and Nicholas Chrimes. They have collaborated to make two new medical education videos to help highlight issues around management of the unexpected difficult airway. They are works of fiction based on the real world event of the death of Martin’s first wife, Elaine Bromiley during an elective operation. Martin established the Clinical Human Factors Group in 2007 to help promote the issue of human error and patient safety in clinical medicine. In 2014, he was awarded the Difficult airway Society Medal in recognition of his work in advancing the study and teaching of non technical skills in anaesthesia and airway management.
Right Click and Choose Save-as to Download the Podcast.
GET FOAMEd rural masterclass session : Spotting the Crook!
Nov 04, 2012
Hi folks!
We have an idea for another FOAMEd educational series..its called GET FOAMEd ( Generalist Education & Training via Free Open Access Meducation)
Our intent is to aim it at the rural generalist doctor, remote nurse or paramedic, or if you are working in remote areas and need to make do with less toys and resources. I know we have lots of listeners from rural and remote Canada, USA and Europe.
For the first episode we decided to talk on Spotting the Crook! This is a very peculiar Australian vernacular term, which essentially means identifying the deteriorating and critically ill patient at an early stage. Crook is Australian for sick, not criminal! We might introduce our international listeners to other weird Australian terms , as we progress through the series!
PHARM Podcast 32 : Dr Brian Burns and a pitlane DSI case
Aug 07, 2012
Brian and I do a quick case presentation on DSI and retrieval medicine human factorsHi there.
Remember Brian, awesome Irish emergency physician, prehospital and retrieval consultant specialist and mate of Cliff Reid, Karel Habig and the greater GSA HEMS team in Sydney?
He is back!
We talk about a recent DSI case he performed last week where a team approach to airway management in the high risk patient led to successful safe airway intervention.
Also I review a short correspondence in the July edition of Anaesthesia and Intensive care by the GSA HEMS team on their new difficult airway intubation technique using an Ambu Ascope disposable endoscope and iGel supraglottic airway and trauma shears!
Right Click and Choose Save-as to Download the Podcast.
PHARM Podcast 31 : ED chronic pain management
Aug 03, 2012
Seth and I do a quick overview of the challenges of managing chronic pain presentations in the EDHi there. A week ago, we read a tweet about the challenges of managing chronic pain presentations to the ED. I thought it was worthwhile having a discussion of the options in dealing with such presentations. What we discuss:
Harm minimisation strategy with limited prescribing
Alternatives to opioids
General approach to pain in the ED
Systems in Australia and US to monitor drug addiction and seeking prescription drugs for illicit sale
Right Click and Choose Save-as to Download the Podcast.
PHARM Podcast 30 : Respiratory Therapy Profession with Sean Marshall
Aug 02, 2012
This is Sean, a Canadian respiratory therapist. Tune in and learn about his profession!
Hi folks! This interview I talk to Sean Marshall, a respiratory therapist in Ontario, Canada. We do not have this profession in Australia and I believe it is mainly in North America and Canada. So I wanted to learn more about it and the training and daily role these RTs provide.
Things we discuss :
RT training
RT daily routine and duties
RT scope of practice
Hypothetical severe asthma case in ED and role of RT within the ED resuscitation team
Critical care air transport and RT role
The ideal transport ventilator
Why RT profession and other non doctor professions may have trouble establishing themselves in Australia
Sean provided some commentary and reference link below:
Hi Minh,
This article may be an appropriate citation, I’ll let you be the judge.
There are many studies such as this one. They are often used to advocate that ventilator management by a Respiratory Therapist following a protocol achieves better success than physician’s managing the ventilator. I support this view but feel it is a bit of an extrapolation from the actual findings of the studies to say one group of professionals does a better job than another.
Although I can’t seem to find a good reference, I would also make the following pitch for RTs: During a night shift in hospital, it is often a single physician responsible for the medicine wards. It may be a Resident or specialist Attending that does not have a great deal of experience with critical care and airway management. I feel that especially at times of day when staffing is less, that a Respiratory Therapist brings experience and confidence to airway management and ventilation, allowing the physician to step back and lead the whole team through a resuscitation. I feel this is a safer model of care than requiring the MD to simultaneously take in all the facts and lead an effective resuscitation while at the same time searching for vocal cords to pass a tube or initiating mechanical ventilation. And if you staff multiple physicians to address that situation, RTs can fill the need more cost-effectively.
I understand it’s political, but I felt compelled to advocate for my profession.
Thanks again,
Sean
Minh here – Sean, I agree with you. Its not about egos in airway management and frankly I dont really care who sticks the plastic past the cords as long as they do it safely and defend oxygenation at all times. The lone wolf attitude to critical care airway procedures and ventilation must be culturally displaced and a team approach adopted where the doctor maybe best utilised as a team leader if appropriately skilled and confident to act in such a role. Operational silos of clinical practice do not help patient safety and quality of care and we should all be sharing skills, knowledge and experience rather than defending professional territories.Rant ends
Right Click and Choose Save-as to Download the Podcast.
PHARM Podcast 015 – MICA Service of Victoria with Flight Paramedic Ben Meadley
Jun 03, 2012
Flight Paramedic Ben Meadley(middle back of picture) tells us about MICA Victoria
Hi folks! Ben Meadley has a great prehospital blog. He is proud of his service, MICA Victoria. Things that we talk about during the interview are Adult Retrieval Services in Victoria ( ARV), check out the weblink for some fantastic resources on retrieval medicine! We discuss the training of a MICA paramedic and here is a great presentation from a MICA Flight team manager, Anthony De Wit, on the outdoor training aspects. Prehospital research trials are discussed and references to these can be found on Ben’s blog article, CHILLOUT. I mention iSOBAR clinical handover tool and I recommend you all check it out. The key to prehospital and retrieval medicine is effective communication.
During the case scenario, we discuss management of status epilepticus and I mention ketamine. Here are some references for its use in refractory seizures.
Right Click and Choose Save-as to Download the Podcast.
King Vision Video Laryngoscope intubation with DuCanto
May 27, 2012
King Vision Video laryngoscope wielded by Master DuCanto
A short sharp video demonstrating the overhand technique and speed of intubation in a large patient with the King Vision video laryngoscope
Note how Jimmy does not even change the overhand grip and proceeds to pass the tube down the guide channel with his right hand. This takes some practice as most operators are used to inserting a laryngoscope blade like the familiar Macintosh with the “holding a beer can” grip position.
Also note the gas analyser display at the bottom of the screen showing inspired and expired O2 levels and the first reading appearing after intubation of an expired O2 of 94%, indicating adequate prexoygenation prior to intubation attempt.
Minh
Novel Hybrid Airway technique with Dr Jim Du Canto
May 21, 2012
Jimmy D is back with more videos on intubation via a supraglottic airway and a really novel twist!
Jimmy excels once again in his passion for demonstrating novel and resilient airway management techniques. Here are two videos taken in his elective OR list. All videos we post have been consented by the patients for medical education purposes. Come and spend a session in JImmy’s OR!
Incredible stuff, right? Whats so novel about what you just saw?
1.The LMA Unique utilised as the supraglottic airway is almost ubiquitous in one form or another. It is essentially a disposable version of the original LMA Classic. In other words almost everywhere that needs to provide emergency airway management will have one
2.Note the swivel connector used to attach ventilator circuit and insert bougie. Find one of these cheap connectors and keep it in your pocket. Scott Weingart has a nice description of using one of these here for suctioning during direct laryngoscopy. This connector will allow you to continuously ventilate during bougie insertion as well with this hybrid airway technique Jimmy demonstrates.
3.Note the gas analyser monitor on the videos and the Inspired and Expired values. This is what Jimmy talks about in using much more accurate “barometers” of adequate ventilation. If your expired O2 is > 94%, you have a large reservoir of oxygen sitting in your lungs = lots of safety during apnoea
4. The CrankShaft MAneuver I am going to name the DuCanto maneuver but this was his novel solution to a problem we encountered in testing this technique. As the bougie exits the LMA, it enters the larynx at an acute angle and hits the anterior wall of the tracheal entrance. There are a number of things you can do like withdrawing the LMA to make the exit angle less acute but this crankshaft maneuver works well too. I tried it out on a Frova intubating bougie which is hollow and it did not work so well as the haemostat crushed the bougie shaft and made it difficult to rotate. A solid bougie like the Portex one Jimmy uses in the video is recommended.
5. I call this novel hybrid concept the Mount Everest strategy of emergency airway management. If you were to consider how one might tackle the highest mountain in the world, you should realise that altitude related hypoxia is the big killer in this situation. Just like it is for our critical airway patients. How do the experienced climbers tackle Mt Everest? They lay siege to the mountain, establish base camps and higher rest camps with a staged approach of acclimatisation. Any attempts to rush this time honored process are often fraught with disaster and high risk. Similarly in our high risk hypoxic patients we need to lay siege to enemy hypoxia, establish a base camp of reliable and secure oxygenation ( preoxygenation) then setup our first stage of the climb ( by inserting a LMA or SGA). This gets us closer to the summit but allows for reoxygenation and breathing space to make the next staged ascent. Of course you can just try to intubate as quickly as possible, or using the climbing analogy, try to summit in one ascent. Thats possible but is it safe, is it acceptable risk? Not so sure…
Hope you airway interested providers out there have enjoyed this episode as much as I have.
Send in your comments and please thank Jimmy for all this work he is doing to educate us all on his discovery and exploration of resilient airway techniques to assist the emergency provider
regards
Minh
Bougie assisted intubation via SGA with Dr Jim Du Canto
May 16, 2012
Jimmy D is back with a video on intubation via a supraglottic airway but with a novel twist!
SO what you say? Bougie assisted intubation via a LMA has been done before..sure thing. But what have we added or described further here …? See for yourself. Will this technique spell the death of RSI as we know it?
Incredible stuff, right? Whats so novel about what you just saw?
1. Almost all the airway gear shown is commonly available in every ICU, ED , OT or prehospital EMS service
2. The use of a swivel endoscopic connector allows for continuous ventilation throughout the procedure
3. Adding a video laryngoscope or optical stylet is the most expensive part of the whole technique but allows you to use the device alone or combined in this hybrid technique of SGA and VL assisted bougie intubation
4. This technique allows a SGA device to be exchanged for an ETT, during CPR for example.
NEXT EPISODE, AN INTERVIEW WITH DR DARREN BRAUDE ON THE RAPID SEQUENCE AIRWAY CONCEPT OR RSA
DASH -1A Emergency Airway Concepts with Dr Bill Hinckley
May 14, 2012
Hi folks, Dr Bill Hinckley, sent me an awesome audio powerpoint recording on DASH -1 A emergency airway concept
Wild Bill has some great ideas on emergency airway management and he has formulated them into a concept he has coined DASH-1A. What is it? Well check it out here for download and your viewing and listening pleasure! (50Mb file)
Stay safe and enjoy the presentation! Minh Le Cong, Flying Doctor Down Under
PHARM Historical Case Studies
May 06, 2012
A tale of two traumas, two women, two continents and two approaches to prehospital care.
Introduction
In 1996, Lady Diana was in a serious car crash at over 85mph in a Paris tunnel. She and her bodyguard were the only survivors, on arrival of the French prehospital services within twelve minutes. She arrested on extrication and had to be resuscitated by a prehospital doctor. Despite clearly a critical traumatic arrest, it took over ninety minutes from the time of the accident to arrival at the trauma hospital a few miles away. In the ambulance ride, a dopamine infusion was started after the arrest to treat hypotension. The ambulance was stopped during the transport, due to a drop in blood pressure and the dopamine infusion adjusted. Lady Diana died despite all efforts from exsanguinating thoracic injury to left pulmonary vein. Her bodyguard was the sole survivor and was the only one wearing a seat belt.
In early 2011, Senator Giffords was shot in the head with a 9mm pistol at close range during a community event at a shopping centre in Tucson, Arizona. Her intern rendered immediate first aid. Prehospital services arrived within ten minutes of the shooting. Paramedics quickly triaged Giffords to a rapid road transport to the nearest trauma hospital and she arrived there and was undergoing a decompressive craniectomy within thirty eight minutes from wounding. She survived the assassination attempt and made a steady recovery and paid tribute to those killed that day, at the one year anniversary ceremony in 2012.
Discussion
Two prominent women , on two different continents, suffering life threatening trauma with two very different prehospital systems of care. One doctor based, utilising specialist doctors and nurses in mobile intensive care units, the other paramedic based. One strategy of bringing the emergency room care to the patient, versus the other of transporting the patient quickly to the emergency room. Of the two victims of trauma here, one survivor. Did rapid transport make the difference here? What are the lessons if any that can be gleaned from comparing these two trauma cases and the optimal prehospital care for the critically injured?
Its a complex question and in the past has been oversimplified by the expression : Scoop and run or stay and play?
If one were to argue that clearly Senator Giffords case demonstrates the superior North American prehospital strategy of rapid transport for severe trauma versus trying to provide advanced resuscitation procedures at the scene, then the pitfalls of such an approach need to be highlighted. Gifford’s intern is credited with saving her life by providing immediate haemorrhage control and airway clearance. Without this , no matter how quick the transport, she would have likely died. So clearly there are life saving interventions that need to be done as soon as possible.
The longer the transport time, the more need of early and ongoing critical care resuscitation for the critical trauma patient. For example if the shooting had occurred on a cruise ship in the middle of the Pacific and helicopter retrieval was going to take several hours, then no one would question the need to provide early advanced airway support and ventilation and perhaps even resuscitative surgical interventions under remote guidance/advice.
Take home messages
Basic trauma first aid might be more effective than a dopamine infusion in the haemorrhaging trauma patient
If you are in Paris or Tucson and suffer a critical injury, it might be better to get to a trauma hospital within twelve minutes, than ninety minutes
There is no one size fits all answer to severe trauma
 Stay Connected
Stay Connected
















")