The Clinical Problem Solvers is a multi-modal venture that works to disseminate and democratize the stories and science of diagnostic reasoning
Twitter: @CPSolvers
Website: clinicalproblemsolving.com
Episode 452: The Clinical Unknown Series – Young lady with dizziness
Mar 27, 2026
https://clinicalproblemsolving.com/wp-content/uploads/2026/03/CUS-March-post-post-prod.wavStep into a new chapter of the Clinical Unknown Series, where each case is a riddle eager to catch you off guard. This time, Academy member Ethan from Taiwan brings forth a perplexing case: a young woman whose dizziness unravels into the extraordinary. Mark, Debora, and Noah scramble to reveal the twist hidden deep within this medical enigma.
Episode 451: WDx #41: Burnout, Existential Dread, and Everything in Between
Mar 18, 2026
For this episode of WDx, Sharmin and Kaylin are joined by Dr Alice Mao to discuss what they have learned about burnout so far and how their perspectives have changed over time. Alice Mao’s Bio:Dr. Alice Mao is an internal medicine and geriatric medicine physician who is passionate about social equity, community empowerment, and innovations in primary care. She was born in China and grew up in Canada and the US. She completed medical school at UCSF, internal medicine residency at the University of Washington, and geriatric medicine fellowship at Stanford. She is currently the Lead Geriatrician at Asian Health Services, where she is helping build a new geriatric clinic and a new Program of All-Inclusive Care for the Elderly (PACE) to better serve high frailty seniors in the community. Outside of medicine, she enjoys spending time with family and friends, giving her cat cheek scratches, and resurrecting her childhood dreams of learning how to freestyle dance. https://clinicalproblemsolving.com/wp-content/uploads/2026/03/WDx-3.19.26-final.m4a
Noah presents a case about AKI. Tune in to listen how Maddy, Youssef, and Mark build their AKI differential diagnosis and work through the pivot points in this interesting case!
Youssef, Alec, and Ann Marie head to Southern SGIM in New Orleans and discuss two clinical unknowns on the stage! Cases presented by Joel Cohen & Huda Dagra.
To join us live on Virtual Morning Report (VMR), sign up HERE.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Zakariyya presents a case of acute psychiatric disturbance and tremors to Sebastian.
Zakariyya is a medical doctor from South Africa with a strong passion for internal medicine, neurology, and clinical reasoning. He thrives on tackling complex diagnostic challenges and is committed to lifelong learning. He is the founder of The Study Doc, a platform dedicated to teaching evidence-based study strategies and learning science to help students and junior doctors succeed. He is deeply committed to medical education and is excited to contribute to theCPS Academy community.
Sebastian Green @sebfgreen
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA). He was born and raised in London, England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has published on neuroimaging, memory, sleep, epilepsy, and more. He is passionate about medical education in neurology, and using EEG to answer big questions about the brain. In his free time you will find him hiking in the Santa Monica mountains
To join us live on Virtual Morning Report (VMR), sign up HERE.
Episode 442: WDx #40: Clinical Unknown with Kassidy and Dr. Ann Marie Kumfer
Feb 04, 2026
Kaylin, Sharmin, and Cheryl are joined by Kassidy Lovins, MS3, and Ann Marie Kumfer, MD, to discuss a case of a 35-year-old man with fevers, diffuse myalgias, and weakness.
Bio:Kassidy Lovins is a third-year student at UNC School of Medicine, approaching the end of her clinical rotations and exploring a future in Internal or Family Medicine. She has a strong interest in clinical reasoning and enjoys working through complex patient cases. Outside of medical school, Kassidy serves as a Transportation Officer in the North Carolina National Guard, which has given her a strong appreciation for teamwork and problem-solving. She lives in North Carolina with her husband, puppy, and cat and is expecting her first child. https://clinicalproblemsolving.com/wp-content/uploads/2026/02/WDx-2.5.26-actual-final-2_3_26-7.50-PM.m4a
RR discussed a case presented by Shantanu Rai involving a young woman with four months of fever. The case is adapted from a novel written by Shantanu Rai.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Andrew presents a case of bilateral leg weakness to Sarah and Valeria.
Andrew is a rising hospitalist-educator at Beth Israel Deaconess Medical Center. Meeting inpatients and working with them to achieve diagnostic clarity is his primary clinical passion, and his interest in diagnosing the undifferentiated patient is the driving force behind deep interest in learning and teaching diagnostic reasoning. On X/Twitter), he is known for creating and sharing schemas for both common and uncommon clinical dilemmas, and he is currently developing a new podcast space for Dx enthusiasts: Diagnostic Atypia.
Sarah K Blaine
@sarahkblaine
Sarah Blaine is an MD/MSc student at Emory University School of Medicine applying into neurology residency. She is from Southern California and went to UC Berkeley for her undergraduate degree where she studied Molecular Biology with an emphasis in Immunology and Pathogenesis. Her research interests are in antibiotic resistance, epidemiological modeling, and predicting outcomes in critical illness. She loves going to concerts, rock climbing, and playing with her dog, Pluto.
Valeria Roldan
(@valeroldan23)
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
To join us live on Virtual Morning Report (VMR), sign up HERE.
Ring in the New Year with a fresh episode! Join Debora, Mark, and Noah in the latest Clinical Unknown Series as they unravel a puzzling case together. Let’s start the year learning!
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Sarah presents a case to Sebastian and Vijay.
Sarah Blaine (@sarahkblaine)
Sarah Blaine is an MD/MSc student at Emory University School of Medicine applying into neurology residency. She isfrom SouthernCalifornia and went to UC Berkeley for her undergraduate degree where she studied Molecular Biologywith an emphasis in Immunology and Pathogenesis. Her research interests are in antibiotic resistance, epidemiologicalmodeling, and predicting outcomes in critical illness. She loves going to concerts, rock climbing, and playing with herdog, Pluto.
Dr. Vijay Balaji (@vijaybramhan)
Vijay was born and raised in Bangalore, India. He is currently a Pulm-Crit fellow at AIIMS Jodhpur. He is passionate about clinicalreasoning, medicaleducation, EKG, POCUS and teaching. Outside of medicine he enjoys contemplating Indian philosophy, cooking and playing basketball.
Dr. Sebastian Green ( @sebfgreen )
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA). He was born and raised in London, England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has published on neuroimaging, memory, sleep, epilepsy, and more. He is passionate about medical education in neurology, and using EEG to answer big questions about the brain.
Episode 430: WDx #39: Clinical Unknown with Drs. Kuchal Agadi and Ann Marie Kumfer
Nov 13, 2025
In this episode of WDx, Cheryl, Kaylin, and Sharmin are joined by Kuchal and Ann Marie, two wonderful members of the CPSolvers Academy. Kuchal presents a case of a young man with fevers to Ann Marie and Sharmin.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Dr. Yousuf Patel presents a case of diplopia and fever to Vale and Sebastian.
Yousuf Patel
Dr. Yousuf Patel is currently a resident in neurology in Cape Town, South Africa. He completed his undergraduate training at Stellenbosch University. He holds post graduate qualifications in emergency medicine, occupational medicine, and travel medicine. In addition to this he also attained a BA in Philosophy & Sociology, and a masters equivalent in theological studies. His work experience includes sports medicine, emergency medicine, maritime medicine, and relief medicine where he has been able to travel to various regional and international relief sites. Other than his interests in neuroscience, physical health, and health equity, he is passionate about ethics and metaphysics.
Valeria Roldan (@valeroldan23)
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Dr. Sebastian Green ( @sebfgreen )
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA). He was born and raised in London, England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has published on neuroimaging, memory, sleep, epilepsy, and more. He is passionate about medical education in neurology, and using EEG to answer big questions about the brain.
Episode 29 – Clinician Burnout, Racial Health Inequities, and Reincorporating Rest into the Profession
Show Notes by Asya Pitre
October 29, 2025
Summary: In this episode, hosts Ashley Cooper and Sud Krishnamurthy sit down with Dr. Kriti Prasad and Dr. Khaalisha Ajala to talk about the heavy toll of clinician burnout, how it intersects with racial inequities in healthcare, and why reclaiming rest needs to be treated as both a personal and systemic priority. Together, they explore how exhaustion, moral injury, and structural racism are intertwined, and how these forces not only affect providers but also shape patient outcomes. The conversation explores both big-picture policy ideas and practical steps for everyday advocacy and healing.
Timestamps:
0:00 Introductions
2:30 Origin Stories
9:07 Research Study of Burnout in Healthcare Workers
14:05 Advocating for and Humanizing Patients
22:07 COVID-19 Pandemic’s Impact on Clinician Burnout
28:19 Research: The Blueprint for Overcoming Burnout Exists
34:00 Policies to Ameliorate Clinician Burnout
39:08 Destigmatizing Mental Health Among Healthcare Workers
48:00 Nonprofit organization: A Tribe Called Health
56:00 Closing Remarks
Credits
Written and produced by: Ashley Cooper, Sudarshan Krishnamurthy, and Team
Hosts: Ashley Cooper and Sudarshan Krishnamurthy
Infographic and Audio Edits: Ashley Cooper
Show Notes: Asya Pitre
Guest: Dr. Kriti Prasad & Dr. Khaalisha Ajala
Guest Biographies:
Dr. Kriti Prasad is an Internal Medicine and Primary Care Resident at Boston Medical Center and volunteer faculty at the Boston University Chobanian & Avedisian School of Medicine. Her research focuses on clinician stress and burnout, antiracism in medical education, and trauma-responsive care. She hopes to practice as a primary care and palliative care physician in safety-net settings.
Dr. Khaalisha Ajala is an Assistant Professor of Medicine at Emory University and Assistant Site Director of Education for Hospital Medicine at Grady Memorial Hospital. A leader in DEI initiatives, she has built mentorship programs for underrepresented students, is a global health educator, and is founder of A Tribe Called Health, a nonprofit blending hip-hop culture with health advocacy.
Episode Takeaways
Dr. Prasad and Dr. Ajala share how their personal journeys, families, and communities drew them into medicine and continue to inspire their advocacy.
Dr. Prasad’s research reveals that nearly half of healthcare workers experienced burnout during the pandemic, with women, Black, and Latinx clinicians reporting higher rates of burnout. Traditional measures of burnout may not capture the unique challenges faced by minoritized providers.
Both guests highlight how implicit bias can show up when clinicians are stretched thin, and how advocacy at the bedside and through our notes can counteract harm. Exhaustion and moral injury ripple outward, influencing not just clinician well-being but also patient care and health inequities.
The COVID-19 pandemic exposed deep issues in our healthcare system and left lasting trauma for providers.
Dr. Ajala shares how her nonprofit, A Tribe Called Health, reflects the intersection of her passions for hip-hop and medicine.
From reducing administrative burdens and strengthening resident unions to normalizing mental health support, the guests underscore the importance of systemic change. On a more personal level, they emphasize building community, incorporating wellness into training, and helping clinicians reconnect with the “North Star” that first called them to medicine. Honoring your humanity is a form of advocacy for yourself and your patients.
Lawrence, J. A., Davis, B. A., Corbette, T., Hill, E. V., Williams, D. R., & Reede, J. Y. (2021). Racial/Ethnic Differences in Burnout: A Systematic Review. Journal of Racial and Ethnic Health Disparities, 9(1), 257. https://doi.org/10.1007/s40615-020-00950-0
Khullar, D., Prasad, K., Neprash, H., Poplau, S., Brown, R. L., Williams, E. S., Audi, C., & Linzer, M. (2022). Factors associated with patient trust in their clinicians: Results from the healthy work place study. Health Care Management Review, 47(4), 289–296. https://pubmed.ncbi.nlm.nih.gov/35170482/
LeClaire, M. M., Poplau, S., Prasad, K., Audi, C., Freese, R., & Linzer, M. (2019). Low ICU burnout in a safety net hospital. Critical Care Explorations, 1(5), e0014. https://pmc.ncbi.nlm.nih.gov/articles/PMC6927682/
Prasad, K., McLoughlin, C., Stillman, M., Poplau, S., Goelz, E., Taylor, S., Nankivil, N., Brown, R., Linzer, M., Cappelucci, K., Barbouche, M., & Sinsky, C. A. (2021). Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: A national cross-sectional survey study. eClinicalMedicine, 35. https://doi.org/10.1016/j.eclinm.2021.100879
Prasad, K., Poplau, S., Brown, R., Yale, S., Grossman, E., Varkey, A. B., Williams, E., Neprash, H., Linzer, M., & for the Healthy Work Place (HWP) Investigators. (2020). Time Pressure During Primary Care Office Visits: A Prospective Evaluation of Data from the Healthy Work Place Study. Journal of General Internal Medicine, 35(2), 465–472. https://doi.org/10.1007/s11606-019-05343-6
The hosts and guests report no relevant financial disclosures.
Citation
Ajala K, Prasad K, Krishnamurthy S, Cooper A, Pitre A, “Episode 29: Clinician Burnout, Racial Health Inequities, and Reincorporating Rest into the Profession” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. October 29, 2025.
Maddy presents a fascinating case of dyspnea with diffuse ground-glass opacities. Tune in as Mark, Youssef, and Noah work through the diagnostic puzzle.
In this new episode, Rabih shares an important case with Debora, Mark, and Noah. We invite you to listen and join in on their journey as they work together to discover the final diagnosis.
To join us live on Virtual Morning Report (VMR) or to present a case to us, sign up here.
Episode 422: WDx #38: Clinical Unknown with UCLA Cardiology fellows
Oct 02, 2025
Kaylin and Sharmin were joined by UCLA Cardiology fellows, Drs. Rachel Ohman and Angela Duvalyan, to discuss a case of a 49 year old woman with acute chest pain.
Angela Duvalyan, MD is a second year Cardiology Fellow at University of California, Los Angeles (UCLA). Her clinical interests include interventional cardiology, medical education, and clinical trials. Dr. Duvalyan earned her M.D. from Keck School of Medicine of USC and completed her Internal Medicine Residency and Chief Residency at UTSW. In her spare time, she loves taking her puppy on hikes, hosting charcuterie nights, or unwinding at a fitness class.
Rachel Ohman, MD is an ocean lover from San Diego who grew interested in medicine while an undergraduate at the University of Chicago. She explored the integration of research, clinical care, and health disparities during a two-year-long research fellowship at the NIH. She then returned home to California for medical school and residency training at UCLA, after which she nurtured her passion for medical education as a chief resident. She is now a third-year cardiology fellow at UCLA and remains particularly interested in cardio-oncology, heart failure, health equity, and clinical reasoning. Outside of the hospital, she enjoys hiking and spending time at the beach with her husband, toddler daughter, and Rhodesian Ridgeback.
Episode 421: Baby on Board – and a surprise guest! Listen to Greg and Bobby discuss how to manage the guest tagging along for the ride!!
Sep 18, 2025
Case Presenter:
Anna Jarvis, MD
Anna Jarvis is a current 3rd year OB/GYN resident at Johns Hopkins. She is originally from California, where she completed her MD at University of California, Irvine. She is currently applying to Maternal Fetal Medicine Fellowship this cycle! Case Discussant
MFM Fellow – at University of Pennsylvania
Greg is a current first year Maternal-Fetal Medicine fellow at the Hospital of the University of Pennsylvania with a particular interest in pharmacology and metabolism in pregnancy. Before fellowship, I attended undergrad at Princeton University before completing an MD/PhD at Stony Brook University in New York with a PhD in molecular pharmacology and then completing residency training in Ob/Gyn at Johns Hopkins Hospital in Baltimore. Teaching and clinical reasoning are passions of mine, and I continue to teach and mentor students from the undergraduate to medical student and resident level. In my free time, I enjoy reading, running, and traveling with my wife.
Episode 25 – Immigrant and Refugee Health: Live from SGIM 2025: Best of Antiracism Research at the Society of General Internal Medicine’s Annual Meeting
Show Notes by Alec J. Calac
September 15, 2025
Summary: This episode highlights a selection of antiracism research presentations at a live recording of the podcast at the 2025 Society for General Internal Medicine (SGIM) Annual Meeting. This year’s episode, our fifth conducted at SGIM, is focused on immigrant and refugee health. During this episode, we speak with experts Dr. Harita Shah, an internal medicine/pediatrics specialist at the University of Chicago who has conducted extensive community-engaged participatory research, Dr. Masha Slavin, an internist and Director of Primary Care for Bellevue’s Program for Survivors of Torture, and Dr. Sarah Kimball, an Associate Professor at Boston University Chobonian and Avedisian School of Medicine and Director of the Immigrant and Refugee Health Center (IRHC) at Boston Medical Center. This episode is hosted by Asya Pitre and Ashley Cooper. The show notes for this episode were written by Alec Calac.
Important Note: This episode represents the views of the podcast participants and is not necessarily representative of the institutions at which they work and practice.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Understand how xenophobia and racism (at the interpersonal, institutional, and structural levels) impact the health experiences of immigrant and refugee populations.
Evaluate how community-based participatory research plays a pivotal role in providing comprehensive care to immigrant and refugee populations.
Identify critical points of intervention (including decreasing linguistic barriers, utilizing a trauma-informed approach, and promoting an inclusive environment) to bolster health outcomes amongst immigrant and refugee communities.
Credits
Written and produced by: Ashley Cooper, MS, MPhil; Asya Pitre, DO; Alec Calac, PhD
Hosts: Asya Pitre, Ashley Cooper
Infographic: Ashley Cooper
Audio Edits: Ashley Cooper
Show Notes: Alec Calac
Guests: Dr. Harita Shah, MD, Dr. Sarah Kimball, MD & Dr. Masha Slavin, MD
Speaker Biographies:
Dr. Masha Slavin, MD, is a primary care physician at Bellevue Hospital, a large public hospital in New York City, and a Clinical Assistant Professor in the Department of Medicine at the NYU Grossman School of Medicine. In her role as the director of primary care for Bellevue’s Program for Survivors of Torture, she works with a multidisciplinary team of behavioral health, legal, and social work colleagues in caring for people who have experienced human rights violations. Her particular interests are in medical education on immigrant health, with the goal of improving clinicians’ comfort level in caring for this patient population and in improving workflows that facilitate care. She also enjoys working with medical students as an advisor to the NYU Grossman School of Medicine’s Asylum Clinic.
Dr. Harita Shah, MD, is a med-peds primary care physician and an Assistant Professor in General Internal Medicine at the University of Chicago. Dr. Shah trained at the Johns Hopkins School of Medicine and the Urban Health Medicine-Pediatrics residency program. Her research focuses on the combination of community-based participatory research (CBPR) and implementation science to improve access to preventive care for underserved populations. She has directed 3 community-engaged public health campaigns, including most recently the PrEPárate campaign promoting access to PrEP among Latino/a/e sexual and gender minority individuals in Chicago (preparate.info). Her current research includes a community-driven project to understand best practices for serving Latinx populations, with a goal of informing health equity initiatives.
Dr. Sarah Kimball, MD, is a board-certified internist and is an Associate Professor at Chobanian and Avedisian School of Medicine. She completed her medical school training at Harvard University Medical School and did residency training in Internal Medicine at the Brigham and Women’s Hospital Residency Program. Dr. Kimball has expertise in immigration-informed medical care, where she has helped to research and build health systems that are responsive to the needs of im/migrant patients. She is currently the Director of the Immigrant & Refugee Health Center (IRHC) at Boston Medical Center, a comprehensive medical home that addresses the barriers that immigrants face to being holistically healthy.
Radl-Karimi, C., Nielsen, D. S., Sodemann, M., Batalden, P., & von Plessen, C. (2022). “When I feel safe, I dare to open up”: Immigrant and refugee patients’ experiences with coproducing healthcare. Patient Education and Counseling, 105(7), 2338–2345. https://doi.org/10.1016/j.pec.2021.11.009
Shah, H. S., Serrano, P. A., Rodriguez-Diaz, C. E., Page, K. R., Ross, J., Wilson, S. M., & Cantos, V. D. (2025). Not a Monolith: Regional HIV Implementation Science Lessons With Latino/a/x Populations. JAIDS: Journal of Acquired Immune Deficiency Syndromes, 98(5 Suppl), e98–e103. https://doi.org/10.1097/QAI.0000000000003611
The PrEPárate Campaign. (n.d.). PrEP for You & Me. The PrEPárate Campaign. Retrieved August 1, 2025, from https://www.preparate.info/
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Kimball S, Shah H, Slavin M, Pitre A, Cooper A, Krishnamurthy S, Calac A. “Episode 28: Live from SGIM 2025: Best of Antiracism Research at the Society of General Internal Medicine’s 2025 Annual Meeting” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. September 15, 2025.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Jeffrey presents a case of headache and diplopia to Vale and Sebastian.
Jeffrey is an academic rheumatologist whose early love for guessing TV plot twistswith his parents sparked a lifelong passion forclinical problem solving. He is especially drawn to caring for misunderstood patients, striving to offer empathetic and thoughtful care. Atwork, he leads the weekly case conference and co-directs a neuro-rheumatology clinic. Outside of medicine, he enjoys watching animewith his two kittens and—less successfully—singing in the shower.
Sebastian Green (@sebfgreen)
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA).He was born and raised in London,England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has publishedon neuroimaging, memory, sleep, epilepsy, and more. Dr. Green is passionate about medical education in neurology, and using EEGto answer big questions about the brain.
Valeria Roldan (@valeroldan23)
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or reading.
In this episode of the Clinical Unknown Series, Noah and Vini will address a rash case presented by Mark and Debora. Mark will share his insights on the diagnosis by the end of the episode.
Episode description: does your PTT cross the upper limit of normal when you think about the coagulation cascade? Got *mixed* feelings about APLS labs? This episode might be for you!
In this hepatology episode, Dr. Hirsh Elhence presents a case to Dr. Elliot Tapper. They discuss the question: “Is the liver the driver or a bystander?”
Episode 410: Neurology VMR – right hand weakness for 3 months
Jul 31, 2025
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of right hand weakness for 3 months to Vale.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Valeria Roldan (@valeroldan23)
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Episode description: A fascinating case that started as flank pain … ultimately seen in outpatient pulmonology! Join us for this adventure in clinical reasoning.
In this Rheumatology Rafael Medina Subspecialty episode, Dr. Ana Valle presents a case of Joint pain and skin rash to Dr. Eli Miloslavsky.
Session facilitator: Rahul Pottabathini
Case Discussant: Dr. Eli Miloslavsky is a rheumatologist and Associate Professor of Medicine at the Massachusetts General Hospital and Harvard Medical School. Dr. Eli’s Career has been focused on medical education across all stages of training. He Serves as a curriculum phase director at Harvard Medical School, Firm Chief in the MGH Internal Medicine Residency Program and an Associate Program Director in the MGH Rheumatology Fellowship. He also leads the MGH Clinician Educator Track for Department of Medicine subspecialty fellows.
Case Presenter: Dr. Ana Valle, MD, MHS is a rheumatology fellow at Brigham and Women’s Hospital. She attended Johns Hopkins University and the Johns Hopkins Bloomberg School of Public Health where she studied public health during her undergraduate and graduate years. Afterwards, she worked as a research coordinator which introduced her to the field of rheumatology and instilled a passion for clinical research. She then obtained her medical degree from the Zucker School of Medicine at Hofstra/Northwell and completed residency at Montefiore Medical Center in the Bronx, NY, where she was awarded Intern of the Year and Ambulatory Chief. She is pursuing a clinical research career where she dedicates her time to address health inequities within rheumatology and further understand idiopathic inflammatory myopathies. In her free time, she enjoys barre, podcasts, and spending time with her two cats (Dolly & Stevie).
Bayan is a senior medical student from Syria with a passion for neurology and a drive to make a difference in healthcare. From founding a screening initiative for congenital conditions in children to working with other students and residents to create the NeuroAnki flashcard deck to help neurology residents prep for board exams, Bayan is all about supporting others. As a passionate advocate for ethics, she is the co-leader of the journal club team in the neuro-ethics group. Outside of medicine and in her free time, Bayan loves to relax with a cup of tea and a book.
Aye Chan Moe Thant (@AyeThant94)
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Welcome to another episode of the Clinical Unknown Series! Mark presented a case with a chief complaint of constipation to Debora and Mengyu, and there was an unpredictable turnover.
Episode 398: WDx #36: How to Approach a “Struggling” Learner
May 29, 2025
Description: Kaylin and Sharmin are joined once again by Dr. Julia Armendariz to learn from her approach to a “struggling” learner. The discussion focuses on the value of using low-inference statements to accurately describe the behavior, how to identify the underlying problem(s) the behavior may represent, and tailoring a path to improvement based on the learner’s level of insight.
Julia Armendariz, MD, is a hospitalist and clinician educator in the Bay Area who works closely with trainees on the wards and in the classroom. She is the co-director for the Medical Education Elective for the Stanford Internal Medicine Residency, where she shares her passion for Med Ed with Stanford junior and senior residents. Her special areas of interest within Med Ed are communication, specifically feedback, and the struggling learner. She is also a facilitator for a national CME course called MODEL (Maximizing Ongoing Development and Educational Leadership) within the Veteran’s Administration, where she delivers a feedback workshop for attending physicians. She is currently collaborating with faculty at Stanford and other academic programs for research projects, including resident perspectives on faculty feedback delivery, how to improve feedback skills for attending physicians, and how to coach feedback givers. Outside of medicine, Julia loves gardening, the ocean, and spending time with family and friends
In this Maternal-Fetal Medicine (MFM) Rafael Medina Subspecialty episode, Dr. Mary Peeler presents a case of headache in a pregnant patient to Dr. Greg Kirschen.
Case Discussant: Dr. Greg Kirschen is a Maternal-Fetal Medicine fellow at the Hospital of the University of Pennsylvania with a particular interest in pharmacology and metabolism in pregnancy. Before fellowship, he completed an MD/PhD at Stony Brook University in New York with a PhD in molecular pharmacology and then completed residency training in Ob/Gyn at Johns Hopkins Hospital in Baltimore. Teaching and clinical reasoning are his passions and he continues to teach and mentor students from the undergraduate to medical student and resident level.
Case Presenter: Dr. Mary Peeler is originally from Memphis, Tennessee. She completed her undergraduate degree in Health Policy and Management at the University of North Carolina, Chapel Hill. She pursued medical school and residency in Ob/Gyn at Johns Hopkins in Baltimore, Maryland. She also completed a Master’s of Public Health at the Harvard TH Chan School, concentrating in Social and Behavioral Health. She is now in her first year of Maternal Fetal Medicine fellowship back at UNC. Outside of medicine, Mary loves hiking, exploring new places and gardening.
Correction to discussion: – Outcomes for mode of delivery at 24 weeks: outcomes are comparable between c-section and vaginal delivery for breech singletons
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of behavior change, headaches, and blurry vision to Vale.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Valeria Roldan (@valeroldan23)
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Episode description: is a simple case of hyperglycemia hiding something sinister? Elena presents a rich teaching case on a common, but complex, chief complaint.
Episode 27 – Racial and Gender Health Disparities in Youth Suicide: Part 2
Show Notes by Asya Pitre
April 25, 2025
Summary: In this second half of a two-part series, Dr. Tami Benton and Dr. Kevin Simon discuss racial and gender health disparities in youth suicide. They explore the impact of racism, trauma, and inequities in care, while emphasizing the need for culturally grounded, community-based prevention. The episode highlights the importance of policy advocacy, culturally responsive therapy, and practicing cultural humility in mental health care.
Episode Learning Objectives
After listening to this episode, learners will be able to:
Identify barriers and facilitators to establishing care with a child and adolescent psychiatrist
Explain the shifting visibility of racial and gender health disparities in the academic literature
Describe the importance of cultural humility and racial concordance in health care
Credits
Written and produced by: Ashley Cooper, Sudarshan Krishnamurthy, and Team
Host: Ashley Cooper
Infographic and Audio Edits: Ashley Cooper
Show Notes: Asya Pitre
Guests: Dr. Tami Benton and Dr. Kevin Simon
Speaker Biographies
Dr. Tami Benton, MD, is the Frederick Allen Professor of Psychiatry at the University of Pennsylvania. She is the Psychiatrist-in-Chief and Chair of the Department of Child and Adolescent Psychiatry and Behavioral Sciences at the Children’s Hospital of Philadelphia (CHOP). She is the President of The American Association of Directors of Child and Adolescent Psychiatry (AADCAP) and the President of The American Academy of Child and Adolescent Psychiatry (AACAP). She served on the National Institute of Mental Health Advisory Council and the APA’s Council for Research. Dr. Benton mentors clinical and research physicians, fellows, and postdoctoral trainees. She was awarded the Society of Biological Psychiatry Humanitarian Award and the Community Outreach Award by the American Foundation for Suicide Prevention. Dr. Benton’s career has been dedicated to developing leadership for a diverse child psychiatry workforce. Her mission — preparing the next generation of diverse physician leaders in pediatric healthcare and mental health and creating partnerships between communities and academic centers — will be critical for eliminating disparities among minority populations.
Dr. Kevin M. Simon, MD, MPH, is Boston’s inaugural Chief Behavioral Health Officer, appointed by Mayor Michelle Wu. He is a physician-scientist, health policy expert, inspirational teacher, and a gifted writer. Dr. Simon is a pediatric addiction medicine psychiatrist at Boston Children’s Hospital; an assistant professor in psychiatry at Harvard Medical School; a recent Commonwealth Fund fellow in health policy at Harvard University; and the medical director of Wayside Youth & Family Support Network. Clinically, he cares for youth and families through the Department of Psychiatry & Behavioral Sciences and the new Division of Addiction Medicine at Boston Children’s Hospital. Academically, he has won multiple awards for research on structural violence, health equity, and mental health. Additionally, he consults with federal agencies on mental health system design and practices. Dr. Simon’s writings on health equity are in notable journals like the American Journal of Public Health and the New England Journal of Medicine. National audiences regularly seek his perspectives on mental health through trusted outlets.
Episode Takeaways
Rising Suicide Rates Among Black and Indigenous Girls: In this episode of the Clinical Problem Solvers Anti-Racism in Medicine Podcast, host Ashley Cooper is joined by Dr. Tami Benton and Dr. Kevin Simon to continue the conversation on racial and gender health disparities in youth suicide. The episode opens with a discussion on the rising suicide rates among Black girls. Dr. Simon stresses the importance of educational efforts to dismantle biases and calls for greater research attention to this group. Dr. Benton emphasizes the role of intersecting psychosocial factors—poverty, racism, and trauma—that contribute to suicide risk among Black and Indigenous girls and how these early life experiences impact mental health in adulthood.
Community-Based Prevention: The conversation then moves toward community-based prevention, with Dr. Simon advocating for trusted community networks to support youth mental health. He points out that historically, some community spaces have also been sources of harm, so intentional engagement and mental health education are essential. Dr. Benton’s presidential theme, as President of the American Academy of Child and Adolescent Psychiatry, “Bringing the Village to the Children,” underscores the importance of collective responsibility. She highlights promising initiatives like suicide prevention programs in African American churches and the American Foundation for Suicide Prevention-Soul Shop.
Dr. Simon’s Role as Chief Behavioral Health Officer: Dr. Simon shares his work as Boston’s first Chief Behavioral Health Officer, prioritizing substance use treatment and uplifting Black and Indigenous communities. The episode also explores how digital tools can help youth manage their mental health, while also noting the need for culturally relevant care providers.
Disparities in Restraint Practices: Disparities in restraint practices are addressed, particularly the disproportionate use of physical and pharmacologic restraints on Black people.
Policy issues such as the need for enforcement of the Mental Health Parity and Equity Act (MHPAEA) are discussed, alongside practical clinical strategies to prevent youth suicide. These include population-specific adaptations of DBT, attachment-based family therapy, and increasing research on effective interventions for minority youth. A referenced meta-analysis questions the effectiveness of psychotherapy in communities with high levels of anti-Black racism, reinforcing the importance of environmental context in mental health outcomes.
The Mental Health Parity and Addiction Equity Act (MHPAEA) and Youth Suicide Interventions: Racial socialization is offered as a protective intervention for youth facing racism-related trauma.
Key Takeaways (Awareness, Access, and Cultural Humility): The conversation ends by emphasizing awareness of mental health warning signs in youth, advocating for broader access to care, and urging healthcare professionals to practice cultural humility.
Disclosures
The hosts and guests report no relevant financial disclosures.
References
1. Benton TD, Boyd RC, Njoroge WF. Addressing the Global Crisis of Child and Adolescent Mental Health. JAMA Pediatr. 2021;175(11):1108–1110. doi:10.1001/jamapediatrics.2021.2479
2. Benton T, Njoroge WFM, Ng WYK. Sounding the Alarm for Children’s Mental Health During the COVID-19 Pandemic. JAMA Pediatr. 2022;176(4):e216295. doi:10.1001/jamapediatrics.2021.6295
3. Benton TD. Suicide and Suicidal Behaviors Among Minoritized Youth. Child and Adolescent Psychiatric Clinics of North America. 2022;31(2):211-221. doi:10.1016/j.chc.2022.01.002
4. Benton TD. A Culturally Informed Approach to Supporting Suicidal Minoritized Patients. Focus. 2023 Apr;21(2):166-7.
5. Brent DA, Goldstein TR, Benton TD. Bridging Gaps in Follow-up Appointments After Hospitalization and Youth Suicide: Mental Health Care Disparities Matter. JAMA Netw Open. 2020;3(8):e2013100. doi:10.1001/jamanetworkopen.2020.13100
6. Bridge JA, Asti L, Horowitz LM, et al. Suicide Trends Among Elementary School-Aged Children in the United States From 1993 to 2012. 2015;169(7):673-677. doi:10.1001/jamapediatrics.2015.0465
7. Fontanella CA, Hiance-Steelesmith DL, Bridge JA, Lester N, Sweeney HA, Hurst M, Campo JV. Factors Associated With Timely Follow-Up Care After Psychiatric Hospitalization for Youths With Mood Disorders. Psychiatr Serv. 2016 Mar;67(3):324-31. doi: 10.1176/appi.ps.201500104. Epub 2015 Dec 1. PMID: 26620293.
8. Lindsey MA, Sheftall AH, Xiao Y, Joe S. Trends of Suicidal Behaviors Among High School Students in the United States: 1991–2017. Pediatrics. 2019;144(5):e20191187. doi:10.1542/peds.2019-1187
9. Lindsey MA, Brown DR, Cunningham M. Boys do(n’t) cry: Addressing the unmet mental health needs of African American boys. American Journal of Orthopsychiatry. 2017;87:377-383. doi:10.1037/ort0000198
10. Molock, Sherry Davis et al. “Developing suicide prevention programs for African American youth in African American churches.” Suicide & life-threatening behavior vol. 38,3 (2008): 323-33. doi:10.1521/suli.2008.38.3.323
11. Price JH, Khubchandani J. The Changing Characteristics of African-American Adolescent Suicides, 2001–2017. J Community Health. 2019;44(4):756-763. doi:10.1007/s10900-019-00678-x
12. Price, Maggi A et al. “Meta-analysis: Are Psychotherapies Less Effective for Black Youth in Communities With Higher Levels of Anti-Black Racism?.” Journal of the American Academy of Child and Adolescent Psychiatry vol. 61,6 (2022): 754-763. doi:10.1016/j.jaac.2021.07.808
13. Sheftall AH, Vakil F, Ruch DA, Boyd RC, Lindsey MA, Bridge JA. Black Youth Suicide: Investigation of Current Trends and Precipitating Circumstances. Journal of the American Academy of Child & Adolescent Psychiatry. 2022;61(5):662-675. doi:10.1016/j.jaac.2021.08.021
14. Sheftall AH, Miller AB. Setting a Ground Zero Research Agenda for Preventing Black Youth Suicide. 2021;175(9):890-892. doi:10.1001/jamapediatrics.2021.1112
15. Simon KM. Daughters’ Keeper—The Care and Treatment of Black Girls in America. New England Journal of Medicine. 2022 Jun 2;386(22):2067-9.
16. Simon KM. Mitigating the Negative Mental Health Impact of Racism on Black Adolescents—A Preventive Perspective. JAMA Netw Open. 2023;6(11):e2340577. doi:10.1001/jamanetworkopen.2023.40577
17. Simon KM. Them and Me – The Care and Treatment of Black Boys in America. N Engl J Med. 2020 Nov 12;383(20):1904-1905. doi: 10.1056/NEJMp2022606. PMID: 33176082.
18. Congressional Black Caucus: Emergency Task Force on Black Youth Suicide and Mental Health. Ring the Alarm. The Crisis of Black Youth Suicide in America. U.S. Congress. Published December 17, 2019. Accessed 2024. https://watsoncoleman.house.gov/imo/media/doc/full_taskforce_report.pdf
Benton T, Simon K, Cooper A, Krishnamurthy S, Calac A, Pitre A, Pierce G, Onuoha C, Watkins A, Khazanchi R. “Episode 27: Racial and Gender Health Disparities in Youth Suicide: Part 2” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. April 25, 2025.
In this episode, Noah and Marcela explored a compelling case presented by Debora, engaging in a thoughtful discussion. At the end, Mark shared the key teaching points from the case, inspiring us all to reflect and grow.
Description: Dr. Julia Armendariz joins Kaylin, Sharmin, and Cheryl to discuss feedback. She shares why giving feedback is so critical as well as an approach to feedback and goal-setting with learners. She also debunks common myths, highlights potential pitfalls, and shares her strategies to create a positive team learning environment.
Julia’s bio:
Julia Armendariz, MD, is a hospitalist and clinician educator in the Bay Area who works closely with trainees on the wards and in the classroom. She is the co-director for the Medical Education Elective for the Stanford Internal Medicine Residency, where she shares her passion for Med Ed with Stanford junior and senior residents. Her special areas of interest within Med Ed are communication, specifically feedback, and the struggling learner. She is also a facilitator for a national CME course called MODEL (Maximizing Ongoing Development and Educational Leadership) within the Veteran’s Administration, where she delivers a feedback workshop for attending physicians. She is currently collaborating with faculty at Stanford and other academic programs for research projects, including resident perspectives on faculty feedback delivery, how to improve feedback skills for attending physicians, and how to coach feedback givers. Outside of medicine, Julia loves gardening, the ocean, and spending time with family and friends.
Episode 389: Rafael Medina Subspecialty Series – Hypotension and Peaked T waves
Apr 11, 2025
In this Nephrology episode, Dr.Samira Farouk discusses the nuances of AKI, why you should be trending Urine like you trend Troponin. Stay tuned to find out the final diagnosis!
Session facilitator: Dr.Elena Storz
Case Discussants:
Dr.Douglas Farrell MD: Nephrology Fellow, Icahn School of Medicine at Mount Sinai
Dr. Samira Farouk MD: Associate Professor of Medicine and medical Education, Associate Program Director of the Nephrology Fellowship Program, Icahn School of Medicine at Mount Sinai
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Sebastian presents a case of confusion to Aye.
Aye Chan Moe Thant ( @AyeThant94 )
Aye is a physician from Myanmar and now working as a clinical research team member at the Department of Neurology, Washington University in Saint Louis. Throughout her career in Myanmar, she worked closely and received training from her mentor neurologist, one of only three neurologists available for the whole upper Myanmar of 23 million population. Witnessing the challenges faced by the patients from underserved areas, she is dedicated to advancing health equity, research, and global neurology. Aye is also very passionate about medical education and has been deeply involved in Clinical Problem Solvers mainly in neurology with the mentor Dr. Aaron Berkowitz. She is going to apply for neurology residency and very excited about the journey ahead!
Dr. Sebastian Green ( @sebfgreen )
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA). He was born and raised in London, England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has published on neuroimaging, memory, sleep, epilepsy, and more. He is passionate about medical education in neurology, and using EEG to answer big questions about the brain.
Episode 26 – Racial and Gender Health Disparities in Youth Suicide: Part 1
Show Notes by Alec J. Calac
March 14, 2025
Summary: In this first half of a two-part series, we discuss the growing rates of suicide amongst child and adolescent populations in the United States, with a focus on historically underserved groups. In particular, our guests, Dr. Tami Benton and Dr. Kevin Simon, elucidate the disturbing rises in suicidality—suicide attempts and suicidal ideation—and suicide fatality amongst Indigenous and Black youth. Drs. Benton and Simon recount the pervasive nature of the suicide crisis impacting Black and Indigenous youth and offer insights into how we may begin ameliorating these harrowing inequities.
Episode Learning Objectives
After listening to this episode, learners will be able to:
Identify barriers and facilitators to establishing care with a child and adolescent psychiatrist
Explain the shifting visibility of racial and gender health disparities in the academic literature
Describe the importance of cultural humility and racial concordance in health care
Credits
Written and produced by: Ashley Cooper, Sudarshan Krishnamurthy, Asya Pitre, and Team
Hosts: Ashley Cooper and Sudarshan Krishnamurthy
Infographic and Audio Edits: Ashley Cooper
Show Notes: Alec J. Calac
Guest: Dr. Tami Benton and Dr. Kevin Simon
Time Stamps
0:00 Opening and Guest Biographies
3:15 Personal Guest Introductions (Dr. Simon)
6:50 Personal Guest Introductions (Dr. Benton)
13:08 Youth Suicide Crisis Discussion, “Ringing the Alarm”
20:10 Shift in Issue Framing in the Literature
24:31 The Network Begins with Primary Care
28:42 Diversifying your Outreach
30:54 Cultural Humility
Speaker Biographies
Dr. Tami Benton, MD, is the Frederick Allen Professor of Psychiatry at the University of Pennsylvania. She is the Psychiatrist-in-Chief and Chair of the Department of Child and Adolescent Psychiatry and Behavioral Sciences at the Children’s Hospital of Philadelphia (CHOP). She is the President of The American Association of Directors of Child and Adolescent Psychiatry (AADCAP) and the President of The American Academy of Child and Adolescent Psychiatry (AACAP). She served on the National Institute of Mental Health Advisory Council and the APA’s Council for Research. Dr. Benton mentors clinical and research physicians, fellows, and postdoctoral trainees. She was awarded the Society of Biological Psychiatry Humanitarian Award and the Community Outreach Award by the American Foundation for Suicide Prevention. Dr. Benton’s career has been dedicated to developing leadership for a diverse child psychiatry workforce. Her mission — preparing the next generation of diverse physician leaders in pediatric healthcare and mental health and creating partnerships between communities and academic centers — will be critical for eliminating disparities among minority populations.
Dr. Kevin M. Simon, MD, MPH, is Boston’s inaugural Chief Behavioral Health Officer, appointed by Mayor Michelle Wu. He is a physician-scientist, health policy expert, inspirational teacher, and a gifted writer. Dr. Simon is a pediatric addiction medicine psychiatrist at Boston Children’s Hospital; an assistant professor in psychiatry at Harvard Medical School; a recent Commonwealth Fund fellow in health policy at Harvard University; and the medical director of Wayside Youth & Family Support Network. Clinically, he cares for youth and families through the Department of Psychiatry & Behavioral Sciences and the new Division of Addiction Medicine at Boston Children’s Hospital. Academically, he has won multiple awards for research on structural violence, health equity, and mental health. Additionally, he consults with federal agencies on mental health system design and practices. Dr. Simon’s writings on health equity are in notable journals like the American Journal of Public Health and the New England Journal of Medicine. National audiences regularly seek his perspectives on mental health through trusted outlets.
Episode Takeaways
Community health centers play an important role in access to evidence-based psychiatric care rooted in community values. They are often the first interface for patients experiencing mental health crises, not academic medical centers.
The youth suicide crisis is disproportionately shouldered by Indigenous and Black and African American communities. Historical challenges include inadequate data surveillance and reporting systems and “hidden” trends brought to the attention of academics by Dr. Jeffrey Bridge, a leading researcher at the Nationwide Children’s Hospital. Among these groups, youth suicide is particularly more prominent at younger ages when compared to other racial and ethnic groups.
Groups experiencing severe morbidity and mortality–due to any psychiatric cause–often do not reflect the demographics of inpatient hospital censuses. Comprehensive mental health interventions are often beyond reach of those uninsured and underinsured.
Resources are often directed to the largest group by number, not necessarily the group with the highest incidence and prevalence per capita. This can have devastating effects on public health and impede timely policy and program development. Literature has also shown that youth beneficiaries in Medicaid are not prioritized for mental health services when compared to other programs, which impedes continuity of care.
There are a growing number of Child Psychiatric Access Programs, including one in Massachusetts, which provide quick access to psychiatric consultation and facilitates referrals for accessing ongoing behavioral health care. These programs recognize the increasing difficulties in having to first see a community-based primary care provider before seeing a specialized psychiatrist.
Diversifying your mental health outreach goes hand in hand with diversifying your providers. This is directly related to the importance of cultural humility in mitigating health disparities among racial and gender minority youth, as well as literature highlighting the benefits of racial concordance between providers and patients.
According to a 2019 study published by Price and Khubchandani, the suicide rate among Black girls increased by a striking 182% over the course of 2001 to 2017. Despite these increases there remains a paucity of literature addressing this critical disparity.
Language plays an important role in obtaining a thorough mental health history. Youth are often not familiar with medical jargon on questionnaires and intake forms, which can work against important conversations and opportunities for shared decision-making.
Large language models and artificial intelligence technologies are likely biased by the documentation we place in the electronic health record, which may reinforce youth health disparities.
Disclosures
The hosts and guests report no relevant financial disclosures.
References
Benton TD, Boyd RC, Njoroge WF. Addressing the Global Crisis of Child and Adolescent Mental Health. JAMA Pediatr. 2021;175(11):1108–1110. doi:10.1001/jamapediatrics.2021.2479
Benton T, Njoroge WFM, Ng WYK. Sounding the Alarm for Children’s Mental Health During the COVID-19 Pandemic. JAMA Pediatr. 2022;176(4):e216295. doi:10.1001/jamapediatrics.2021.6295
Benton TD. Suicide and Suicidal Behaviors Among Minoritized Youth. Child and Adolescent Psychiatric Clinics of North America. 2022;31(2):211-221. doi:10.1016/j.chc.2022.01.002
Benton TD. A Culturally Informed Approach to Supporting Suicidal Minoritized Patients. Focus. 2023 Apr;21(2):166-7.
Brent DA, Goldstein TR, Benton TD. Bridging Gaps in Follow-up Appointments After Hospitalization and Youth Suicide: Mental Health Care Disparities Matter. JAMA Netw Open. 2020;3(8):e2013100. doi:10.1001/jamanetworkopen.2020.13100
Bridge JA, Asti L, Horowitz LM, et al. Suicide Trends Among Elementary School-Aged Children in the United States From 1993 to 2012. 2015;169(7):673-677. doi:10.1001/jamapediatrics.2015.0465
Fontanella CA, Hiance-Steelesmith DL, Bridge JA, Lester N, Sweeney HA, Hurst M, Campo JV. Factors Associated With Timely Follow-Up Care After Psychiatric Hospitalization for Youths With Mood Disorders. Psychiatr Serv. 2016 Mar;67(3):324-31. doi: 10.1176/appi.ps.201500104. Epub 2015 Dec 1. PMID: 26620293.
King, C. A., Brent, D., Grupp-Phelan, J., Shenoi, R., Page, K., Mahabee-Gittens, E. M., Chernick, L. S., Melzer-Lange, M., Rea, M., McGuire, T. C., Littlefield, A., & Casper, T. C. (2020). Five Profiles of Adolescents at Elevated Risk for Suicide Attempts: Differences in Mental Health Service Use. Journal of the American Academy of Child & Adolescent Psychiatry, 59(9), 1058-1068.e5. https://doi.org/10.1016/j.jaac.2019.10.015
Lindsey MA, Sheftall AH, Xiao Y, Joe S. Trends of Suicidal Behaviors Among High School Students in the United States: 1991–2017. Pediatrics. 2019;144(5):e20191187. doi:10.1542/peds.2019-1187
Lindsey MA, Brown DR, Cunningham M. Boys do(n’t) cry: Addressing the unmet mental health needs of African American boys. American Journal of Orthopsychiatry. 2017;87:377-383. doi:10.1037/ort0000198
Price JH, Khubchandani J. The Changing Characteristics of African-American Adolescent Suicides, 2001–2017. J Community Health. 2019;44(4):756-763. doi:10.1007/s10900-019-00678-x
Sheftall AH, Vakil F, Ruch DA, Boyd RC, Lindsey MA, Bridge JA. Black Youth Suicide: Investigation of Current Trends and Precipitating Circumstances. Journal of the American Academy of Child & Adolescent Psychiatry. 2022;61(5):662-675. doi:10.1016/j.jaac.2021.08.021
Sheftall AH, Miller AB. Setting a Ground Zero Research Agenda for Preventing Black Youth Suicide. 2021;175(9):890-892. doi:10.1001/jamapediatrics.2021.1112
Simon KM. Daughters’ Keeper—The Care and Treatment of Black Girls in America. New England Journal of Medicine. 2022 Jun 2;386(22):2067-9.
Simon KM. Mitigating the Negative Mental Health Impact of Racism on Black Adolescents—A Preventive Perspective. JAMA Netw Open. 2023;6(11):e2340577. doi:10.1001/jamanetworkopen.2023.40577
Simon KM. Them and Me – The Care and Treatment of Black Boys in America. N Engl J Med. 2020 Nov 12;383(20):1904-1905. doi: 10.1056/NEJMp2022606. PMID: 33176082.
Benton T, Simon K, Cooper A, Krishnamurthy S, Calac A, Pitre A, Pierce G, Essien UR, Fields NF, Lopez-Carmen V, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Khazanchi R. “Episode 26: Racial and Gender Health Disparities in Youth Suicide: Part 1” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. March 14, 2025.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of double vision to Vale.
Aye Chan Moe Thant ( @AyeThant94 )
Aye is a physician from Myanmar and now working as a clinical research team member at the Department of Neurology, Washington University in Saint Louis. Throughout her career in Myanmar, she worked closely and received training from her mentor neurologist, one of only three neurologists available for the whole upper Myanmar of 23 million population. Witnessing the challenges faced by the patients from underserved areas, she is dedicated to advancing health equity, research, and global neurology. Aye is also very passionate about medical education and has been deeply involved in Clinical Problem Solvers mainly in neurology with the mentor Dr. Aaron Berkowitz. She is going to apply for neurology residency and very excited about the journey ahead!
Valeria Roldan
@valeroldan23
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Episode 374: WDx #34: It’s Not a Meritocracy
Jan 23, 2025
Description:
Kaylin, Sharmin, and Cheryl are joined by Dr. Arghavan Salles. They discuss career transitions/pivots, challenging workplace experiences, social/digital media use, and thoughts on allyship and gender biases/stereotype threat as self-identified angry women.
Bio:
Dr. Salles is a minimally invasive and bariatric surgeon. She completed medical school and residency in general surgery at Stanford prior to completing her fellowship in minimally invasive surgery at Washington University in St. Louis. She stayed on faculty at Washington University for three years prior to moving back to Stanford in 2019. During the pandemic, Dr. Salles has served as a disaster relief physician, caring for patients with COVID in the ICU. Dr. Salles obtained a PhD in education from Stanford University during her residency training, and her research focuses on gender equity, implicit bias, diversity, inclusion, and physician well-being. Her R01 grant from the NIH focuses on sexual harassment. She is a sought-after speaker and has given over 100 national and international invited talks related to gender equity, physician well-being, and weight bias. She currently serves as the Special Advisor for DEI Programs at the Stanford University Department of Medicine where she is a Clinical Associate Professor.
In this Pulmonary & Critical Care episode, Dr. Meghan Nothem presents an unusual case of acute encephalopathy and unresponsiveness to Dr. Paul A. Bergl. Stay tuned to found out the final diagnosis!
Dr. Paul A. Bergl is an intensivist at Gundersen Lutheran Medical Center in La Crosse, WI and clinical adjunct assistant professor with the University of Wisconsin. He completed medical school at the University of Wisconsin-Madison, internal medicine residency at the University of Chicago, and critical care fellowship at the Medical College of Wisconsin.
Dr. Bergl is a decorated educator with over a dozen major teaching awards and honors from medical students, residents, and fellows. His foremost passions in medical eduation are critical thinking and diagnostic reasoning. His other scholarly work has focused on diagnostic error, point-of-care ultrasonography and echocardiography, and bedside teaching and rounding.
Case presenter: Dr. Meghan Nothem
Dr. Nothem is a third year Pulmonary & Critical Care Medicine fellow at The Medical College of Wisconsin in Milwaukee, Wisconsin where she also completed her Internal Medicine residency and served as Chief Resident. Prior to returning to her home city for post-graduate training, she earned her Bachelor of Science in Biology at University of Wisconsin-Madison and her medical degree at Rocky Vista University College of Osteopathic Medicine in Parker, Colorado. Dr. Nothem will be joining a Pulmonary and Critical Care Medicine practice in Milwaukee upon completion of her fellowship in summer of 2025.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Dr. Sebastian Green presents a case of generalized weakness to Aye.
Aye is a physician from Myanmar and now working as a clinical research team member at the Department of Neurology, Washington University in Saint Louis. Throughout her career in Myanmar, she worked closely and received training from her mentor neurologist, one of only three neurologists available for the whole upper Myanmar of 23 million population. Witnessing the challenges faced by the patients from underserved areas, she is dedicated to advancing health equity, research, and global neurology. Aye is also very passionate about medical education and has been deeply involved in Clinical Problem Solvers mainly in neurology with the mentor Dr. Aaron Berkowitz. She is going to apply for neurology residency and very excited about the journey ahead!
Dr. Sebastian Green ( @sebfgreen )
Dr. Sebastian Green is a neurology resident at the University of California, Los Angeles (UCLA). He was born and raised in London, England. He has degrees in Medicine from the University of Bristol and Neuroscience from the University of Oxford. He has published on neuroimaging, memory, sleep, epilepsy, and more. He is passionate about medical education in neurology, and using EEG to answer big questions about the brain.
Episode description: Welcome our new SLS team member, Seyma! The SLS team get together from four time zones across the world to discuss a challenging case of altered mental status.
Episode 369: WDx #33: Clinical Unknown Discussion with Dr Laila Woc-Colburn
Dec 11, 2024
In this episode of WDx, Sharmin, Yaz, and Kaylin are joined by Dr. Laila Woc-Colburn. Tune in to hear Dr. Woc expertly discuss a case of a young woman with a worsening headache, followed by a roundtable discussion about what drew her to infectious diseases and her passions in medicine and life.
Bio:
**Laila Woc-Colburn, MD** is an associate professor in the Division of Infectious Diseases at Emory University School of Medicine. A graduate of Universidad Francisco Marroquín in Guatemala, she completed her internal medicine residency at Advocate Illinois Masonic Medical Center in Chicago and her fellowship in infectious diseases and HIV medicine at Case Western University in Cleveland. Dr. Woc-Colburn also holds a Diploma in Tropical Medicine and Hygiene.
Her clinical interests encompass tropical diseases in immunosuppressed individuals, including those with HIV, as well as mycotic diseases, orthopedic infections, and medical education. She is passionate about teaching the next generation of healthcare professionals about infectious diseases and is dedicated to empowering women and BIPOC individuals in medicine.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Bayan presents a case of headache and seizure to Aye.
Aye is a physician from Myanmar and now working as a clinical research team member at the Department of Neurology, Washington University in Saint Louis. Throughout her career in Myanmar, she worked closely and received training from her mentor neurologist, one of only three neurologists available for the whole upper Myanmar of 23 million population. Witnessing the challenges faced by the patients from underserved areas, she is dedicated to advancing health equity, research, and global neurology. Aye is also very passionate about medical education and has been deeply involved in Clinical Problem Solvers mainly in neurology with the mentor Dr. Aaron Berkowitz. She is going to apply for neurology residency and very excited about the journey ahead!
Bayan Al Zoabu
Bayan is a senior medical student from Syria with a passion for neurology and a drive to make a difference in healthcare. From founding a screening initiative for congenital conditions in children to working with other students and residents to create the NeurAnki flashcard deck to help neurology residents prep for board exams, Bayan is all about supporting others. As a passionate advocate for ethics, she is the co-leader of the journal club team in the neuro-ethics group. Outside medicine and in her free time, Bayan loves to relax with a cup of tea and a book.
Episode description: Jas presents a fascinating case of chest pain, dyspnea, and lower extremity edema that ends up in a very different place than any of us expected. Welcome to our new teammate Elena!
Kaylin, Sharmin, Cheryl, and Jane discuss two cases of volume overload. Kaylin reviews the pathophysiology behind constrictive pericarditis and restrictive cardiomyopathy, normal pericardial and thoracic anatomy and pressure changes with respiration, and the difference in treatments between the two disease processes.
This joint rheumatology and pulmonary critical care medicine session is a collaboration between CPSolvers and The University of Colorado. This session, like all Rafa Medina Subspecialty sessions, is in honor of Dr. Rafael Medina. Dr. Melissa Griffith and Dr. Geoff Connors discuss a case of myositis presented by Dr. Sarah Haeger and Dr. Evan Zehr
Case Discussants: Geoff Connors is an associate professor in Pulmonary and Critical Care at the University of Colorado. He is the Associate Dean for Graduate Medical Education and is the former program director of the Internal Medicine Program at University of Colorado. Melissa Griffith is an Assistant Professor of Rheumatology at the University of Colorado.
Case Presenters: Sarah Haeger was a chief medical resident at the University of Colorado and is currently a nephrology fellow at the University of Washington. Evan Zehr was a chief medical resident at the University of Colorado and is currently a fellow in Pulmonary and Critical Care medicine at Vanderbilt.
Episode title: Episode 359 Neurology VMR – altered mental status
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Vale presents a case of altered mental status to Aye.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Valeria Roldan
@valeroldan23
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Episode 354: Antiracism in Medicine – Episode 25 – Live from SGIM 2024: Best of Antiracism Research at the Society of General Internal Medicine’s 2024 Annual Meeting
Sep 19, 2024
Episode 25 – Live from SGIM 2024: Best of Antiracism Research at the Society of General Internal Medicine’s 2024 Annual Meeting
Show Notes by Ashley M. Cooper
September 19, 2024
Summary: This episode highlights a selection of antiracism research presentations at a live recording of the podcast at the 2024 SGIM Annual Meeting. This year’s episode, our fourth conducted at SGIM, is focused on the importance of qualitative research and the role it plays in antiracism research, community-based work, and scholarship. During this episode, we hear from Dr. S. Michelle Ogunwole, MD, PhD, an internist and social epidemiologist who specializes in the care of women with chronic medical conditions and racial disparities in maternal health outcomes, and Dr. Caroline Sloan, MD, a general internist whose research focuses on how financial considerations are imbued into medical decision-making. This episode is hosted by Ashley Cooper and Sudarshan (Sud) Krishnamurthy. The show notes for this episode were written by Ashley M. Cooper.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Understand how they can better center patient experiences by engaging with, and conducting their own, qualitative research.
Describe the positive impacts of qualitative methods on healthcare provision and/or policies in clinical settings.
Identify the critical role that qualitative research plays in antiracism and health equity work.
Credits
Written and produced by: Ashley Cooper, Sudarshan Krishnamurthy, Team
Hosts: Ashley M. Cooper, Sudarshan Krishnamurthy
Infographic: Canva
Audio Edits: Ashley M. Cooper
Show Notes: Ashley M. Cooper
Guests: Dr. Michelle Ogunwole and Dr. Caroline Sloan
Time Stamps
00:00: Opening
00:10: Introductions
01:03: Guest Introduction 1 – Dr. S. Michelle Ogunwole
01:54: Guest Introduction 2 – Dr. Caroline Sloan
02:48: Background and Inspiration for Guests
7:21: Barriers to Pursuing Qualitative Research in Medicine
12:31: The Role of Qualitative Research in Cultivating Health Equity
19:37: Qualitative Research as a vehicle towards centering patient experiences in research
28:14: Audience Questions
28:16: Meta-Cognition: Evaluating Biases in Interpreting Qualitative Data
34:05: Trajectory of Qualitative Research’s Incorporation into Medical Curricula
39:33: Qualitative Research at the Nexus of Storytelling and Narrative Medicine
45:42: Honoring Community Stakeholders in Qualitative Research
49:00: Fostering Communal Trust: Advocacy and Patient-Centered Care
52:33: Humility and Community Involvement
56:55: Closing Remarks
Speaker biographies (Abbreviated)
Dr. S. Michelle Ogunwole, MD, PhD is a health disparities researcher, social epidemiologist and General Internal Medicine physician specializing in the care of women with chronic medical conditions. She has advanced training in Quality Improvement and Patient Safety Science. She currently practices at Johns Hopkins Hospital in Baltimore, MD. Her research is focused on racial disparities in maternal health outcomes among African American women.
Dr. S. Michelle Ogunwole, MD, PhD is a health disparities researcher, social epidemiologist and General Internal Medicine physician specializing in the care of women with chronic medical conditions. She has advanced training in Quality Improvement and Patient Safety Science. She currently practices at Johns Hopkins Hospital in Baltimore, MD. Her research is focused on racial disparities in maternal health outcomes among African American women.
References
Ogunwole, S. M., Chen, X., Mitta, S., Minhas, A., Sharma, G., Zakaria, S., Vaught, A. J., Toth-Manikowski, S. M., & Smith, G. (2021). Interconception Care for Primary Care Providers: Consensus Recommendations on Preconception and Postpartum Management of Reproductive-Age Patients With Medical Comorbidities. Mayo Clinic Proceedings: Innovations, Quality & Outcomes, 5(5), 872–890. https://doi.org/10.1016/j.mayocpiqo.2021.08.004
Ogunwole, S. M., Karbeah, J., Bozzi, D. G., Bower, K. M., Cooper, L. A., Hardeman, R., & Kozhimannil, K. (2022). Health Equity Considerations in State Bills Related to Doula Care (2015–2020). Women’s Health Issues, 32(5), 440–449. https://doi.org/10.1016/j.whi.2022.04.004
Ogunwole, S. M., Oguntade, H. A., Bower, K. M., Cooper, L. A., & Bennett, W. L. (2023). Health Experiences of African American Mothers, Wellness in the Postpartum Period and Beyond (HEAL): A Qualitative Study Applying a Critical Race Feminist Theoretical Framework. International Journal of Environmental Research and Public Health, 20(13), Article 13. https://doi.org/10.3390/ijerph20136283
Sinaiko, A. D., Sloan, C. E., Soto, M. J., Zhao, O., Lin, C.-T., & Goss, F. R. (2023). Clinician Response to Patient Medication Prices Displayed in the Electronic Health Record. JAMA Internal Medicine, 183(10), 1172–1175. https://doi.org/10.1001/jamainternmed.2023.3307
Sloan, C. E., Millo, L., Gutterman, S., & Ubel, P. A. (2021). Accuracy of Physician Estimates of Out-of-Pocket Costs for Medication Filling. JAMA Network Open, 4(11), e2133188. https://doi.org/10.1001/jamanetworkopen.2021.33188
Sloan, C. E., & Ubel, P. A. (2019). The 7 Habits of Highly Effective Cost-of-Care Conversations. Annals of Internal Medicine, 170(9_Supplement), S33–S35. https://doi.org/10.7326/M19-0537
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Ogunwole M, Sloan C, Cooper A, Krishnamurthy S, Calac A, Pitre A, Pierce G, Essien UR, Fields NF, Lopez-Carmen V, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Khazanchi R. “Episode 25: Live from SGIM 2024: Best of Antiracism Research at the Society of General Internal Medicine’s 2024 Annual Meeting” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. September 19, 2024.
In this Clinical Reasoning Rafael Medina Subspecialty episode, Dr. Kuchal Agadi presents a case to Dr. John Woller and Dr. Areeb Masood of a 67 year-old male with altered mental status.
The goal of this session is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case discussant:
Dr. John Woller is an academic hospitalist working in the Johns Hopkins Hospital in the Division of Hospital Medicine. As a clinical coach and Associate Program Director for clinical reasoning and bedside medicine, John is enthusiastic about teaching medical students and Osler residents at the bedside.
And Dr. Areeb Masood, is a third-year internal medicine resident at Johns Hopkins Hospital in the Osler Internal Medicine Residency and Urban Health Track. He earned his undergraduate degree from The University of Texas at Austin and his medical degree from The University of Texas Rio Grande Valley School of Medicine. After completing his residency, he aims to practice a blend of hospital medicine and HIV primary care. @areebmasoodMD
Case presenter:
Dr. Kuchal Agadi, is first year Resident at a community hospital in Chicago. Kuchal is passionate about medical education. Apart from medicine she is a fitness enthusiast, and enjoys a good workout routine with Kettle bells.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of bilateral lower limb weakness to Valeria.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Valeria Roldan
@valeroldan23
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Episode 348: WDx #31: “Guardian Angels, Mistaken Identities, and Code Blues: Stories from Intern Year”
Aug 08, 2024
https://clinicalproblemsolving.com/wp-content/uploads/2024/08/8.8-Wdx-RTP.mp3 To celebrate the new academic year, Kaylin and Sharmin sit down with Dr. Alice Mao to share a few memorable stories from their intern year. They reflect on tough days, lessons learned, power moves, and the importance of community. We hope these stories and reflections make you laugh, feel connected, and inspire you to take gentle care of yourself. Welcome to the profession—we are so excited to have you. Dr. Alice Mao is an internal medicine and geriatric medicine physician who is passionate about social equity, community empowerment, and innovations in primary care. She was born in China and grew up in Canada and the US. She completed medical school at UCSF, internal medicine residency at the University of Washington, and geriatric medicine fellowship at Stanford. She is currently a primary care provider at On Lok Program of All-Inclusive Care for the Elderly where she gets to take care of help vulnerable seniors stay home for as long as possible. Outside of medicine, she enjoys spending time with family and friends, giving her cat cheek scratches, and resurrecting her childhood dreams of learning how to freestyle dance.
In this Infectious Disease Rafael Medina Subspecialty episode, Dr. Milee Nelson presents a case to Dr. John Huang & Dr. Varun Phadke of a man presenting with a rash and shortness of breath.
The goal of this series is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case Discussants: Dr. Varun Phadke is an infectious disease specialist at Emory.
Dr. John Huang is an infectious disease fellow at Emory.
Case Presenter: Dr. Milee Nelson is an internal medicine resident at Emory.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of bilateral lower limb weakness to Valeria.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Valeria Roldan
@valeroldan23
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine.
Sharmin, Kaylin, and Jane interview Anu Gorukanti, MD and Laura Holford, RN MSN, the co-founders of Introspective Spaces. They discuss their journeys in healthcare and what motivated them to build an inclusive space to foster connection, cultivate contemplative practice, and empower women in healthcare through introspective and reflection.
Anu Gorukanti, MD is a public health advocate and pediatric hospitalist at a county hospital in Los Angeles, CA who is passionate about health equity and racial justice. She went to undergraduate and medical school at Saint Louis University and completed her residency at Stanford University. She is passionate about social justice and the role that reflection and contemplation play as building blocks for revolution (as inspired by many theologians, spiritual leaders, and activists before her). She strongly believes that understanding who you are, what you value, and where your values come from can lead to a meaningful and authentic life. In her perspective, social change should always honor and incorporate both the individual and systems-based approach.
Laura Holford, RN MSN, is an oncology certified nurse and public health nurse committed to working to reduce nursing burnout and moral distress, and the reassembly of responsibility and accountability in healthcare. Liberation theology led her to train as a masters prepared nurse at University of San Francisco. She works as a community health nurse in Sacramento, CA She has a background as a campus minister & was lay community pastor of an Christian Interfaith church and she enjoys nothing more than accompanying people on their healing, reflective, and spiritual paths. Like many mystics before her, she believes that contemplation and action cannot be separated and finds herself naturally helping others’ build reflective, imaginative, and spiritual practices to ground their action and work in the world.
In this Nephrology Rafael Medina Subspecialty episode, Dr. Maddie Abrams presents a case to Dr. Jai Radhakrishnan of a 28 year old woman presenting with headache and blurry vision.
The goal of this session is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case discussant: Dr. Jai Radhakrishnan is Professor of Medicine at Columbia University Medical Center in New York. He is the Director of Clinical Services of the Nephrology Division and co-director of the hypertension center of Columbia University. @jradnephro
Case presenter: Dr. Maddie Abrams is an Internal Medicine PGY-2 & an aspiring cardiologist at ColumbiaMed at NewYork-Presbyterian Hospital. She graduated from Zucker School of Medicine in 2022. @Maddie_Abrams
Episode 339: Neurology VMR – left facial numbness for 5 days
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Aye presents a case of left facial numbness for 5 days to Andrea and Sridhara.
Aye graduated from University of Medicine, Mandalay, Myanmar, and has been working with her mentor neurologist, one of only three neurologists covering the Upper Myanmar region of 23 million population. Through her experiences witnessing the challenges faced by patients in underserved areas and hearing their stories, Aye is dedicated to advancing health equity, global health initiatives, and various aspects of neurology, both in clinical practice and medical education. She is going to apply for a neurology residency program this year. Outside of work, she spends time playing piano, jogging along trails, and listening to music.
Andrea Mendez Colmenares
@andreamendez92
Andrea Mendez Colmenares is a Venezuelan medical doctor and cognitive neuroscientist. She recently completed her PhD and postdoctoral fellowship in Colorado and will begin her neurology residency at Duke University in North Carolina in the summer of 2024. Outside of medicine, she enjoys playing guitar, discovering new coffee shops, hiking, and climbing mountains.
Sridhara Yaddanapudi
@syaddana_neuro
Sridhara is a board-certified internist, neurologist, vascular neurologist, and hypertension specialist. Currently, he holds the position of Clinical Assistant Professor at Thomas Jefferson University Hospital and serves as the Director of Neurology for Jefferson New Jersey. As a medical professional, he is passionate about case-based learning, clinical reasoning, and teaching decision-making while avoiding the pitfalls of heuristics. His goal is to bridge the ever-growing gap between neurology and internal medicine, an area in which he has a keen interest.
In this episode of WDx, Dr Nidhi Patel joins Jane, Kaylin, and Sharmin and presents a case of a 23 yr old woman with worsening dyspnea and orthopnea.
Screenshot
Nidhi is a current CPSolvers Academy member and a PGY2 in internal medicine at Emory University. She grew up in South Florida and went to University of Miami for undergrad and for medical school. Clinically she is interested in prevention of atherosclerotic disease, cardiac imaging and women’s health in cardiology! In her free time, she loves to catch a morning sunrise, and loves being outdoors to try adventurous activities including white water rafting, kayaking, and fast roller coasters.
This case was recently presented by Nidhi on a VMR with Rabih and Reza. Check it out here!
The goal of this series is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case Discussant: Dr. Lianne Gensler is a rheumatologist and serves as director of the UCSF Ankylosing Spondylitis Clinic, which is dedicated to care for this inflammatory disease. Gensler’s primary research interest is the disease progression of axial spondyloarthritis (a category that includes ankylosing spondylitis).
Case Presenter: Dr. Appledene Osbourne is a current rheumatology fellow at UCSF.
Episode 331: Neurology VMR – Headaches and loss of sensation in the left leg
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Hans presents a case of headaches and loss of sensation in the left leg to Andrew and Maria.
Hans Kaus received his MD from Ross University School of Medicine. He completed his undergraduate education in Pharmacy at the University of Tübingen, Germany. Driven by a deep desire to understand patient concerns, Hans wanted to go beyond pharmaceutical care. While in medical school, the virtual morning reports, Clinical Problem Solvers, unleashed his passion for solving complex patient cases. The blend of medicine and pharmacy will markedly benefit patients. In his spare time, Hans enjoys embarking on long bicycle rides.
Andrew Sanchez
@ASanchez_PS
Andrew Sanchez is an exiting PGY-3 in internal medicine at Yale New Haven Hospital: he will soon be starting a career in academic hospital medicine at Beth Israel Deaconess Medical Center, Boston. Meeting hospitalized patients and working with them to achieve diagnostic clarity is his primary clinical passion. His interest in diagnosing the undifferentiated patient is the driving force behind deep interest in learning and teaching diagnostic reasoning. On X/Twitter – which he considers the centerpiece of his teaching portfolio – he is known for creating and sharing schemas for both common and uncommon clinical dilemmas, which are frequently accompanied by “Tweetorial” commentary, as well as diagnostic case challenges.
María Jimena Alemán
@MariaMjaleman
María Jimena Alemán was born and raised in Guatemala. After suffering from long-standing neurophobia, she has embraced her love for neurology and will soon be starting her neurology residency at the University of California San Francisco. She looks forward to dedicating her life to improving neurological care and education around the globe. Maria loves art and culture and is currently obsessed with textiles and flowers
In honor of Women’s History month in the United States, Sharmin, Kaylin, and Jane discuss the Matilda Effect, the current state of gender inequality, and reflect on some of the many incredible women scientists that came before us and helped pave the way for a better future.
In this clinical reasoning Rafael Medina Subspecialty episode, Dr. Mark Heslin presents a case to Dr. Tony Breu of a man presenting with facial swelling.
The goal of this series is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case Discussant: Anthony C. Breu, MD is the Director of Resident Education at the Veterans Affairs Boston Healthcare System and an Assistant Professor of Medicine at Harvard Medical School. He is also core faculty at the Center for Bioethics at Harvard Medical School. He completed his undergraduate degree in biomedical ethics at Brown University, where he also received his medical degree.
Case Presenter: Mark Heslin is a third-year internal medicine resident at the University of Pennsylvania. This summer, he will be starting his career as an academic hospitalist at Stanford. His clinical interests include medical education, clinical reasoning, diagnostic error, and the use of innovative technology to disseminate the teaching of clinical reasoning.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Valeria presents a case of visual hallucinations to Greg and Umbish.
Valeria Roldan was born and raised in Lima, Peru. She recently graduated medical school at Universidad Peruana Cayetano Heredia and is excited to pursue a career in Neurology. She is passionate about LGBTQ+ health, particularly advocating for trans rights, as well as medical education. She would describe herself as an optimist and outside of medicine you probably will find her running or talking about pop culture over a glass of wine
Gregory I. Atafo
Dr. Atafo is a general physician currently practicing in Accra, Ghana. He attended undergrad at the University of Benin, Nigeria where he received his degree as a Doctor of Optometry. He then attended the University of Ghana for his medical degree. He is currently applying for residency in the United States and has interests in Neuroscience, Internal Medicine and Global health.
In his free time, Greg loves to play soccer, volunteer at medical outreach programs and is passionate about sharing medical knowledge across borders.
Umbish Dino
@UmbishD
Umbish Dino, born in New York but raised in Pakistan, embodies a blend of cultures that enrich her perspective both personally and professionally. Having lived and worked in both the United States and Pakistan, she’s set to bring her diverse experiences back to the U.S. as she embarks on her journey into the 2024 internal medicine residency match. Outside the hospital, she is a devoted mom to her four-year-old son, Rayyan, and two cats, Drogo and Luna. She is a talented singer, and a culinary enthusiast who finds joy in cooking. Her passion for clinical reasoning has drawn her to the CP Solvers Academy, where she engages with complex medical cases, reflecting her commitment to excellence in patient care and her zeal for continuous learning.
Episode 24 – Leveraging Narrative Medicine to Cultivate Antiracist Praxis
Show Notes by Sudarshan Krishnamurthy
February 13, 2024
Summary: This episode highlights the ways in which we might leverage stories, at the individual and structural levels, to reimagine medicine with a liberatory practice. During this episode, we hear from Zahra Khan, an educator and editor who has written extensively on abolition in medicine, and Dr. Sayantani DasGupta, a physician-educator, prolific children’s book author and faculty at the Center for the Study of Ethnicity and Race and the Institute for Comparative Literature and Society at Columbia University. Together, our guests offer context around how the medical and carceral systems are deeply intertwined and go hand-in-hand. Further, they expand on this to discuss how we might use stories in the form of visionary and speculative fiction to reimagine new landscapes of health care. This discussion is hosted by Sudarshan Krishnamurthy and Ashley Cooper. The show notes for this episode were written by Sudarshan Krishnamurthy.
Episode Learning Objectives
After listening to this episode, learners will be able to:
Illustrate the relationship between narrative medicine and healing relationships.
Explain the significance of abolition medicine, and the role of the medical system in upholding and perpetuating carceral logics.
Discuss how we might use narrative and stories to enact social change and reimagine medicine.
Credits
Written and produced by: Sudarshan Krishnamurthy, Ashley Cooper, Team
Hosts: Sudarshan Krishnamurthy and Ashley Cooper
Infographic: Creative Edge Design
Audio Edits: Ashley Cooper
Show Notes: Sudarshan Krishnamurthy
Guests: Dr. Sayantani DasGupta, Zahra Khan
Time Stamps
00:00 Opening
00:45 Introductions
01:03 Guest Introduction 1 – Zahra Khan
01:26 Guest Introduction 2 – Sayantani DasGupta
02:40 Background and Inspiration for Guests
13:45 Narrative Medicine in the Clinical Setting
23:45 Role of Narrative in Abolition Medicine
37:10 How does storytelling impact your clinical work and vice-versa?
42:00 Abolitionist reimaginings of Health
55:05 Democratizing Narrative Medicine
1:03:05 Closing Remarks and Clinical Pearls
Speaker biographies (Abbreviated)
Zahra Khan is an educator and editor whose work emerges at the intersection of narrative, healing and disability justice, and liberation pedagogy. Her research, writing, and community engagement focuses on shifting consciousness in medical education toward abolitionist possibilities. Zahra enjoys facilitating spaces that cultivate critical consciousness, earnest reflection, and collective care. Her work has appeared in publications such as the Lancet, Journal of Medical Ethics, and AMA Journal of Ethics. She currently works with Project NIA, a nonprofit dedicated to ending youth incarceration, and teaches in the graduate program in Narrative Medicine at Columbia University and at CUNY School of Medicine.
Sayantani DasGupta is a faculty member in the Master’s Program in Narrative Medicine, the Center for the Study of Ethnicity and Race and the Institute for Comparative Literature and Society, all at Columbia University. Originally trained in pediatrics and public health, her work has appeared in journals including The Lancet, JAMA, Pediatrics, The Hastings Center Report, Literature and Medicine, Teaching and Learning in Medicine, and The Journal of Medical Humanities. She is an associate editor of the journal Literature and Medicine, and her current interests are in issues of narrative humility in medical education and practice, racial justice and health, diaspora studies, and science fiction/health futurities. She is also a New York Times bestselling children’s author. Learn more about her work at www.sayantanidasgupta.com.
Episode Takeaways
Origin Stories – Zahra encountered abolition for the first time at the ‘Beyond the Bars’ Conference, where she encountered students and community members from all backgrounds who were dedicated to ending mass incarceration. Here, she encountered Angela Davis, where she was encouraged to reimagine and build frameworks that center justice and do not reproduce oppression. She started in the Narrative Medicine program at Columbia around Sayantani, and wanted to focus on incarceration as a healthcare issue, and has since engaged in work that attempts to decarcerate health care. Sayantani became a physician since she thought it was a concrete tool for social justice. She came from an activist family, with her mother being one of the first South Asian feminist activists in the country. She grew up among stories of activist struggle and decolonial movements, and discovered a lot around the frameworks in medicine as she navigated her medical education. She discovered narrative medicine, and to her, it was about finding and retelling individual and structural stories in antiracist ways. Now, she teaches undergraduates and graduate students at the intersections of stories, social justice, and health. Part of her journey has been imagining how abolition and medicine go together, thinking through the carceral logics that have built medicine, and reimagining a new form of medicine with a liberatory practice.
Role of Narrative Medicine in the Clinical Setting – Narrative Medicine is often called different things in different places; it is called health humanities in some places, to decenter the physician in the health care team, and Sayantani is a fan of this terminology. What the term gestures towards is the centering of the ‘story’ in healing relationships. However, it is important to think about individual stories within the broader historical and sociocultural context; for instance, you cannot highlight stories in individual physician-patient dyads, without discussing mechanisms of racialized, historical, or sociocultural power and other larger structural forces. Listening to individual stories within the context of their structural stories is important. Stories are not inherently just. It is important to be critical of stories, and we must train individuals to recognize stories that dehumanize groups of people and transform them into more just stories that humanize everyone.
For instance, Toni Morrison’s “Home” depicts scenes of a community of Black women nursing a woman who has been the victim of medical racism and violence. It helps us understand Morrison’s critiques of anti-Black racism in medicine, and better understand care, restoration, and safety too. This helps people think about how people tend to each others’ well-being in their communities as well. It also helps illustrate the power of witnessing and mutual recognition, where there is a narrative exchange between patient and provider, with a validation of patients’ suffering. Apart from this, this also helps practitioners in improving their capacity to develop empathy for their patients, to be more curious about, and appreciate the complex context of those they care for.
Narrative in Abolition Medicine: Zahra explains that structural competency is a framework that Jonathan Metzl and Helena Hansen offer to understand structural factors and barriers to care that perpetuate worse health outcomes like housing, food, and water as upstream factors that lead to worse health. Sayantani and Zahra (along with Yoshiko Iwai) have written about policing to be another one of these upstream factors that affect health, and offer ‘abolition medicine’ as a framework. Medicine often has a role in caring for those impacted by police brutality, and it should also have a role in creating new visions for violence prevention and reenvisioning healthcare without relying on carceral logics. It involves understanding stories and their relationships to power and structural oppression. Narrative medicine can offer us an imaginative space to create change. “Practicing New Worlds”, a book by Andrea Ritchie, talks about visionary fiction to help us look towards abolitionist futures, and can even help us reimagine new possibilities for health care. Sayantani expands on this to discuss the class she teaches on the relevance of visionary medicine, speculative fiction, and imagining an antiracist health system. Abolition Medicine itself involves recognizing and dismantling the carceral logics baked into medicine, and looking outside of medicine to see how we might reimagine these structures to improve health.
How does storytelling impact your clinical work, and how does clinical work impact storytelling? – As a pediatrician, Sayantani shares that physical health, corporeal health, intellectual health, and imaginative health can be thought of as a part of the same praxis. Childrens’ fiction has always been about imagination, and it creates paths forward and gives young people the ability to imagine acts of justice within the storyteller’s own stories.
Abolitionist reimaginings of health – Zahra talks about the piece she wrote with Yoshiko and Sayantani, and talks about how they wrote this piece in the backdrop of the American Medical Association recognizing systemic racism as a public health crisis, and acknowledging that police violence has severe health consequences. They realized that if policing and prisons are systems that require abolitionist reimaginings, health care does too. Ruth Wilson Gilmore, an abolitionist scholar and geographer, uses the term ‘organized abandonment’ to describe what happens when communities lose protections from the state through systems and structures that are involved in disinvestment from communities, leading to these communities being more vulnerable to increased criminalization and police presence, and resulting in these communities lacking safe and just infrastructure in the form of housing options, lack of access to clean and safe water, transportation, etc. For instance, the presence of police and ICE officials in health care settings, along with the use of restraints, are examples of the ways policing has permeated medicine as well. And we have examples of mutual aid networks and organizations that worked to improve care in the setting of organized abandonment; some of these include the Black Panther Party providing free healthcare in communities, and the Puerto Rican activist organization ‘The Young Lords’ ensuring their community receives tuberculosis screenings. There are also more contemporary organizations doing this work; Zahra works with Mental Health First, organized by the Anti Police-Terror Project, a multiracial, intergenerational, mobile, crisis-intervention team led by mental health officials to provide life-affirming treatment and deescalation assistance, without having to rely on law enforcement. This offers a framework for abolitionist and non-carceral solutions that can be implemented around the world.
Sayantani shares that the medical system and carceral system work hand-in-hand and it is not possible to decarcerate medicine or practice antiracism in medicine without acknowledging the carceral logics that permeate medicine and that the medical industrial complex is a part of the carceral system. This is a prerequisite to dismantling oppressive systems within medicine.
Democratizing Narrative Medicine – Zahra says that one of the loudest aspects of narrative medicine that is most powerful is using ‘story’, staying with narratives, and close reading and listening of story. Democratizing narrative medicine is also a matter of breaking open institutions to make knowledge and information more accessible to the public. Zahra also expresses hope around the spread of narrative medicine to the mainstream, and thinks that it might help more people organize around the story. However, institutions are only one place where actions happen, and actions within the institution often remain within the institution. So, it is important to consider how we might use narrative to advance social justice outside of institutions and in the world. Sayantani adds that there is a reason that certain voices are kept away from the fore, and that there are structural forces that are doing so intentionally. For instance, book bans around the country exist because states recognize the radical power of ‘story’ and it is the reason that they attempt to suppress the spread of these stories. Stories are imaginative playgrounds for social change. She even adds that she prescribes reading in a clinical setting, both for the parent to the child and by the child themselves. It is also important to recognize that teachers and librarians that attempt to get banned stories in the hands of their students are also engaged in this work of democratizing narrative medicine.
Pearls
Zahra says that there are so many resources that help us practice and imagine new futures now, and shares with listeners these resources. One of these include Interrupting Criminalization – Beyond Do No Harm is one network of U.S. based health practitioners, advocates, nurses, community members, educators, social workers, and others who are working across racial, gender, reproductive, migrant and disability justice, drug policy, sex worker, and anti-HIV criminalization movements. Another is an Interrupting Criminalization podcast called One Million Experiments, that shares projects that are happening all over the country that build transformative solutions to safety without relying on police and prisons. Another thing Zahra mentions is that we must all be cartographers in mapping out new possibilities of an antiracist health care that satisfies all of us. As Mariame Kaba says, this is an opportunity to shrink the space between our values and our actions, and this is a collaborative and collective project where she invites everyone to think about their role in advancing health and justice.
Sayantani encourages listeners of this podcast not to feel overwhelmed. So many times, we take care of others’ needs better than our own, and there is a sense of exhaustion, frustration, and anger that many face from medical training. We must strive to change the violent carceral logics that medical training and education inculcates, and also remember that we do not have to do everything alone and that we are not alone in this work. Rather than viewing it as one more thing to do, it is easier to become learners again, where we view antiracism as a new philosophy of living, learning, and working, and just taking it one step at a time.
Metzl JM, Hansen H. Structural competency: theorizing a new medical engagement with stigma and inequality. Soc Sci Med. 2014 Feb;103:126-133. doi: 10.1016/j.socscimed.2013.06.032. PMID: 24507917; PMCID: PMC4269606.
Khan Z, Iwai Y, DasGupta S. Military metaphors and pandemic propaganda: unmasking the betrayal of ‘Healthcare Heroes’. Journal of Medical Ethics. 2021;47:643-644.
Khan ZH, Iwai Y, DasGupta S. Abolitionist Reimaginings of Health. AMA J Ethics. 2022 Mar 1;24(3):E239-246. doi: 10.1001/amajethics.2022.239. PMID: 35325526.
Ritchie, Andrea J. Gumbs, Alexis Pauline. Brown, Adrienne Maree. (2023). Practicing new worlds: Abolition and emergent strategies. Consortium Book Sales & Dist.
The hosts and guests report no relevant financial disclosures.
Citation
Khan Z, DasGupta S, Krishnamurthy S, Cooper A, Siddiqui H, Calac A, Pitre A, Pierce G, Essien UR, Fields NF, Lopez-Carmen V, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Leveraging Narrative Medicine to Cultivate Antiracist Praxis.” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. February 13, 2024.
Sharmin and Kaylin sit down with Dr. Denise Davis to discuss communication as a procedure, continuous and incremental improvement, and the interrelationship between social and health justice
Denise L. Davis is a general internist and Clinical Professor of Medicine at University of California San Francisco. She serves as Associate Director for Faculty Development for the SanFrancisco VA Center of Excellence in Primary Care Education. Dr.Davis teaches locally and nationally on a range of topics, including teaching and coaching students, trainees and physicians in communication skills that increase quality, safety and improve patient experience. She is on the Executive Committee of the Academy on Communication in Healthcare and serves as VP of Diversity, Equity and Inclusion. She is also a specialist for minority medical students at UCSF School of Medicine. Dr. Denise Davis is a recipient of many awards, includingthe prestigious Kaiser Foundation Award for Excellence in Teaching and she was elected to the UCSF Academy of Medical Educators in 2015.
In this Rheumatology Rafael Medina Subspecialty episode, Dr. John Landefeld presents a case to Dr. Sarah Goglin of a 74 year old woman presenting with headache.
The goal of this session is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case discussant: Dr. Sarah Goglin is a rheumatologist and associate director at Zuckerberg San Francisco General Rheumatology clinic and at the UCSF Vasculitis Clinic. @SarahGoglinMD
Case presenter: Dr. John Landefeld is an internist and medical educator at Sacramento County Public Health & an assistant Clinical Professor at UC Davis Health. @johnlandefeld
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Kirtan presents a case of generalized weakness to Vivek and Hannah.
Kirtan Patolia is a second-year Internal Medicine resident from John H. Stroger Jr., Hospital of Cook County, Chicago. He relishes being the CPSolvers team member, as solving cases and generating differential diagnoses are his biggest passions. You will frequently find him sharing clinical cases on VMR. Outside of medicine, he likes to read fiction, particularly Agatha Christie and Nancy Drew novels. He also loves kite flying, especially using various techniques and maneuvers to fly the kites.
Vivek Paul
@vjpaul88
Vivek Paul is a medical graduate from Bharati Vidyapeeth University in Pune (India), now based in Chicago, Illinois. Having worked as a junior doctor in India after completing medical school, Vivek has more recently been involved in clinical research at Northwestern University Feinberg School of Medicine and is working towards a residency in Internal Medicine. He is also an avid musician with a Spotify account where he releases songs he has written through the years. When not working, Vivek can be found making loud and angry music, playing tennis, exploring local food joints, or on long walks with his dog, Melody.
In this Hepatology Rafael Medina Subspecialty episode, Dr. Christopher Coe presents a case to Dr. Arpan Patel of a woman presenting with fatigue and splenomegaly.
The goal of this series is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case Discussant: Dr. Arpan Patel is a hepatologist and researcher at UCLA. @ArpanPatelMD
Case Presenter: Dr. Christopher Coe is Chief GI fellow at UCLA. @CCoeMD
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Valeria presents a case of frequent stumbling to Nilayan and Subhangi.
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue Neurology residency. Her interests include neuro-infectious diseases, transgender health and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine she loves running, hiking, cooking pasta and spending time with her dogs.
Nilayan Sarkar
@nilayansarkar
Nilayan is a first year Internal Medicine Resident at Lady Hardinge Medical College in New Delhi, India. He has been an avid fan of the CPSolvers since his third year of medical school. Clinically, his interests include Point of Care Ultrasound (POCUS), Critical Care, Cardiology and Medical Reasoning. Outside of work, Nilayan enjoys quiet evening walks with his family, meditation, and nature jaunts. He hopes this episode brings you as much joy as it did to him and believes Dr. Aaron Berkowitz is the best thing that has ever happened to #beatingNeurophobia.
Episode 310 – WDx Episode #26: “You are Resilient, even if You Don’t Know It”
Nov 09, 2023
https://clinicalproblemsolving.com/wp-content/uploads/2023/11/WDx-11.9.23-RTP.mp3Sharmin, Kaylin, and Jane are joined by Dr. Risheen Reejhsinghani, cardiologist extraordinaire, Clinical Associate Professor at Stanford, and Associate Program Director of the cardiology fellowship. They discuss her journey through medical training as an international medical graduate, how her love for cardiology developed, and how her career has evolved to allow her to combine her passions for medical education and mentoring into her daily work. Dr. Risheen Reejhsinghani is a Clinical Associate Professor in the Division of CardiovascularMedicine at Stanford. She was born in Mumbai, India, where she attended medical college, after spending her early school years in Sydney, Australia. Risheen moved to Boston for residency atSt. Elizabeth’s Medical Center and completed a cardiology fellowship at Baystate Medical Center, the western campus of Tufts University. She then completed an advanced echocardiography fellowship at the University of California, San Francisco.During fellowship, under combined cardiology and rheumatology mentorship, Risheen developed a clinical focus in cardio-rheumatology. This led to the creation of the StanfordCardio-Rheumatology Program, to provide specialized care to patients with cardiac pathology as a direct consequence of autoimmune disease. Risheen cares deeply about medical education and mentorship, and is an Associate Program Director for the CardiovascularMedicine Fellowship, where working closely with fellows is the absolute best part of her role. In the School of Medicine, she serves as an Associate Course Director for the pre-clerkshipPractice of Medicine Course, and is faculty co-lead for the cardiopulmonary block. Her scholarly work addresses curricular interventions and novel methods of teaching to improve education delivery, with the ultimate goal of increasing global access to education for medical trainees.Outside of medicine, Risheen enjoys writing and used to freelance for a newspaper in India.Along with her husband, she tries to travel as frequently as possible and loves learning about local cultures and traditions in the US and internationally. An ardent enthusiast of the alternative rock scene, Risheen has been an unwavering fan of the band Nirvana since well before she could read an EKG.
Episode 23 – Anti-Blackness, Anti-Fatness, and Food Shaming
Show Notes by Humza A. Siddiqui
October 31, 2023
Summary: This episode highlights the culture of food shaming and anti-fatness as it relates to anti-Blackness. During this episode, we hear from Da’Shaun L. Harrison, a community organizer and trans theorist, and Dr. Psyche A. Williams-Forson, an author and chair of the Department of American Studies at the University of Maryland. Together, our guests offer context around the history of anti-Blackness and how it is deeply intertwined with the culture around eating in America as well as the way anti-fatness manifests. Further, they expand on this to discuss how it relates to policing and the court systems in the U.S. This discussion is hosted by Sudarshan Krishnamurthy and Ashley Cooper. The show notes for this episode were written by Humza A. Siddiqui.
Episode Learning Objectives
After listening to this episode, learners will be able to
Explain how anti-fatness and food shaming culture in the U.S. is rooted in anti-Blackness.
Describe the intersection of policing and the court systems with anti-fatness and food shaming.
Identify ways to navigate clinical interactions with patients while respecting them and affirming their experiences with food and fatness.
Credits
Written and produced by: Sudarshan Krishnamurthy, Ashley Cooper, Team
Hosts: Sudarshan Krishnamurthy and Ashley Cooper
Infographic: Creative Edge Design
Audio Edits: Ashley Cooper and Noah Nakajima
Show Notes: Humza A. Siddiqui
Guests: Dr. Psyche A. Williams-Forson, Da’Shaun L. Harrison
Time Stamps
00:00 Opening
00:45 Introductions
03:07 Guest Introduction 1
04:46 Guest Introduction 2
08:15 On the Intersection of Black, Fat, and Trans Communities and the Medical-Industrial Complex
13:35 History and the Racial Underpinnings of Food Shaming in the U.S. Landscape
21:48 Policing, the Court Systems, Anti-Blackness, and Anti-fatness
46:45: Language Matters: The War On Obesity
1:02:09 On Caring For Black, Fat, and Trans Patients
1:15:37 Fatness is Not Killing People and Other Pearls
1:21:25 Closing Remarks
Speaker biographies (Abbreviated)
Dr. Psyche Williams-Forson is a Professor and Chair of the Department of American Studies at the University of Maryland College Park. She is the author of two award winning books: Eating While Black: Food Shaming and Race in America (James Beard Foundation) and Building Houses Out of Chicken Legs: Black Women, Food, and Power (American Folklore Society); as well as the co-edited Taking Food Public: Redefining Foodways in a Changing Food World. Her work can also be found in several other publications and on podcasts and documentaries. Dr. Williams-Forson received her BA from the University of Virginia and her MA and PhD in American Studies from the University of Maryland.
Da’Shaun Harrison is a trans theorist and Southern-born and bred abolitionist in Atlanta, Georgia. They are the author of Belly of the Beast: The Politics of Anti-Fatness as Anti-Blackness, which won the 2022 Lambda Literary Award for Transgender Nonfiction and several other media/literary honors. As an editor, movement media and narrative strategist, and storyteller, Harrison uses their extensive history as a community organizer—which began in 2014 during their first year at Morehouse College—to frame their political thought and cultural criticism. Through the lens of what Harrison calls “Black Fat Studies,” they lecture on blackness, fatness, gender, and their intersections. Harrison currently serves as Editor-at-Large at Scalawag Magazine, is a co-host of the podcast “Unsolicited: Fatties Talk Back,” and one third of the video podcast “In The Middle.” Between the years 2019 and 2021, Harrison served as Associate Editor—and later as Managing Editor—of Wear Your Voice Magazine.
Episode Takeaways
Origin Stories – For Dr. Psyche A. Williams-Forson and Da’Shaun L. Harrison, the work that they do is deeply informed by the history of chattel slavery in the United States, through which eugenicists, white anthropologists, and racial realists created entire disorders to medicalize and bastardize enslaved folks who were interested in freedom. Natal alienation is, in part, the under-structure of the wider Medical-Industrial Complex and the gratuitous violence that fat, Black, trans folks experience. All of this contributes uniquely to social death.
Soul Food – Food cultures are more complex, multilayered, and storied than Black stereotypes will lead even Black communities to believe. For this reason, labeling food in categories, and the moralizing that follows, can be extremely dangerous. A toxic cycle of disordered eating can emerge, and treatment for recovery can be rooted in anti-Blackness as physicians view the Black habitus as out of control, unruly, not in conformance with a wider racial project as described by Michael Omi and Howard Winant. The developing attitudes about food scarcity and deficit models, and mass media’s manufacturing consent, has to be challenged, especially because there is a deep and rich history of Black people as farmers, gardeners, and ranchers that belies what Chimamanda Ngozi Adichie calls the danger of a single story.
Afterlife of Slavery – We are living in what Saidiya Hartman calls the Afterlife of Slavery, in where skewed life chances, limited access to health and education, premature death, and surveillance, incarceration, and impoverishment are overdetermined by slavery’s racial calculus. Da’Shaun L. Harrison explains the role of fatness in all of this and offers examples across medicine, law, and sociology that demonstrate fatness and Blackness cannot be divorced from each other. Dr. Williams-Forson expands on this history with respect to Black women, whose bodies are fetishized, and Black children, whose bodies are adultified, respectively. All of this contributes to various mental health challenges that are consistent with surveillance in not only a wider police-state but also the patient-physician relationship.
The War on Obesity – We cannot make recommendations to our Black and Brown patients about diet and exercise without acknowledging that white supremacy is statistically more likely to kill Black and Brown patients than obesity. The conditions through which the United States’ socio-politico-economic apparatus is maintained, and the cultural mores that we encourage as a society, make it difficult for Black and Brown patients to eat a healthy diet or move their bodies freely.
Fatness is Not Killing Black People – Historically, what is killing Black people is a medical industry that is not primarily built to offer care and is otherwise disinterested in learning more about the experiences of Black bodies. Anti-obesity initiatives that aim to reduce weight and encourage healthy diet and exercise, while they may nudge choices on a population level and put pressure on corporations in their harmful advertising, may be reductive in their understanding of fatness as a function of obesity. Fat people can lead healthy lives, and we need to think about the structural issues that keep the populace from being healthy at all sizes. This demands teleological explanations and policy interventions. On one hand, we must not moralize food choices. On the other hand, we cannot let hyper-capitalism off the hook, especially those industries that target Black and Brown communities and seek to profit from the manufactured consent that lends itself to insecurities about weight loss or weight gain.
Pearls
Respect cultural mores about diet and exercise. Acknowledge that Black and Brown patients understand their bodies at some level and what sustains them nutritionally. Be precise instead about the care we can offer beyond weight loss.
Fatness is not killing Black people. However, consider that Black patients are navigating disordered eating as a function of moralizing their food choices under white supremacy and a standard of care that was created by eugenicists, white anthropologists, and racial realists that inappropriately value the heterosexual, cis-gender, white European male habitus.
References
Cox, J. (2020). Fat girls in Black bodies: creating communities of our own. North Atlantic Books.
Harrison, D. (2021). Belly of the Beast: the politics of anti-fatness as anti-blackness. North Atlantic Books.
Taylor, S. R. (2018). The body is not an apology: the power of radical self-love (First Edition). Berrett-Koehler Publishers.
Williams-Forson, P. A. (2022). Eating while Black: food shaming and race in America. The University of North Carolina Press.
The hosts and guests report no relevant financial disclosures.
Citation
Harrison DL, Williams-Forson P, Cooper A, Krishnamurthy S, Siddiqui H, Calac A, Pitre A, Pierce G, Essien UR, Fields NF, Lopez-Carmen V, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Anti-Blackness, Anti-Fatness, and Food Shaming” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. November 7, 2023.
In this Infectious Disease Rafael Medina Subspecialty Episode, Dr. Navila Sharif presents a case to Dr. Natasha Spottiswoode of a patient presenting for fevers and chills.
Session facilitator: Youssef Saklawi
The goal of this series is to provide greater access to subspecialty, primary care, and internal medicine-adjacent specialty education for learners worldwide. For those interested in participating as a case presenter or discussant (or to nominate an educator or attending), the nomination form is available here.
Natasha is a fellow in the Division of Infectious Diseases at the University of California, San Francisco. Her interests include the use of combined host-pathogen metagenomics to diagnose and treat critically ill patients, and the development of better treatments for patients with rare infectious syndromes. She also loves climbing, trail running and backcountry skiing.
Case Presenter: Navila Sharif, MD
Navila is a second year internal medicine resident at Emory University in Atlanta, GA. She is passionate about health equity and advocacy, and is interested in general hospital medicine and gastroenterology, with a keen interest in transplant hepatology. Outside of work, she enjoys exploring coffee shops, binging reality TV, and any hike with the promise of a view.
To join us live on Virtual Morning Report (VMR), sign up HERE.
Sharmin, Jack, and Maddy discuss their approaches to severe acute liver injury, abdominal pain, and hyperferritinemia as they talk through a case presented by Ann-Marie.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Vaness presents a case of shallow breathing to Maria and Sridhara.
Vanessa, a proud Filipino through and through, has dedicated herself to medicine. She has been serving her countrymen since earning her medical degree. Practicing in areas of limited resources, she has sharpened her clinical eye allowing her to realize her passion for neurology where localizing lesions is as intellectually stimulating and satisfying as a daily crossword puzzle. Her interests include cognitive neurology, vascular neurology, and neurocritical care. A true “jill of all trades”, she is always down for a new adventure. She has explored dance and theater, film and photography, various musical instruments, different languages, and swimming. At home, you are most likely to find her in the kitchen preparing your new favorite meal
Maria Jimena Aleman
@MariaMjaleman
María Jimena Alemán was born and raised in Guatemala where she currently works in community and rural health care. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Ella Fitzgerald. Outside of medicine, she enjoys modern art, 21st century literature, and having hour-long conversations over a nice hot cup of coffee or tequila.
Sridhara Yaddanapudi
@syaddana_neuro
Sridhara is a board-certified internist, neurologist, vascular neurologist, and hypertension specialist. Currently, he holds the position of Clinical Assistant Professor at Thomas Jefferson University Hospital and serves as the Director of Neurology for Jefferson New Jersey.
As a medical professional, he is passionate about case-based learning, clinical reasoning, and teaching decision-making while avoiding the pitfalls of heuristics. His goal is to bridge the ever-growing gap between neurology and internal medicine, an area in which he has a keen interest.
The spaced learning series team discusses a case of a patient with hyperbilirubinemia secondary to acute alcoholic hepatitis, who then developed hypoxia and hemolysis.
Sharmin & Kaylin are joined by María Jimena Alemán, CPSolvers co-director of internal operations & future neurologist with a passion for global health. They discuss how her upbringing has informed & shaped her passions & values, how she got involved with CPSolvers, the growth that comes from being a leader, the power of community & good mentor-mentee relationships.
María Jimena Alemán was born and raised in Guatemala where she currently works in community and rural health care. After suffering from long-standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She looks forward to dedicating her life to breaking barriers for Latin women in the medical field and improving neurology care around the world. She loves being a part of The Clinical Problem Solvers where she serves as the co-director of internal operations alongside Madellena Conte. Her life soundtrack is a mix between Shakira and Ms. Lauryn Hill. Outside of medicine, she enjoys contemporary art, crossword puzzles, and having hour-long conversations over a nice hot cup of coffee or tequila.
Kaylin Nguyen is a non-invasive cardiologist with interests in medical education, women in medicine, and health disparities. She was born in Vietnam and grew up in Southern California. She completed medical school and Internal Medicine residency at UCSF. She then made her way down the peninsula to Palo Alto, where she completed cardiology fellowship at Stanford, serving as a chief fellow. She is super excited to be back in Los Angeles and to help care for the underserved community as a clinician-educator at Olive View-UCLA Medical Center. Outside of medicine, you can find her hiking with her dog, making (and eating) baked goods, and buying and neglecting plants*.
In this Gastroenterology Rafael Medina Subspecialty episode, Dr. Allyson Richardson presents a case to Dr. Ryan Flanagan of a 68 year old woman presenting with chronic diarrhea.
The goal of this session is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case discussant: Dr. Ryan Flanagan is a gastroenterologist and faculty member at the Brigham and Women’s Hospital and Instructor in Medicine at Harvard Medical School in Boston. He has a clinical focus on the inpatient GI consult service and is the Associate Program Director for the Gastroenterology Fellowship Program.
Case presenter: Dr. Allyson Richardson is a second year Gastroenterology/Hepatology fellow at Brigham and Women’s Hospital.
Episode description: We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, María presents a case of clumsiness to Andrea and Sridhara.
Andrea is a Venezuelan medical doctor and cognitive neuroscientist specializing in advanced white matter imaging. She recently completed a Ph.D. in Cognitive Neuroscience from Colorado State University, USA, and is currently a postdoctoral researcher at the BRAiN Lab in Colorado. Andrea is also actively involved in initiatives supporting neurology applicants (e.g., @NMatch2024) and research career development for international medical graduates. In her free time, she is usually playing guitar or climbing a mountain!
Sridhara Yaddanapudi
@syaddana_neuro
Sridhara is a board-certified internist, neurologist, vascular neurologist, and hypertension specialist. Currently, he holds the position of Clinical Assistant Professor at Thomas Jefferson University Hospital and serves as the Director of Neurology for Jefferson New Jersey.As a medical professional, he is passionate about case-based learning, clinical reasoning, and teaching decision-making while avoiding the pitfalls of heuristics. His goal is to bridge the ever-growing gap between neurology and internal medicine, an area in which he has a keen interest.
Maria Jimena Aleman
@MariaMjaleman
María Jimena Alemán was born and raised in Guatemala where she currently works in community and rural health care. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Her life probably has a soundtrack of a mix between Shakira and Ella Fitzgerald. Outside of medicine, she enjoys modern art, 21st century literature, and having hour-long conversations over a nice hot cup of coffee or tequila.
In this episode of WDx, Dr Casey Albin joins Kiara, Jane, & Sharmin to discuss a clinical unknown. Presented by Kiara, the case starts with the chief concern of difficulty recognizing family members.
Casey Albin, MD is an Assistant Professor at Emory University School of Medicine where she is a member of the department of Neurocritical Care. She completed both her neurology residency and a fellowship in Medical Simulation at Harvard Medical School/Partners Neurology before completing a fellowship in Neurocritical Care at Emory. Dr. Albin’s research interests focus on educational innovations in acute neurologic emergencies and neurocritical care. In addition to running simulation courses, she is the editor of The Acute Neurology Survival Guide and is passionate about open access neurologic education through Twitter, EMCrit, and podcasts.
Episode 296 – RLR – A curious case of cough
Jul 19, 2023
In this Infectious Disease Rafael Medina Subspecialty episode, Dr. Jorge Salazar presents a case to Dr. Monica Gandhi of a transgender woman with a recent diagnosis of HIV presenting with fatigue and weight loss.
The goal of this series is to expand access to subspecialty, primary care, and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant (or nominate an attending/educator), fill out the form HERE.
Case discussant: Monica Gandhi MD, MPH is Professor of Medicine and Associate Division Chief of the Division ofHIV, Infectious Diseases, and Global Medicine at UCSF/San Francisco General Hospital. She also serves as the medical director of the HIV Clinic at SFGH (“Ward 86”).
Case presenter: Jorge Salazar is an Infectious Disease Fellow at the University of California, San Francisco. He also serves as an AIDS Research Institute Clinical Fellow and provides integrated HIV care for patients at Ward 86.
Episode 293 – Antiracism in Medicine Series – Episode 22 – Live from SGIM 2023: Best of Antiracism Research at the Society of General Internal Medicine’s 2023 Annual Meeting
Jun 27, 2023
Episode 22 – Live from SGIM 2023: Best of Antiracism Research at the Society of General Internal Medicine’s 2023 Annual Meeting
Show Notes by Alec J. Calac
June 22, 2023
Summary: This episode highlights a selection of antiracism research presentations at a live recording of the podcast at the 2023 SGIM Annual Meeting. This year’s episode, our third conducted at SGIM, is focused on the importance of language in medicine and the role it can play in perpetuating stigma and bias. During this episode, we hear from Dr. Som Saha, an internist whose research focuses broadly on the influence of race and racism in the doctor-patient relationship among other research subjects, Dr. Mary Catherine Beach, whose work has been targeted towards improving healthcare quality for patients who face systemic disadvantage especially in the setting of HIV/AIDS and sickle cell disease, and Dr. Pooja Lagisetty, whose work is focused on understanding how stigma impacts access to care for people living with chronic pain and opioid use disorder. This episode is hosted by Sudarshan (Sud) Krishnamurthy and Ashley Cooper. The show notes for this episode were written by Alec Calac.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Differentiate between stigma and bias in health care and the electronic health record using provided examples.
Describe difficulties and examples of how to measure unconscious race bias in medical practice.
Identify strategies to mitigate bias and stigma in the electronic health record as a trainee and medical practitioner.
Credits
Written and produced by: Sudarshan Krishnamurthy, Ashley Cooper, Team
Hosts: Sudarshan Krishnamurthy, Ashley Cooper
Infographic: Creative Edge Design
Audio Edits: Madellena Conte
Show Notes: Alec J. Calac
Guests: Dr. Som Saha, Dr. Mary Catherine Beach, Dr. Pooja Lagisetty
Time Stamps
0:00 Opening
00:23 Introductions
01:50 Guest Introduction 1
02:43 Guest Introduction 2
04:05 Guest Introduction 3
05:25 Guest Career Paths and SGIM Research
07:20 Anti-Racist Praxis and Sickle Cell Clinical Research/Scale Development
10:00 Unconscious Race Bias
16:30 Positive, Negative, Neutral Language in the Electronic Health Record
19:54 Use Language to Personalize and Humanize Notes
21:22 Considerations for Alternative Language
25:20 “Disbelief of Pain” and Scare-Quotes
26:45 Interrupt Transmission of Stigma in the Electronic Health Record
29:20 Beginning of Audience Questions and “Euphemism Treadmill”
35:00 Reorienting Language
38:00 “Value” in the Electronic Health Record
40:00 Question about “Positive Language” as a Tool
42:00 Language and Intended Audiences, Context
45:50 Question on Multi-Level and/or System-Level Interventions
48:00 Becoming Conscious about the Unconscious
49:35 “Thinking Fast and Slow”
50:30 Question on Person-First Language and Artificial Intelligence
53:50 Pearls and “Ending with Hope”
Speaker Biographies (Abbreviated)
Dr. Som Saha received his medical degree and post-graduate training in internal medicine from the University of California, San Francisco, and completed post-doctoral training in the Robert Wood Johnson Clinical Scholars Program (RWJ) at the University of Washington, where he obtained a master’s degree in public health. He subsequently worked at OHSU and the Portland VA for 2 decades before moving to Johns Hopkins University. Dr. Saha’s research focuses broadly on the influence of race and racism in the doctor-patient relationship, its relation to disparities in the quality of health care, and its implications for diversity in the healthcare workforce. He has also served as a Council member and Secretary of SGIM. He has been a research advisor or mentor for over 50 students, fellows, and junior faculty, over a third of whom have been from racial/ethnic groups underrepresented in medicine.
Dr. Mary Catherine Beach is a professor in the School of Medicine, with appointments in the Center for Health Equity and the Berman Institute of Bioethics, at Johns Hopkins University. Dr. Beach’s research focuses on humanizing healthcare by promoting respect for patients as well as improved patient-clinician communication. Much of her work has been targeted toward improving healthcare quality for patients who face systemic disadvantage and in the setting of HIV/AIDS and sickle cell disease (SCD). Her research has been funded by the National Institutes of Health, the Agency for Healthcare Research and Quality, the Robert Wood Johnson Foundation, and the Greenwall Foundation. Dr. Beach has won numerous awards for her scholarship and mentorship, including the David Levine Mentoring Award from the Johns Hopkins School of Medicine in 2015. She also is the 2017 recipient of the George L. Engel Award for outstanding research contributions to the theory, practice, and teaching of effective healthcare communication and related skills. In 2022, Dr. Beach was elected as a Hastings Center Fellow; and in 2023 was awarded the Excellence in Ethics Award from the Society of General Internal Medicine.
Dr. Pooja Lagisetty received her medical degree from the Johns Hopkins School of Medicine and completed her internal medicine residency at Massachusetts General Hospital. Following residency, she was a Robert Wood Johnson Clinical Scholar and received health services research methodology training. She is currently an Assistant Professor of Medicine in the Division of General Internal Medicine at the University of Michigan and also a research investigator at the Center for Clinical Management and Research at the Ann Arbor VA. Clinically, she is boarded in both Internal Medicine and Addiction Medicine and practices as a primary care physician and teaching hospitalist. Her research focuses on understanding how stigma impacts access to care for people living with chronic pain and opioid use disorder. She is also interested in designing multidisciplinary care models for people with comorbid pain and substance use disorders in the general medical setting.
Episode Takeaways
Stigma in Healthcare: Sud begins by asking our guests what led them to their current career paths and what work they are presenting at SGIM. Many of them share intersecting interests in stigma and other factors, such as chronic pain management, language (“drug-seeking” in the electronic health record), and the patient-provider relationship. Clinician-researchers are increasingly interested in developing novel scales and measures that can quantify stigma in healthcare. As noted by our guests, it is difficult to measure invisible factors such as unconscious race bias, because it is impossible to directly measure these factors. Instead, proxy factors, and other types of experimental inquiry (e.g., qualitative methods) have to be used to describe the impact that factors like bias have in health care. Importantly, there is a lot of nuance around language. It may be difficult to discern the impact that stereotypical language can have in health care because language is very contextual and means different things to different groups.
Stigma (Adverse Impact) vs. Bias (Personal Characteristic): Important to make a distinction between these two concepts. Society stigmatizes certain behaviors, such as drug injection and alcohol use. When a health care provider uses such language (e.g., a person who injects drugs), they may not have any bias against the patient, but they are using language that ascribes stigma to the patient based on societal norms. Another example of phrasing, such as “delightful” and “pleasant” may convey positive bias for one group of patients over another, depending on their racial and/or social identities, but may not be examples of stigma. It is not always clear what is an example of stigma and/or bias in the electronic health record. Learn more here: Negative Patient Descriptors: Documenting Racial Bias In The Electronic Health Record | Health Affairs
Use Language for Good: Think about what people will remember when they access a patient’s electronic health record. Language can be a powerful tool for good, especially in the backdrop of the opioid epidemic.
Opioid Epidemic and Stigma: Providers generally have a fear or discomfort using opioid agents as treatment for individuals with substance use disorders. Coupled with stigma, bias, and language used to describe these patients in the electronic health record, this perfect storm of factors can work against efforts to help patients in need of safe, comprehensive healthcare services.
Active Use of the Electronic Health Record: Be mindful of the use of “scare-quoting” and other phrasing that could be misinterpreted. Consider taking on an active role in interrupting the continued communication of language that is outdated and no longer relevant to the care of the patient. As mentioned earlier, humanizing the electronic health record can have a significant impact down the line.
“Euphemism Treadmill”: This describes the process of replacing words that have taken on a stigmatizing, pejorative, or derogatory connotation with new words that are more humanizing, and how this is an iterative (unlearning-learning) process. An interesting conversation followed that included discussions about the DSM in psychiatry and psychology (personal failing vs. medical disorder) and how this language-shifting process is likely multi-generational in scale.
Pearls
“Do no harm” through language. Be conscious about the words and phrases used in the clinical encounter and electronic health record. Preserve the dignity of the patient. Small changes can have a large impact.
Include personalizing and humanistic details in the electronic health record. The work begins with educating our learners, while incorporating these lessons into our clinical practice simultaneously.
References
Beach MC, Park J, Han D, Evans C, Moore RD, Saha S. Clinician Response to Patient Emotion: Impact on Subsequent Communication and Visit Length. Ann Fam Med. 2021 Nov-Dec;19(6):515-520. doi: 10.1370/afm.2740. PMID: 34750126; PMCID: PMC8575526.
Park J, Saha S, Chee B, Taylor J, Beach MC. Physician Use of Stigmatizing Language in Patient Medical Records. JAMA Netw Open. 2021 Jul 1;4(7):e2117052. doi: 10.1001/jamanetworkopen.2021.17052. PMID: 34259849; PMCID: PMC8281008.
Beach MC, Saha S. Quoting Patients in Clinical Notes: First, Do No Harm. Ann Intern Med. 2021 Oct;174(10):1454-1455. doi: 10.7326/M21-2449. Epub 2021 Aug 17. PMID: 34399061.
Beach MC, Saha S, Park J, Taylor J, Drew P, Plank E, Cooper LA, Chee B. Testimonial Injustice: Linguistic Bias in the Medical Records of Black Patients and Women. J Gen Intern Med. 2021 Jun;36(6):1708-1714. doi: 10.1007/s11606-021-06682-z. Epub 2021 Mar 22. PMID: 33754318; PMCID: PMC8175470.
Kosakowski S, Benintendi A, Lagisetty P, Larochelle MR, Bohnert ASB, Bazzi AR. Patient Perspectives on Improving Patient-Provider Relationships and Provider Communication During Opioid Tapering. J Gen Intern Med. 2022 May;37(7):1722-1728. doi: 10.1007/s11606-021-07210-9. Epub 2022 Jan 6. PMID: 34993861; PMCID: PMC9130417.
Benintendi A, Kosakowski S, Lagisetty P, Larochelle M, Bohnert ASB, Bazzi AR. “I felt like I had a scarlet letter”: Recurring experiences of structural stigma surrounding opioid tapers among patients with chronic, non-cancer pain. Drug Alcohol Depend. 2021 May 1;222:108664. doi: 10.1016/j.drugalcdep.2021.108664. Epub 2021 Mar 18. PMID: 33757709; PMCID: PMC8058315.
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Saha, S, Beach, M, Lagisetty, P, Cooper A, Krishnamurthy S, Calac A, Pierce G, Essien UR, Fields NF, Lopez-Carmen V, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 22: Live from SGIM 2023: Best of Antiracism Research at the Society of General Internal Medicine’s 2023 Annual Meeting” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. June 25, 2023.
Episode 291 – Juneteenth The H&P – History and Perspective – Stories and Conversations with Dr. Kimberly Manning and her Dad, Mr. William Draper, Sr
Jun 19, 2023
Dr. Kimberly Manning and her father, Mr. William Draper, commemorate Juneteenth, the holiday that celebrates the day when all remaining enslaved Black Americas were freed in Galveston Texas, on June 19th, 1865, with this hour-long storytelling event.
Episode 290 – Neurology VMR – Vertigo
Jun 15, 2023
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Dr. Gabriela Pucci presents a case of right arm weakness to Promise and Ravi.
Promise Lee @promiseflee
Promise Lee is currently a 3rd year medical student at Loyola University Chicago Stritch School of Medicine. She is an aspiring internal medicine physician with interests in GI, obesity medicine, public health, and clinical reasoning. Outside of medicine, Promise is a food and fitness enthusiast who loves enjoying the outdoors, spending time with family and friends, and experimenting with new recipes.
Gabriela Figueiredo Pucci @gabifpucci
Gabriela Figueiredo Pucci, MD, is a Neurology PGY 1 at University of Pittsburgh Medical Center. Originally from Brazil, she graduated from Unicamp and completed her first Neurology residency at UNESP. She is enthusiastic about breaking down complex Neurology topics into infographics on her website (www.Neudrawlogy.com). She is passionate about Clinical Reasoning and loves to be part of the CPSolvers. On her free time, she likes to travel, cook, bake, and watch competitive cooking and baking reality shows.
Ravi Singh @rav7ks
Ravi (Ravitej) Singh is originally from Greenwich, London U.K where he grew up playing soccer and rugby. He attended medical school at University of Debrecen, Hungary and completed residency at Medstar Harbor Hospital in Baltimore. Currently he is an associate program director for Sinai Hospital IM residency program in Baltimore as well as a Hospitalist on the teaching service. He is a faculty member at the Johns Hopkins School of Medicine and takes time out of his schedule to run a series of case-based teaching sessions as well as medical simulation with all of the medical students that rotate at Sinai throughout the year. He is also a co-chair of the ACP Maryland IMG committee where he advocates for IMG issues Jo and highlights their contributions to the healthcare system
In this episode of WDx, Dr Rebecca Berger joins Kara, Jane, & Sharmin to discuss a clinical unknown. Presented by Kara, the case starts with a young woman presenting with chronic isolated thrombocytopenia.
Dr. Rebecca Berger
Rebecca is an academic hospitalist and assistant professor of medicine at Weil Cornell Medicine and New York Presbyterian Hospital. In addition to her clinical work, she serves as the Director of Patient Safety for Inpatient Services for the Department ofMedicine and teaches medical students and residents, including leading small groups with students on their medicine clerkships focused on clinical reasoning and diagnosis.Rebecca obtained her undergraduate degree from Stanford University in 2009, her medical degree from Columbia University Vagelos College of Physicians and Surgeons in 2013, and completed her internal medicine internship and residency training at Massachusetts General Hospital (MGH) in 2016. She served as a NEJM Editorial Fellow from 2016-2017 and worked as a hospitalist at MGH before moving to Cornell in 2018.
Maddy Conte and Seyma Yildirim introduce a new series on the podcast: “The Rafael Medina Subspecialty Series,” which will always be in loving memory of our dear friend and CPSolvers family member, Dr. Rafael Medina. Rafa presents a nephrology clinical unknown to Drs. Ashita Tolwani and Mustafa Muhammad.
The goal of this series is to expand access to subspecialty, primary care and internal medicine-adjacent specialty education to learners around the world. If you would like to get involved as a case presenter or discussant, fill out this form here: https://forms.gle/RLbx6A2vELp6PTYp9
Case presenter and facilitator: Dr. Rafael Medina
Rafa was a Brazilian medical graduate who proudly shared on Twitter, “Son of a tailor and confectionary vendor born and raised in rural Brazil. And now incoming internal medicine resident at the University of Colorado. Never let anyone tell you that your dreams are too big for you!” He tragically passed away last week. He impacted the lives of so many and touched every corner of the CPSolvers community, and rippled far beyond. Rafa helped spearhead the subspecialty series; this series has been renamed after Rafa and will continue strong in his honor. Rafa, we love you.
Case discussants: Dr. Ashita Tolwani, Professor of Medicine at the University of Alabama at Birmingham (UAB). She was the Nephrology Fellowship Training Program Director from 2004-2010 and is now the Associate Program Director. She is also the Director for ICU Nephrology at UAB. (Twitter: luck_urine)
Dr. Mustafa Noor Muhammad, nephrology fellow at the University of Alabama at Birmingham.
Episode 285: Anti-Racism in Medicine Series – Episode 21 – Psychosocial and Cultural Considerations for Providing Healthcare to Immigrant and Refugee Populations
May 02, 2023
Episode 21 – Psychosocial and Cultural Considerations for Providing Healthcare to Immigrant and Refugee Populations
Show Notes by Kiersten T. “Gillette” Gillette-Pierce
May 2, 2023
Summary: This episode highlights the psychosocial and cultural considerations for providing healthcare to immigrant and refugee populations. During this episode, we hear from Dr. Altaf Saadi, a neurologist who focuses on neuropsychiatric health disparities and addressing the needs of displaced populations at Mass General Hospital and Harvard Medical School, and Dr. Naweed Hayat, a child and adolescent psychiatry fellow at the University of California San Diego, who applies his own lived experience of resettlement to his clinical practice. Together, our guests explain how trauma shows up in those who experience resettlement, and the role of trauma-informed and culturally-responsive care for refugee, asylee, and immigrant population in clinical practice.. This discussion is hosted by Sudarshan Krishnamurthy, Ashley Cooper, and LaShyra Nolen.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Explain how the current state at the border is informed by historical immigration injustices.
Describe how physiological and psychological trauma show up among immigrant and refugee populations as a result of the violence and injustices experienced during migration, at the border, during the resettlement process and across the lifecourse thereafter.
Identify the role of trauma-informed, culturally-responsive care for refugee, asylee, and immigrant populations and how it can be operationalized in clinical practice.
Credits
Written and produced by: Sudarshan Krishnamurthy, Ashley Cooper, LaShyra Nolen, Kiersten Gillette-Pierce, Rohan Khazanchi, MD, MPH, Dereck Paul, MD, Jazzmin Williams, Victor A. Lopez-Carmen MPH, Naomi F. Fields, Jennifer Tsai MD, MEd, Chioma Onuoha, Ayana Watkins, Michelle Ogunwole MD, Utibe R. Essien MD, MPH
Hosts: Sudarshan Krishnamurthy; Ashley Cooper, and LaShyra Nolen
Infographic: Creative Edge Design
Audio Edits: Garrett Weskamp
Show Notes: Gillette Pierce
Guests: Dr. Altaf Saadi and Dr. Naweed Hayat
Time Stamps
0:28 Introduction
0:31 Episode introduction
1:15 Guest introductions
3:50 Origin stories
8:06 The current state of the border
18:13 Culturally competent and trauma-informed care
24:50 ICE and policing
36:28 Application of teachings
Episode Takeaways
Origin Stories — For Dr. Hayat and Dr. Saadi, the work that they do is deeply informed by their lived experiences as migrants themselves as well as in their professional roles as clinicians who serve immigrant and refugee populations.
State of the Border — Policies that happened under the Trump administration and now under the Biden administration have left people vulnerable to injustices in Mexico and other Central American nations. People are fleeing persecution, gang violence, and other violence such as sexual or other violent assaults and now they must also face the additional burden of the lack of access to basic necessities like food, water and shelter. A lot of compounding trauma occurs at the border that has potential downstream mental health implications for individuals and their families.
Culturally Competent and Trauma-Informed Care — Interpersonal components such as screening for trauma exposure and providing resources to families are an important aspect of trauma-informed care, and it should also include efforts at the organization level to create sanctuary or immigrant-friendly spaces and implement immigration-informed care, which builds on the concept of trauma-informed care by honing in on the unique factors associated with immigrant populations, e.g. protocols for broaching sensitive topics like immigration status and policies to ensure people are safe from immigration enforcement.
ICE and Policing — Instances of immigration enforcement in healthcare settings are rare, and when they do happen they can look like patients being interrogated at the bedside or even being arrested as they step out of the hospital just after visiting someone. These instances contribute to immense fear that can act as a deterrent from seeking care or engaging with any other helping professional institutions in the future–this goes for the individual(s) directly impacted and the people within their communities.
Impact of Health Records — The impact of health records within the context of healthcare for immigrant populations is complex because migration status really should not be documented explicitly as it can open people up to harms such as stigma from providers or being turned over to law enforcement agencies who may cooperate with immigration enforcement. Many organizations, such as the American Medical Association Journal of Ethics, recommend against documenting immigration status in medical records.
Application of teachings — It is advised to amplify the work that is already being done in communities and identify what areas at the systems level need to change as well as the key stakeholders.
Pearls
Dr. Hayat discusses the five major waves of migration in the last fifty years, resulting from the Soviet-Afghan War, the Afghan Civil War, the Fall of the Taliban, August 2021 US and western forces departure, and how he grew up during the 1990s right after the collapse of the government. He recounts street fights in Kabul as well as an overall theme of people going back to a focus on survival, or the need for food, shelter, water and safety.
Dr. Saadi discusses how her parents left Iraq under Saddam Hussein’s dictatorship, where he was targeting many Iraqis with Iranian ancestry and Shi’a Muslims–which included members of her family. She notes she was born in Iran and her family emigrated to Canada and then to the United States just a month before 9/11. She recounts this time as particularly tumultuous for not only Muslim Americans but also South Asian Americans, Sikh Americans, as well as Arab Americans who were not Muslims.
Dr. Saadi highlights that the majority of immigrants do not come through the US-Mexico border, even for undocumented folks. Additionally, in the case of folks who are undocumented, it is likely the case that they attained this status as a result of overstaying their previously valid visa.
Dr. Saadi discusses the Biden administration rule proposal that would essentially prohibit refugees from seeking asylum in the US, making them ineligible for asylee status.
Dr. Saadi highlights that there needs to be a greater focus on the continuum of experiences when we discuss patients who are immigrants or forcibly displaced because there is not often a clear pre-post distinction. Many people’s journeys can involve being in an encampment, being detained in immigration prisons, or stopping in multiple countries before reaching the final destination.
Dr. Saadi also uplifts the fact that while we focus primarily on those we have clinical encounters with, it is always important to mention that there are many people that did not make it to clinic for an amalgam of reasons — many people lost their lives in the quest for better lives and freedom from persecution.
Dr. Hayat stresses the difference that cultural psychiatry, cultural competency, and the biopsychosocial model make in building rapport and there is a lot that goes on in between pre- and post-resettlement and those experiences have to be taken into account, especially in cases where there are language and cultural barriers. He highlighted the DSM-5 Cultural Formulation Interviews.
Dr. Saadi recommends avoiding documentation of immigration status in medical records, or having clear guidelines on what to do if immigration enforcement is present at the clinical setting.
Dr. Saadi notes that we must not see people as the sum of their traumas, they are so much more than that — especially in the case of forcibly displaced peoples and immigrants. We must not reduce people to their trauma exposure alone.
Dr. Hayat interestingly mentions that some organizations have been able to build relationships with law enforcement, educate them, and share different challenges to help realize a common goal.
Dr. Hayat notes that while organizations recommend against documenting immigration status in medical records, needs can still be met through partnerships with community organizations. Dr. Saadi adds that we can collect this data, and there is immense groundwork that must be done to develop protections for immigrant and refugee populations and ensure the data are protected.
Dr. Saadi mentioned a toolkit around policies and actions that can be implemented at an organizational level that is publicly available at www.doctorsforimmigrants.com. She also mentions additional organizational-level policies and actions that can take place beyond what is mentioned in the toolkit such as setting up a medical legal partnership where people can connect to attorneys that can help them with their immigration case or civic engagement promotion. She also mentioned Dr. Mark Kuczewski’s sanctuary doctrine toolkit that focuses more on the individual level. Refer to Good Sanctuary Doctoring for Undocumented Patients for more information. Dr. Hayat mentioned his colleague, Dr. Olivia Shadid, who does work on mental health evaluations for asylum seekers, which can be found here.
References
Morris JE, Saadi A. The Biden administration’s unfulfilled promise of humane border policies. Lancet. 2022 May 28;399(10340):2013. doi: 10.1016/S0140-6736(22)00741-3. Erratum in: Lancet. 2022 Jun 2;: PMID: 35644152.
Shi M, Stey A, Tatebe LC. Recognizing and Breaking the Cycle of Trauma and Violence Among Resettled Refugees. Curr Trauma Rep. 2021;7(4):83-91. doi: 10.1007/s40719-021-00217-x. Epub 2021 Nov 13. PMID: 34804764; PMCID: PMC8590436.
Valtis Y, Okah E, Davila C, Krishnamurthy S, Essien UR, Calac A, Fields NF, Lopez-Carmen VA, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 16: Live from SGIM: Best of Antiracism Research at the Society of General Internal Medicine’s 2022 Annual Meeting” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. May 3, 2022
Berkman JM, Rosenthal JA, Saadi A. Carotid Physiology and Neck Restraints in Law Enforcement: Why Neurologists Need to Make Their Voices Heard. JAMA Neurol. 2021;78(3):267–268. doi:10.1001/jamaneurol.2020.4669
James J, Heard-Garris N, Krishnamurthy S, Cooper A, Calac A, Watkins A, Onuoha C, Lopez-Carmen VA, Krishnamurthy S, Calac A, Nolen L, Williams J, Tsai J, Ogunwole M, Khazanchi R, Fields NF, Gillette-Pierce K. “Episode 18: Remedying Health Inequities Driven by the Carceral System” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. October 18, 2022.
Chiesa V, Chiarenza A, Mosca D, Rechel B. Health records for migrants and refugees: A systematic review. Health Policy. 2019 Sep;123(9):888-900. doi: 10.1016/j.healthpol.2019.07.018. Epub 2019 Jul 30. PMID: 31439455.
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Saadi A, Hayat N, Krishnamurthy S, Cooper, A, Nolen L, Gillette-Pierce K, Calac A, Essien UR, Fields NF, Lopez-Carmen VA, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 21: Antiracist Healthcare for Immigrant and Refugee Populations ” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. April 25, 2023
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Dr. Ravi Singh presents a case of right arm weakness to Yazmin and Sridhara.
Yazmin is a Mexican Graduate from the Universidad Autonoma de Yucatan. During her medical training, she developed a strong interest in Public Health, Medical Education, and Health Equity and is looking forward to pursuing a career in Internal Medicine. When she is not volunteering on a project, she likes taking care of her plants, developing her skills in the fine arts, or learning a new language.
Sridhara is a board-certified internist, neurologist, vascular neurologist, and hypertension specialist. Currently, he holds the position of Clinical Assistant Professor at Thomas Jefferson University Hospital and serves as the Director of Neurology for Jefferson New Jersey.
As a medical professional, he is passionate about case-based learning, clinical reasoning, and teaching decision-making while avoiding the pitfalls of heuristics. His goal is to bridge the ever-growing gap between neurology and internal medicine, an area in which he has a keen interest.
Ravi (Ravitej) Singh is originally from Greenwich, London U.K where he grew up playing soccer and rugby. He attended medical school at University of Debrecen, Hungary and completed residency at Medstar Harbor Hospital in Baltimore. Currently he is an associate program director for Sinai Hospital IM residency program in Baltimore as well as a Hospitalist on the teaching service. He is a faculty member at the Johns Hopkins School of Medicine and takes time out of his schedule to run a series of case-based teaching sessions as well as medical simulation with all of the medical students that rotate at Sinai throughout the year. He is also a co-chair of the ACP Maryland IMG committee where he advocates for IMG issues Jo and highlights their contributions to the healthcare system
Episode 20 – Medical Racism and Indigenous Peoples
Show Notes by Sudarshan (“Sud”) Krishnamurthy
April 4, 2023
Summary: This episode highlights the checkered past of medicine and the advancements in the field that have occurred at the expense of the humanity of Indigenous peoples. During this episode, we hear from Dr. Nav Persaud, a staff physician in the Department of Family and Community Medicine at St. Michael’s Hospital in Unity Health Toronto, and Dr. Alika Lafontaine, the current President of the Canadian Medical Association. Together, our guests explain how Indigenous knowledge systems are the foundation of modern medicine and also share strategies to promote truth and reconciliation with Indigenous Peoples in North America. This discussion is hosted by Alec Calac and Gillette Pierce.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Explain how the dark legacy of discrimination and deliberate oppression of Indigenous Peoples has led to present-day disparities across the world
Describe how medicine has held some white men to high esteem, even when they harbored significant racist and sexist notions
Identify the role of Indigenous knowledge systems in shaping much of modern medicine today, yet experiencing erasure from the mainstream
Credits
Written and produced by: Alec J. Calac, Gillette Pierce, Sudarshan Krishnamurthy, Rohan Khazanchi, MD, MPH, Dereck Paul, MD, Jazzmin Williams, Victor A. Lopez-Carmen MPH, Ashley Cooper, Naomi F. Fields, LaShyra Nolen, Jennifer Tsai MD, MEd, Chioma Onuoha, Ayana Watkins, Michelle Ogunwole MD, Utibe R. Essien MD, MPH
Hosts: Alec J. Calac and Gillette Pierce
Infographic: Creative Edge Design
Audio Edits: Caroline Cao
Show Notes: Sudarshan (“Sud”) Krishnamurthy
Guests: Dr. Nav Persaud and Dr. Alika Lafontaine
Time Stamps
0:00 Introduction
0:45 Episode Introduction
1:10 Guest Introductions
3:30 Existing global disparities among Indigenous Peoples
6:00 How access to medications are impacted among Indigenous Peoples in Canada
8:30 Framing around the Design of Structures in Canada to suppress Indigenous voices
13:30 Legacy of Osler and the importance of rediscovering forgotten dark histories
16:20 Dehumanization of individuals belonging to marginalized groups by the healthcare system
27:50 Modern medicine and its roots in Indigenous knowledge systems
31:30 Provision of healthcare to Indigenous Peoples in Canada
34:50 Alec’s own advocacy around renaming a campus parking garage
36:55 Weaponization of professionalism
45:00 Clinical takeaways and practical tools for clinician listeners
Episode Takeaways
Indigenous communities around the world experience significant disparities in life expectancy, burden of disease, and socioeconomic status, due to deliberate exclusion of Indigenous Peoples from the mainstream and suppression of their voices in the design of the system.
Within medicine, we tend to hold white men from history books in high esteem, often without recognizing the dark legacy that accompanied their lives. William Osler is one such example who, along with numerous other sexist and racist misconducts, took remains of Indigenous people with him as a gift to his mentor in Germany, that is still held by a German museum who refuses to return it.
The dehumanization of individuals of color at the margins of society by the healthcare system is not simply a thing of the past, and is certainly a persistent phenomenon. Cindy Gladue, Brian Sinclair, and Joyce Echaquan are three Indigenous individuals who suffered immense harm at the hands of the healthcare system.
There is strength in reconciling Indigenous history, and we must prevent further erasure of Indigenous knowledge systems. The solutions to these issues do not fall upon one community’s shoulders, but instead on the shoulders of all of us along with the oppressive systems that have led us here.
Pearls
Alec begins by contextualizing this episode with the fact that although Indigenous people make up 6% of the global population, they compose 15% of the global population experiencing extreme poverty. Additionally, Indigenous communities experience lower life expectancy, higher burden of disease, and lower socioeconomic status compared to non-Indigenous Peoples. These disparities are likely attributable, in part, to the disruption of Indigenous knowledge systems, inadequate infrastructure, and poor identification of health data among these groups, rather than individual behavior. [Supplementary Resource for Listeners: CPSolvers Episode 12: Addressing Anti-Indigenous Racism in Medicine with team members Alec Calac and Victor Anthony Lopez-Carmen]
Nav discusses that despite publicly funded healthcare systems in Canada and federal protections in place for certain Indigenous groups, Indigenous populations and other groups facing discrimination and historic oppression are much more likely to report not being able to take medications due to cost. Although healthcare services are publicly funded, access to medications depends on private or public insurance and is linked with employment. While some have the impression that there is a safety net in Canada for life-saving medications, Nav still sees patients in his practice who are harmed by the system and not able to afford life-saving medications, many of them Indigenous, and this is a violation of their right to access essential medicines.
Alika expands on Nav’s framing by highlighting the three broad demographics in Canada: the Inuit, the Métis, and the First Nations. In contrast to settlers in the United States where “conquering” through deception was a priority, the spread of settlers was more so through the signing of agreements that were never lived up to. Indigenous peoples in Canada have deliberately been left out of the mainstream to ensure their voices were suppressed in the design of the system.
Alika elaborates on the history of Indigenous populations in Canada and how they would conduct X-Rays on the Inuit children, and ship these kids away for 3 to 10 years if they found tuberculosis in the lungs, without even allowing the children to say goodbye to their parents. Alika recalls stories of individuals in Ottawa who were on the same floor for several years, only to realize that they were members of the same family after being placed in these TB sanatoriums and crossing paths there.
Nav begins to discuss how Osler is still revered as one of the most prominent historical physicians in Canada and the United States. A colleague brought information to Nav that Osler had brought remains of Indigenous people as a gift to one of his mentors in Germany. This led him to look into Osler’s history a little further, and Nav found it easy to find other instances of racist and sexist misconduct by William Osler. These remains are still in a museum in Germany, with no plan of return to Indigenous communities. [Supplementary Resource for Listeners: Read Dr. Persaud’s initial article on Osler here]
Osler lived in the time of Numbered Treaties and the North-West Rebellion under Louis Riel, when Indigenous rights were front and center. It is ridiculous to consider that a physician brought Indigenous remains with him as a gift during this period in history, when Osler knew Indigenous people were fighting for their rights and lives. So, we must rethink the esteem that we hold white men like Osler in, and rediscover the forgotten history that accompanies them. [Supplementary Resource for Listeners: You can read more about the North-West Rebellion here]
Alika discusses the dehumanization of individuals of color and other identities who exist at the margins within the healthcare system and emphasizes that these are not phenomena of the past. He highlights the hostility within the healthcare system and how healthcare must be a service that is available equally to everybody, and not treated as a favor being done to individuals. He narrates the stories of Cindy Gladue, Brian Sinclair, and Joyce Echaquan, all of whom suffered immense harm at the hands of the healthcare system as Indigenous individuals. [Supplementary Resource for Listeners: You can read about Cindy Gladue, Brian Sinclair, and Joyce Echaquan here]
Nav expands on this aspect of dehumanization of Indigenous peoples and speaks about how the Indigenous remains are being treated in Germany today. Although there is guidance that they must be returned, they have decided to retain them. In addition, there is writing within these skulls with numbers written on the inside, as if to catalog them. The museum has also added multiple barriers for those who wish to rightfully receive these remains, and has placed the onus on these communities for these remains to be returned.
Alec importantly highlights that while these harms might seem historical and like things of the past, they have taken place within one or two generations and even today. He discusses his experiences as an Indigenous person in California who attends a medical school that begrudgingly decided to return Indigenous remains, from one of the largest collections in the world.
Alika talks about strength in knowing his history. He discusses the medical knowledge of settlers in Canada believing in four humors and the practice of bloodletting to relieve sickness. At that time, Indigenous Peoples were harvesting plants at their peak potency and concentrating these plants in teas, and delivering medications through oral and transdermal routes. He talks about how Atropine, a commonly used drug by anesthesiologists like Alika, is derived from Belladonna and how folks practicing traditional medicine use Belladonna.
Alika also delves deeper into the provision of healthcare to Indigenous peoples in Canada. He mentions that healthcare was provided to Indigenous peoples rooted in a charitable effort, rather than as a basic human right. It is important to move beyond being nice to each other, and begin to think about the requirements and obligations we have to each other as human beings.
Alec goes on to highlight that as much as we have gained, we have much more to fight for. In episode 12, we discussed how the American Indian and Alaskan Native life expectancy as of 2021 was equivalent to that of the American public in the 1940s. The solution to these issues shouldn’t fall upon one or a few of our shoulders, but instead upon the shoulders of all of us along with the systems that have the resources and infrastructures to inform change.
Alec used Nav’s article to advocate for the renaming of a parking garage on campus that was named after William Osler. Our spaces reflect our values, so the question he asked was why they had a parking garage named after an individual who has no relation to the local community in San Diego? We think about the legacy in medicine, but forget about the community we are in. [Supplementary Resource for Listeners: Read Alec’s Editorial about his advocacy related to renaming a street and parking structure in his medical school campus here.]
Nav describes professionalism as a vague concept that is often used to oppress individuals from racialized and marginalized backgrounds. Professionalism is often antithetical to a rights-based approach to medicine, where every member of a team feels comfortable to speak up when everything is not right with a patient’s care and professionalism can scare people from speaking out when needed.
Alika expands on this explanation of professionalism in terms of what is acceptable, decided by whoever is in control. It can be used to amplify what leaders think is important and suppress what leaders do not like, demonstrating the importance of leadership from diverse backgrounds and varied lived experiences. Retaliation can be severe to violations of professionalism, and it’s hard to know the effects of retaliation unless one has experienced these themselves. [Supplementary Resource for Listeners: Read about the experience Dr. Lafontaine describes regarding his own experience with reporting unprofessional and unacceptable conduct here]
Nav states that it is important for us to reflect on what has happened and recollect all of the work people have done to chronicle anti-Indigenous racism. Racism is not new, and there have been numerous reports that document racism and anti-Indigenous discrimination over decades and centuries. We must respect what has happened, and recognize as non-Indigenous people that we benefit from advocacy and efforts of Indigenous peoples for Indigenous rights over generations.
Alika emphasizes that the point of this conversation is not to make anyone feel like they are a bad person, but instead to help them acknowledge that in this healthcare system we provide both health and harm. Providing our patients with more space and ensuring our patients feel human again is a great first step. It is also important to remember that in the course of restructuring power, there are winners and losers and we may not all have the same voice around the table that we did before. We entered medicine to help people, and sometimes the best way to help people is by getting out of the way and allowing for others to step forward.
References
Persaud N, Butts H, Berger P. William Osler: saint in a “White man’s dominion”. CMAJ. 2020;192(45):E1414-E1416. doi:10.1503/cmaj.201567
Reid P, Cormack D, Paine SJ. Colonial histories, racism and health-The experience of Māori and Indigenous peoples. Public Health. 2019;172:119-124. doi:10.1016/j.puhe.2019.03.027
Redvers N, Blondin B. Traditional Indigenous medicine in North America: A scoping review. PLoS One. 2020;15(8):e0237531. Published 2020 Aug 13. doi:10.1371/journal.pone.0237531
Fredericks CF. Mapping the Sustainable Development Goals onto Indian Nations. In: Miller RJ, Jorgensen M, Stewart D, eds. Creating Private Sector Economies in Native America: Sustainable Development through Entrepreneurship. Cambridge: Cambridge University Press; 2019:185-194. doi:10.1017/9781108646208.011
Browne AJ, Lavoie JG, McCallum MJL, Canoe CB. Addressing anti-Indigenous racism in Canadian health systems: multi-tiered approaches are required. Can J Public Health. 2022;113(2):222-226. doi:10.17269/s41997-021-00598-1
Persaud N, Ally M, Woods H, et al. Racialised people in clinical guideline panels. Lancet. 2022;399(10320):139-140. doi:10.1016/S0140-6736(21)02759-8
Lafontaine AT, Lafontaine CJ. A retrospective on reconciliation by design. Healthc Manage Forum. 2019;32(1):15-19. doi:10.1177/0840470418794702
Lafontaine A. Indigenous health disparities: a challenge and an opportunity. Can J Surg. 2018;61(5):300-301. doi:10.1503/cjs.013917
Durand-Moreau Q, Lafontaine J, Ward J. Work and health challenges of Indigenous people in Canada. Lancet Glob Health. 2022;10(8):e1189-e1197. doi:10.1016/S2214-109X(22)00203-0
Okpalauwaekwe U, Ballantyne C, Tunison S, Ramsden VR. Enhancing health and wellness by, for and with Indigenous youth in Canada: a scoping review. BMC Public Health. 2022;22(1):1630. Published 2022 Aug 29. doi:10.1186/s12889-022-14047-2
Berger P. Canadian Physicians’ Breach of Duty to Patients and Communities from the Acquisition of Indigenous Skulls in the 19th Century to the Abandonment of People with AIDS in the 20th Century. J Biocommun. 2021;45(1):E13. Published 2021 Aug 15. doi:10.5210/jbc.v45i1.10849
The hosts and guests report no relevant financial disclosures.
Citation
Persaud N, Lafontaine A, Calac A, Pierce G, Krishnamurthy S, Essien UR, Fields NF, Lopez-Carmen VA, Cooper A, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 20: Advancing Medicine at the Expense of Indigenous Humanity” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. April 4, 2023
Episode 281: The Consult Question #8 – Pancytopenia and Rash
Mar 23, 2023
https://clinicalproblemsolving.com/wp-content/uploads/2023/03/3.23.23-TCQ-RTP.mp3Dr. Vipul Kumar presents a fascinating case of pancytopenia and rash to guest discussant, Dr. Anand Patel. Dr. Vipul Kumar MD PhD is a hematology-oncology fellow at UCSF. He is currently in his second year of fellowship and has a clinical interest in oncology of all forms as well as a passion for teaching. Dr. Anand Patel is an assistant professor of medicine at University of Chicago where he treats patients with leukemia and myeloid malignancies. He also serves as medical director of the inpatient leukemia service. His research focuses on the development of clinical trials to help improve the standard of care for patients with high risk leukemias and myeloid malignancies. Twitter: @Anand_88_Patel
Simone and Moses review their approach to chronic lower extremity weakness in a patient with new-onset jaundice, as Vale presents them a case with a neuro flavor to it.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Yazmin presents a case of lethargy and myoclonus to Kiara and Maria.
María Jimena Alemán was born and raised in Guatemala where she currently works in community and rural health care. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Ella Fitzgerald. Outside of medicine, she enjoys modern art, 21st century literature, and having hour-long conversations over a nice hot cup of coffee or tequila.
Kiara Camacho-Caballero was born in Lima, Perú and she is a medical doctor at Universidad Científica del Sur. She is passionate about Internal Medicine, Cardiology, and medical education. Her research interests are cardiology, neurology, and, geriatrics. Her plans are to apply for Internal Medicine residency in the US this year. Outside medicine, she is a past triathlete and her dream is to perform an IRONMAN 70.3 someday. Kiara enjoys running, and spending time with her dog named Zack and her favorite food is turkey legs.
Yazmin Heredia
@minheredia
Yazmin is a Mexican Graduate from the Universidad Autonoma de Yucatan. During her medical training, she developed a strong interest in Public Health, Medical Education, and Health Equity and is looking forward to pursuing a career in Internal Medicine. When she is not volunteering on a project, she likes taking care of her plants, developing her skills in the fine arts, or learning a new language.
Episode 275: Anti-Racism in Medicine Series – Episode 19 – Reframing the Opioid Epidemic: Anti-Racist Praxis, Racial Health Inequities, and Harm Reduction
Feb 09, 2023
Episode 19 – Reframing the Opioid Epidemic: Anti-Racist Praxis, Racial Health Inequities, and Harm Reduction
Show Notes by Alec Calac
February 9, 2022
Summary: This episode highlights racialized disparities in addiction treatment. During this episode, we hear from Dr. Jessica Isom, a board-certified community psychiatrist and faculty leader in the Yale Department of Psychiatry’s Social Justice and Health Equity Curriculum, and Dr. Ayana Jordan, the endowed Barbara Wilson Associate Professor in the Department of Psychiatry, Addiction Psychiatrist and Associate Professor in the Department of Population Health at New York University (NYU) Grossman School of Medicine. Together, our guests explore and unpack how the criminalization and racialization of substance use builds to the present-day opioid epidemic and shapes inequities in care. There is a special emphasis on the use of public health models that prioritize harm reduction and person-centered care to prevent drug-related fatalities and curb the opioid epidemic along lines of race and class. This discussion is hosted by Ashley Cooper, Sudarshan Krishnamurthy, and new team member Gillette Pierce.
Episode Learning Objectives:
After listening to this episode, learners will be able to…
Explain how the criminalization and racialization of substance use builds to the present-day opioid epidemic and shapes inequities in care.
Describe how the media shapes public sentiment toward substance use and addiction treatment.
Identify realistic solutions to drug policy reform that promote health equity among marginalized communities living in the United States.
Credits:
Written and produced by: Ashley Cooper, MPhil; Sudarshan Krishnamurthy; Gillette Pierce; Alec J. Calac; Michelle Ogunwole, MD, PhD; Ayana Watkins; Chioma Onuoha; Naomi F. Fields, MD; Victor A. Lopez-Carmen, MPH; Rohan Khazanchi, MPH; Sudarshan Krishnamurthy; Utibe R. Essien, MD, MPH; Jazzmin Williams; LaShyra Nolen; Jennifer Tsai MD, MEd
Hosts: Ashley Cooper, Sudarshan Krishnamurthy, and Gillette Pierce
Infographic: Creative Edge Design
Audio Edits: Caroline Cao and Ashley Cooper, MPhil
Show Notes: Alec Calac
Guests: Jessica Isom, MD, MPH and Ayana Jordan, MD, PhD
Time Stamps:
1:30 Guest Introductions
4:15 Framing the Sociohistorical Context of the Opioid Epidemic
10:47 Racialization of Substance Use and Medicalization of the Human Experience
14:28 Changing “Faces of Addiction” and Impact on U.S. Drug Policy
16:35 United States, Chinese Laborers, and Anti-Chinese Sentiment (“Opium Fiends”)
19:30 “Moral Panic”
23:00 Separating Minoritized Individuals from the Majority
23:40 Cocaine Possession Sentencing Disparities
26:50 Shifting Social Attitudes Toward Substance Use and Addiction
30:30 (Mis)framing of Substance Use as a White Problem to Enact Change
33:15 Rectifying Racial Health Inequities in Opioid Addiction Treatment
36:10 Take-Home Methadone and a Less Clear Need for Methadone Clinics
40:40 Understanding Substance Use Disparities with Racially Disaggregated Data
47:00 Pushing Back Against “One Size Fits Most”
49:30 Harm Reduction Practices
53:00 Narrowing the Empathy Gap and Connecting with Patients
55:25 Spirit of Sankofa: Looking Back to Move Forward
59:15 Reducing Harm and “Optimizing Safety”
1:08:00 Community-Centered Solutions
1:10:20 Drug Policy Reform
1:15:42 Episode Takeaways
Episode Takeaways:
Health care providers, especially physicians, cannot be equity-ignorant or egalitarian in our racialized society. They can use their training and privilege to advocate for meaningful policy reform.
The opioid epidemic is more than a white problem. Demographic data in research and practice must always be disaggregated by race and ethnicity.
Screening for substance use and offering connections to treatment and community-based services are important strategies that clinicians can implement in their own practice today.
Pearls:
In 2020, American Indian and Alaska Native (Indigenous) communities experienced the highest drug overdose mortality rate of any racial or ethnic group, also surpassing rates among the non-Hispanic white population. Between 2007 – 2019, Black individuals experienced a higher death rate for opioid overdose deaths than any other racial or ethnic group. [Supplementary Resource for Listeners: CPSolvers Episode 12: Addressing Anti-Indigenous Racism in Medicine with team members Alec Calac and Victor Anthony Lopez-Carmen]
Dr. Jordan begins our episode by framing the racialization and criminalization of substance use in the larger history of the United States, emphasizing that American society has seen substance use as “criminal behavior” or a moral failing, rather than as a medical condition, which began towards the early 2000s. She mentions that academia, as well as the media, have contributed to this complex social phenomenon by tying together race, gender, and substance use, especially in the context of maternal health and neonatal abstinence syndrome. The foundational literature in this area has furthered stigma and bias, especially towards Black birthing persons. These narratives have vilified individuals who would benefit from comprehensive, person-centered substance use treatment, rather than incarceration and other adverse harms.
Dr. Isom continues the conversation around the intentionality of these structural processes and the language that frames the racialization of substance use in the United States by lawmakers, media, and the healthcare profession. This parallels another process, which is the medicalization of human experiences, especially those relating to childbirth and pregnancy. A more Western perspective on health care emphasizes the role of physicians and health care providers and marginalizes the role and contributions of doulas and midwives. She then ties this back to Dr. Jordan’s conversation about the criminalization of substance use and how resources and infrastructure are dedicated to incarceration, rather than psychotherapy and related treatments. [Supplementary Resource for Listeners: Advancing Health Equity: A Guide to Language, Narrative and Concepts]
Sudarshan goes further into the changing “faces of addiction” and asks our guests to describe its impact on drug policy in the United States. Dr. Isom first challenges our listeners to engage with anti-racist praxis and challenge dominant racial narratives about substance use, policing, and other encounters. She then goes into how the racialization of substance use drove positive public sentiment for the adoption of punitive outcomes for substance use. One example that is presented involves the complicated relationship between the United States and Chinese immigrants and farmworkers in California. Once the need for labor was largely met, anti-Chinese narratives (e.g., opium fiends) emerged around opium, gambling, and prostitution, which fits into this pattern or formula of associating specific racial and ethnic groups with substance use as a rhetorical threat to the “most valued demographic” in the United States (white women and children) to drive the adoption of punitive measures. This largely obscures the reality that substance use rates are similar among different racial and ethnic groups. [Supplementary Resource for Listeners: San Francisco Opium Ordinance described in Race and the Criminalization of Drugs – National Press Foundation | NPF featuring Dr. Jessica Isom and Dr. Helena Hansen]
Dr. Jordan echoes these thoughts and posits that divergence from the “ideal” American identity (i.e., white, cisgender, heterosexual) makes it possible to other (verb) individuals and enact policies and laws that punish individuals with marginalized identities. She shared that rhetoric used by Nixon and the subsequent war on drugs has similarities to Trumpism and messaging associated with Make America Great Again (MAGA). This is then reaffirmed during the Reagan Administration and is later codified into sentencing structures, in which we see vastly different amounts of cocaine possession (100:1 crack versus powder cocaine possession offenses) amounting to similar sentences, with crack cocaine use most prevalent among minoritized individuals and powder cocaine use most prevalent among the white majority. Involvement with the carceral system further intersects with issues around employment, household income, and other related disparities. To our listeners, how might we begin redressing these harms and reinvest in minority communities adversely affected by the war on drugs? [Supplementary Resource for Listeners: Cracks in the System: 20 Years of the Unjust Federal Crack Cocaine Law | American Civil Liberties Union]
The conversation then shifts into changing social attitudes toward substance use and addiction. Dr. Isom breaks down media messaging and the varying tones and contexts used to describe substance use disparities and how that contributes to social stigma. She explains how different types of stigma intersect with media messaging to craft narratives that encourage sympathy or even a lack of sympathy towards certain racial and ethnic groups and health behaviors. Dr. Isom then discusses that policy reform and changing attitudes toward substance use and addiction are largely driven by the hurt and pain of those in the white majority with substance use disorder, further minimizing the experiences of marginalized communities.
Dr. Jordan agrees with this characterization and goes more into the historical media coverage of substance use and the dehumanizing language that was (and is still) used to describe drug use among minority individuals. This segues into a conversation about the legacy of the war on drugs and today’s racial inequities in opioid addiction treatment. Ashley delineates that methadone has been disproportionately prescribed in predominantly Black communities, as a means to drive down crime, whereas white patients undergoing substance use treatment are more likely to receive buprenorphine. Dr. Jordan highlights the harm that these prescribing practices cause as they falsely associate race and substance use with criminal activity and neighborhood safety. She further goes into the stigma and stereotyping that continues to this day with the incessant and inhumane need to pick up prescription treatment once daily, submit “clean” urine samples under direct supervision, and submit to oral examinations. Dr. Jordan then questions the utility and continued operation of methadone clinics, especially as the United States largely moves on from the COVID-19 pandemic. She highlights actions taken by the United States Substance Abuse and Mental Health Services Administration (SAMHSA) to expand access to take-home methadone doses, which promoted patient autonomy and had comparable adherences outcomes and no significant changes in potential adverse harms, such as overdose and diversion. Other actions include elimination of the United States Drug Enforcement Administration (DEA) X waiver which was needed to prescribe buprenorphine. Dr. Jordan concludes by thinking about incentive strategies that would encourage health care providers to change their prescribing practices and minimize racial inequities in opioid addiction treatment [Supplementary Resource for Listeners: Lessons from COVID 19: Are we finally ready to make opioid treatment accessible? – PMC]
Dr. Isom highlights the differences in substance use disparities and infrastructure utilization from the national level moving into discrete communities. Using an equity lens, she shares her own experiences in Massachusetts examining treatment utilization and encourages health care providers to examine racially disaggregated data to make sure that services offering suboxone (buprenorphine and naloxone) are reaching and being used in the most impacted communities. She also discusses the importance of the patient-provider relationship and shared-decision making, which helps ensure that a full range of services are being offered to patients. Dr. Jordan and Dr. Isom both agree that simply offering treatment services and having an “open door” are not enough. Dr. Jordan discusses the importance of de-centering the majority and identifying the factors that are most relevant to minoritized individuals and communities. Oftentimes, researchers and practitioners working to implement addiction treatment programs and interventions are not from those same communities. Dr. Jordan pushes back on the notion that “one size fits most” is the optimal approach for treating substance use disorder and that the evidence we rely on for patients undergoing substance use treatment was largely informed by the experiences of white individuals. Therefore, traditional settings of addiction care may unintentionally cause harm to individuals with marginalized identities.
Gillette moves the conversation into strategies addressing substance use disparities, particularly those that emphasize the importance of harm reduction. Dr. Isom begins by sharing her experiences in the clinic and how harm reduction approaches such as offering fentanyl test strips humanize substance use treatment and place individual and community health and well-being at the center of treatment. To her dismay, she also learned that her racially and linguistically diverse patient population was one of most affected by the opioid epidemic in the Commonwealth of Massachusetts. Reflecting on these health data and rethinking “traditional” addiction treatment strategies helped her connect with her patients and close a self-described empathy gap that she says patients accessing treatment often have with their health care provider. Dr. Jordan enters into the conversation and also shares how she best connects with her patients who often feel unheard and marginalized by the health care system. She discusses the strengths and limitations of harm reduction approaches and the continued need for a clinician-researcher workforce that reflects the diversity seen in communities experiencing hardship. An important part of her discussion includes the contributions of community health workers and a need not just to focus on harm reduction, but also to optimize safety among individuals using substances such as alcohol and opioids. This complementary approach has the potential to increase the positive impact that the harm reduction movement has made over time.
The group briefly discusses Dr. Isom’s article Nothing About Us Without Us in Policy Creation and Implementation | Psychiatric Services (2021) which highlights the need for patients and communities to be included in the creation and implementation of drug policy. This approach has the potential to best direct resources to the most impacted communities and may be more impactful than traditional community engagement models. Dr. Jordan has also written about culturally-responsive programs benefiting Black communities affected by the opioid epidemic and has completed a pilot study providing addiction treatment in partnership with faith-based organizations. Both guests acknowledge that academics do not always have the right solutions and that practitioners have to listen openly to community knowledge holders.
Towards the end of the episode, Dr. Jordan highlights opportunities for meaningful drug policy reform, including examining federal methadone regulations (e.g., dosing, availability), investing in harm reduction and safety optimization, and decreasing police involvement in mental health crisis response and police presence in substance use treatment settings.
New Host! Kiersten TâLeigh (Ta-Lee) “Gillette” Gillette-Pierce (she/they) is currently a student at Johns Hopkins School of Public Health pursuing a Master of Science in Public Health with a double concentration in Maternal, Fetal, and Perinatal Health and Women, Sexual and Reproductive Health. As an academic researcher, they focus on transnational racial/ethnic and gender disparities in pregnancy-related, sexual, and reproductive health outcomes for all persons with gynecologic organs, with a specific interest in people of African descent. She is published in the Journal of Advanced Nursing and Medicine, Science, and Law. Gillette has also published work with Rewire News Group and the Center for American Progress focusing on sexual and reproductive health and rights policy, reproductive justice, and health outcomes for Black birthing persons. With almost ten years of experience in the global sexual and reproductive health, rights, and justice field, Gillette aims to improve sexual and reproductive health care and outcomes for disenfranchised communities and significantly improve pregnancy-related outcomes for people of African descent.
Speaker Biographies
Dr. Jessica Isom, MD, MPH, is a board-certified community psychiatrist and faculty leader in the Yale Department of Psychiatry’s Social Justice and Health Equity Curriculum. She primarily works in Boston as an attending psychiatrist at Codman Square Health Center where she is leading a grant effort to infuse antiracism in Opioid Use Disorder (OUD) services. She is a nationally recognized expert on racial equity and justice in psychiatry with a focus on workforce development and organizational transformation. Her professional interests include working toward eradicating racial and ethnic mental health disparities, mitigating the impact of implicit racial bias on clinical care, and the use of a community-centered population health approach in psychiatric practice. She serves on multiple advisory boards and is a consultant, curriculum developer and presenter to a variety of organizations including Fortune 500 companies and medical societies through her company, Vision for Equity LLC. Dr. Isom received her MD from the University of North Carolina School of Medicine, and completed her residency at Yale University.
Ayana Jordan, MD, PhD, is the Barbara Wilson Associate Professor in the Department of Psychiatry, Addiction Psychiatrist and Associate Professor in the Department of Population Health at New York University (NYU) Grossman School of Medicine. She also serves as Pillar Co-Lead for Community Engagement at NYU Langone’s Institute for Excellence in Health Equity. As Principal Investigator for the Jordan Wellness Collaborative (JWC), she leads a research, education, and clinical program that partners with community members to provide optimal access to evidence-based treatments for racial and ethnic minoritized patients with mental health disorders. Through her multifaceted work, she provides addiction treatment in faith settings, studies health outcomes for people with opioid use disorder in the carceral system, and trains addiction specialists to provide culturally-informed treatment. Dr. Jordan is dedicated to creating spaces and opportunities for more people of color, specifically Black women in academia who are vastly underrepresented. She has numerous peer-reviewed publications, has been featured at international conferences, and is the proud recipient of various clinical and research awards. The fundamental message of equity and inclusion has informed her research, clinical work, and leadership duties at NYU and beyond.
References
Ahmad FB, Cisewski JA, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. 2022. Designed by LM Rossen, A Lipphardt, FB Ahmad, JM Keralis, and Y Chong: National Center for Health Statistics.
Balasuriya, L., Isom, J., Cyrus, K., Ali, H., Sloan, A., Arnaout, B., Steinfeld, M., DeSouza, F., Jordan, A., Encandela, J., & Rohrbaugh, R. (2021). The Time Is Now: Teaching Psychiatry Residents to Understand and Respond to Oppression through the Development of the Human Experience Track. Academic Psychiatry, 45(1), 78–83. https://doi.org/10.1007/s40596-021-01399-x
Castillo, E. G., Isom, J., DeBonis, K. L., Jordan, A., Braslow, J. T., & Rohrbaugh, R. (2020). Reconsidering Systems-Based Practice: Advancing Structural Competency, Health Equity, and Social Responsibility in Graduate Medical Education. Academic Medicine, 95(12), 1817–1822. https://doi.org/10.1097/ACM.0000000000003559
DeSouza, F., Mathis, M., Lastra, N., & Isom, J. (2021). Navigating Race in the Psychotherapeutic Encounter: A Call for Supervision. Academic Psychiatry, 45(1), 132–133. https://doi.org/10.1007/s40596-020-01328-4
Friedman, J. R., & Hansen, H. (2022). Evaluation of Increases in Drug Overdose Mortality Rates in the US by Race and Ethnicity Before and During the COVID-19 Pandemic. JAMA Psychiatry, 79(4), 379. https://doi.org/10.1001/jamapsychiatry.2022.0004
Godkhindi P, Nussey L, O’Shea T. “They’re causing more harm than good”: a qualitative study exploring racism in harm reduction through the experiences of racialized people who use drugs. Harm Reduct J. 2022 Aug 25;19(1):96. doi: 10.1186/s12954-022-00672-y. PMID: 36008816; PMCID: PMC9406271.
Goldman, M. L., Swartz, M. S., Norquist, G. S., Horvitz-Lennon, M., Balasuriya, L., Jorgensen, S., Greiner, M., Brinkley, A., Hayes, H., Isom, J., Dixon, L. B., & Druss, B. G. (2022). Building Bridges Between Evidence and Policy in Mental Health Services Research: Introducing the Policy Review Article Type. Psychiatric Services, 73(10), 1165–1168. https://doi.org/10.1176/appi.ps.202100428
Hansen H, Jordan A, Plough A, Alegria M, Cunningham C, Ostrovsky A. Lessons for the Opioid Crisis-Integrating Social Determinants of Health Into Clinical Care. Am J Public Health. 2022 Apr;112(S2):S109-S111. doi: 10.2105/AJPH.2021.306651. PMID: 35349328; PMCID: PMC8965192.
Hughes M, Suhail-Sindhu S, Namirembe S, Jordan A, Medlock M, Tookes HE, Turner J, Gonzalez-Zuniga P. The Crucial Role of Black, Latinx, and Indigenous Leadership in Harm Reduction and Addiction Treatment. Am J Public Health. 2022 Apr;112(S2):S136-S139. doi: 10.2105/AJPH.2022.306807. PMID: 35349317; PMCID: PMC8965189.
Isom, J., & Balasuriya, L. (2021). Nothing About Us Without Us in Policy Creation and Implementation. Psychiatric Services, 72(2), 121–121. https://doi.org/10.1176/appi.ps.72202
Isom, J., Jordan, A., Goodsmith, N., Medlock, M. M., DeSouza, F., Shadravan, S. M., Halbert, E., Hairston, D., Castillo, E., & Rohrbaugh, R. (2021). Equity in Progress: Development of Health Equity Curricula in Three Psychiatry Residency Programs. Academic Psychiatry, 45(1), 54–60. https://doi.org/10.1007/s40596-020-01390-y
James K, Jordan A. The Opioid Crisis in Black Communities. J Law Med Ethics. 2018 Jun;46(2):404-421. doi: 10.1177/1073110518782949. PMID: 30146996.
Jordan, A., Mathis, M. L., & Isom, J. (2020). Achieving Mental Health Equity: Addictions. Psychiatric Clinics of North America, 43(3), 487–500. https://doi.org/10.1016/j.psc.2020.05.007
Jordan A, Babuscio T, Nich C, Carroll KM. A feasibility study providing substance use treatment in the Black church. J Subst Abuse Treat. 2021 May;124:108218. doi: 10.1016/j.jsat.2020.108218. Epub 2020 Dec 3. PMID: 33771290.
Lagisetty, P. A., Ross, R., Bohnert, A., Clay, M., & Maust, D. T. (2019). Buprenorphine Treatment Divide by Race/Ethnicity and Payment. JAMA Psychiatry, 76(9), 979. https://doi.org/10.1001/jamapsychiatry.2019.0876
Nweke, N., Isom, J., & Fashaw-Walters, S. (2022). Health Equity Tourism: Reckoning with Medical Mistrust. Journal of Medical Systems, 46(5), 27. https://doi.org/10.1007/s10916-022-01812-4
Portnoy, G. A., Doran, J. M., Isom, J. E., Wilkins, K. M., DeViva, J. C., & Stacy, M. A. (2021). An evidence-based path forward for diversity training in medicine. The Lancet Psychiatry, 8(3), 181–182. https://doi.org/10.1016/S2215-0366(21)00024-9
Roxas, N., Ahuja, C., Isom, J., Wilkinson, S. T., & Capurso, N. (2021). A Potential Case of Acute Ketamine Withdrawal: Clinical Implications for the Treatment of Refractory Depression. American Journal of Psychiatry, 178(7), 588–591. https://doi.org/10.1176/appi.ajp.2020.20101480
Townsend, T., Kline, D., Rivera-Aguirre, A., Bunting, A. M., Mauro, P. M., Marshall, B. D. L., Martins, S. S., & Cerdá, M. (2022). Racial/Ethnic and Geographic Trends in Combined Stimulant/Opioid Overdoses, 2007–2019. American Journal of Epidemiology, 191(4), 599–612. https://doi.org/10.1093/aje/kwab290
Wyatt JP, Suen LW, Coe WH, Adams ZM, Gandhi M, Batchelor HM, Castellanos S, Joshi N, Satterwhite S, Pérez-Rodríguez R, Rodríguez-Guerra E, Albizu-Garcia CE, Knight KR, Jordan A. Federal and State Regulatory Changes to Methadone Take-Home Doses: Impact of Sociostructural Factors. Am J Public Health. 2022 Apr;112(S2):S143-S146. doi: 10.2105/AJPH.2022.306806. PMID: 35349318; PMCID: PMC8965186.
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Isom J, Jordan A, Cooper A, Krishnamurthy S, Pierce G, Calac A, Watkins A, Onuoha C, Lopez-Carmen VA, Nolen L, Williams J, Tsai J, Ogunwole M, Khazanchi R, Fields NF. “Episode 19: Reframing the Opioid Epidemic: Anti-Racist Praxis, Racial Health Inequities, and Harm Reduction”. The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. February 9, 2022.
Sukriti and Maani present a clinical unknown to Dr. Reza, followed by a brief discussion about addressing roadblocks that women in medicine face.
Dr. Nosheen Reza
Dr. Nosheen Reza is a cardiologist and translational researcher at the University of Pennsylvania focusing on advanced heart failure and transplant cardiology and cardiovascular genetics. She obtained her medical degree from the University of Virginia School of Medicine and completed internal medicine residency at the Massachusetts General Hospital. She then completed both her Cardiovascular Disease and Advanced Heart Failure and Transplant Cardiology fellowships at the University of Pennsylvania. At Penn, Dr. Reza pursued additional scholarship in genomic medicine as an NIH T32-funded postdoctoral fellow and in healthcare quality as a Penn Benjamin & Mary Siddons Measey Fellow in Quality Improvement and Patient Safety. Now, as an Assistant Professor of Medicine, she cares for patients in the Penn Center for Inherited Cardiovascular Disease and in the Section of Heart Failure, Transplantation, and Mechanical Support. Dr. Reza is also an Assistant Program Director of the Cardiovascular Disease Fellowship and the Director of the Penn Women in Cardiology program.
The spaced learning series team tackles the case of a patient with a non-resolving pulmonary inflammatory syndrome, found to have a cavitary lesion on lung imaging with glomerulonephritis.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time,Valeria presents a case of headache and altered mental status to Joy and Mattia.
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue Neurology residency. Her interests include neuro-infectious diseases, transgender health and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine she loves running, hiking, cooking pasta and spending time with her dogs.
Joy Glanton
@joytibalan
Joy is a neuro enthusiast who has completed her neuroscience undergrad and medical studies in the Philippines. She is passionate about neurology and believes “the brain is everything; it’s what makes us who we are.” She is hoping to match into Neurology in 2023, and is currently in NYC completing clinical externships/rotations in neurology. Post residency, she aspires to do translational/clinical research work or pursue a career in academic/general neurology. Joy enjoys running, swimming, literary art, debates in neuroscience, and listening to rock and roll and classical music.
Mattia Rosso
@MattiaRosso3
Mattia Rosso is a neurology resident at the Medical University of South Carolina (MUSC) in Charleston, South Carolina. He is interested in movement disorders, behavioral neurology, and autoimmune neurology. He is also passionate about the intersection between the humanities and medicine. He started a Neurohumanities group at MUSC, which meets monthly and features internal and guest speakers. This group focuses on the role of the Arts, Cinema, Literature, Philosophy, and Music in medicine and neurosciences. Outside work, he enjoys photography, cinema, and discovering new music. Since starting residency, the Clinical Problem Solvers have been an irreplaceable source of learning and inspiration.
Episode 268: WDx #21 – Clinical Unknown with Dr. Rachael Lee
Dec 14, 2022
Dr. Lee joined the UAB Division of Infectious Diseases at UAB in 2016 and is currently an Associate Professor. She is the UAB Chief Healthcare Epidemiologist and in this role, she utilizes evidence based medicine to prevent the spread of healthcare-associated infections. Her research focuses on multi-drug resistant pathogens as they relate to infection prevention and control.
Reza and Rabih discuss a fascinating case of AMS, infection and polyuria.
rlrCPSOLVERS.COM
RLR have transitioned from Patreon to have their website rlrCPSolvers.com. Check out this virtual classroom full of bonus schemas, illness scripts, teaching videos and case challenges
Get a personalized clinical reasoning curriculum to take your skills to the next level AND support the CPSolvers while you are at it.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, John presents a case of diplopia to Valeria and Madellena.
John Acquaviva is a fourth-year medical student attending Lake Erie College of Osteopathic Medicine in Erie, Pennsylvania. He has a passion for both clinical and academic neurology and will be starting neurology residency in the summer of 2023. He has special interests in neurophysiology, autoimmune neurology, and neuroimmunology, but is excited about all neurological fields. In his free time, he enjoys hanging out with friends, long-boarding, running, and martial arts.
Valeria Roldán
@valeroldan23
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue Neurology residency. Her interests include neuro-infectious diseases, transgender health and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine she loves running, hiking, cooking pasta and spending time with her dogs.
Madellena Conte
@MadellenaC
Madellena Conte was born and raised in San Francisco, CA. She completed her undergraduate degree at Dartmouth College. After college, she worked at Collective Health, a healthcare insurance technology company, and then completed her Master’s of Science in Global Health at UCSF where her research focused on understanding preferences for HIV care among people experiencing unstable housing. She is a MS4 at the Zucker School of Medicine at Hofstra/Northwell in New York and is currently taking a research year in the Division of HIV, ID, and Global Medicine at UCSF. Outside of medicine, Madellena loves to travel, meet new people, run, figure skate and really do anything outdoors. She plans on applying into internal medicine residency.
Episode 18 – Remedying Health Inequities Driven by the Carceral System
Show Notes by Ayana Watkins
October 18, 2022
Summary: This episode highlights the history and roots of the carceral system, as well as its far-reaching impacts on the health of women and children today. During this episode, we gain insight from special guests Dr. Jennifer James—a qualitative researcher, a Black Feminist scholar, and an assistant professor in the Institute for Health and Aging, the Department of Social and Behavioral Sciences, and the Bioethics program at the University of California San Francisco—and Dr. Nia Heard-Garris—a pediatrician and researcher in the Department of Pediatrics at Feinberg School of Medicine at Northwestern University and in the Division of Academic General Pediatrics and Mary Ann & J. Milburn Smith Child Health Research, Outreach, and Advocacy Center at the Ann & Robert H. Lurie Children’s Hospital of Chicago. This discussion is hosted by Sudarshan Krishnamurthy, Ashley Cooper, and Alec J. Calac.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Understand the history of mass incarceration and its effect on health
Recognize how cultures of punishment and control within carceral spaces and within clinical settings impact health
Learn how to best care for and support those experiencing violence at the hands of the carceral system
Consider how we enact carceral structures and act as agents of the state in our clinical practices
Credits
Written and produced by: Sudarshan Krishnamurthy, Ashley Cooper, Alec J. Calac, Michelle Ogunwole MD, PhD, Ayana Watkins, Chioma Onuoha, Naomi F. Fields MD, Victor A. Lopez-Carmen MPH, Rohan Khazanchi MPH, Sudarshan Krishnamurthy, Utibe R. Essien MD, MPH, Jazzmin Williams, LaShyra Nolen, Jennifer Tsai MD, MEd, Zahada (Kiersten) Gillette -Pierce
Hosts: Sudarshan Krishnamurthy, Ashley Cooper, and Alec J. Calac
Infographic: Creative Edge Design
Audio Edits: Isabella Gau
Show Notes: Ayana Watkins
Guests: Dr. Nia Heard-Garris, MD, MSc and Dr. Jennifer James, PhD, MS, MSW
Time Stamps 00:00 Introduction of episode and guests 04:01 History of mass incarceration and its relationship with health 11:38 Understanding healthcare decision-making in carceral spaces 22:27 Substance Use and Treatment/Diversion vs. Incarceration of BIPOC mothers 29:30 Health Impacts on Children and Young Adults with History of Parental Incarceration 35:24 Remedying Health of Women and Children Impacted by the Criminal Legal System 45:55 Key takeaways
Episode Takeaways:
Prisons are not places of healing. Incarceration negatively affects the physical and mental health of people who are incarcerated as well as their family members and loved ones, and limits access to healthcare before, during, and after incarceration.
All healthcare professionals will have patients who are directly or indirectly impacted by the carceral system. Our guests remind us to think critically about our role in the carceral system and in imposing systems of control and punishment within clinical settings. Additionally, our guests urge us to recognize the ways in which our patients are impacted by incarceration and to ask our patients about these impacts in order to better care for them.
The ways to remedy the negative impacts of incarceration are to incarcerate fewer people and to invest in communities. Providing communities with the resources they need to survive, such as educational opportunities, jobs, and quality healthcare, will eliminate the need for incarceration. Additionally, decarceration and abolition will remedy the far-reaching health effects of the criminal legal system.
Pearls
“Prisons and jails are not healing spaces [. . .] They are not spaces designed for healing or care, they are designed for punishment and control.”
Dr. James explains that the culture of punishment, control, and violence within jails and prisons impedes healthcare for people who are incarcerated. People who are incarcerated are dehumanized and feel they are treated as inmates, rather than as patients. Correctional officers act as gatekeepers, deciding who does and does not need medical care. This means that people who are incarcerated are often not believed when they say they need medical care. As a result of this dehumanization and mistreatment, people who are incarcerated may forgo seeking medical care because they do not trust that the system and healthcare professionals will do anything but harm them further.
Dr. Heard-Garris draws parallels between the culture within the carceral system and that within hospitals and clinics. For clinicians who do not work within jails or prisons, it is important to recognize the presence of these same issues within other clinical spaces. Hospitals and clinics also have security, armed guards, and police whose roles are to impose control, and their presence can impact health outcomes for patients.
Dr. Heard-Garris also added that having a family member in the carceral system makes it more likely that a person will lose confidence in the medical system and will not seek care, so this mistrust in healthcare reverberates in generations post-incarceration.
Substance Use and Society’s focus on incarceration and punishment over treatment, diversion, and healing for BIPOC women
Dr. Heard-Garris explained that systems such as capitalism, politics, and white supremacy are the reasons our society focuses on incarceration and punishment rather than on substance use treatment. She discusses how it’s easier to incarcerate people than it is to invest in treatment because investment requires time, money, and the dismantling of our current systems.
Dr. James adds that reproductive justice and the rights to family, and having the resources and support to raise children have never existed for people of color and people experiencing poverty. Current-day familial structures reflect policies dating back to slavery, the forced displacement of Native Americans, and the way immigrant families have been treated. Today, the carceral system plays a pivotal role in modern-day eugenics and in reproductive and family control.
Health Impacts on Children and Young Adults with History of Parental Incarceration & Juvenile Justice Involvement
Dr. Heard-Garris explains that the health impacts that affect people who are incarcerated also impact children and adolescents with parents who have been incarcerated. This exposure to the carceral system negatively impacts the physical and mental health of these children and young adults and reduces their access to healthcare.
She also reminds us that children with parents who are incarcerated are not doomed to poor outcomes. Many of these children and young adults are resilient and are still able to thrive. However, they should not have to undergo these adverse childhood experiences and traumas. The carceral system needs to be changed and these children need to be supported and have their healthcare and education needs met.
Remedying the Health of Women and Children Impacted by the Criminal Legal System
Both Dr. James and Dr. Heard-Garris agree that the best way to remedy the health impacts of the carceral system is to incarcerate fewer people.
Dr. James discusses changes that can be made if we assume the current carceral system will remain. We need a system, such as a single-payer healthcare system, that provides people with consistent access to high-quality care before, during, and after incarceration. Additionally, we should provide people who are incarcerated with better ways to communicate with their families. For healthcare specifically, it is important to believe people when they say they need care and provide them with access to trauma-informed care.
Dr. Heard-Garris adds that a good place to start is to decarcerate people and offer them support. Additionally, we need to prevent incarceration by investing in communities and providing communities with resources, education, jobs, healthcare, etc. The goal is to create a society in which prisons and jails aren’t necessary because every person has what they need to survive.
Practices Clinicians can Incorporate to Reduce the Impacts of Mass Incarceration on Patients
Dr. James reminds us that no matter where we work or what specialty we work in, we will see people who are impacted by incarceration. As physicians and healthcare professionals, we should ask people about their histories of trauma and about the impact of incarceration on their lives. Additionally, we need to be cognizant of the ways we as providers enact a carceral state and think critically about the way these systems impact patient care.
Dr. Heard-Garris encourages us to ask patients about their interactions with the carceral system. Asking these questions provides us with an opportunity to better care for our patients. It can allow us to offer more support systems to patients and to connect patients with resources that have worked for others. We also have to be aware of our power and privilege and recognize that we do not treat all our patients equitably in order to change and do better.
References
Black Feminist Bioethics: Centering Community to Ask Better Questions. Hastings Cent Rep. 2022 03; 52 Suppl 1:S21-S23. James JE. PMID: 35470879.
Race, Racism, and Bioethics: Are We Stuck? Am J Bioeth. 2022 03; 22(3):22-24. James JE. PMID: 35258424.
Heard-Garris N, Sacotte KA, Winkelman TNA, Cohen A, Ekwueme PO, Barnert E, Carnethon M, Davis MM. Association of Childhood History of Parental Incarceration and Juvenile Justice Involvement With Mental Health in Early Adulthood. JAMA Netw Open. 2019 Sep 4;2(9):e1910465. doi: 10.1001/jamanetworkopen.2019.10465. PMID: 31483468.
Heard-Garris N, Winkelman TNA, Choi H, Miller AK, Kan K, Shlafer R, Davis MM. Health Care Use and Health Behaviors Among Young Adults With History of Parental Incarceration. Pediatrics. 2018 Sep;142(3):e20174314. doi: 10.1542/peds.2017-4314. Epub 2018 Jul 9. Pediatrics. 2019 May;143(5): PMID: 29987170.
Heard-Garris N, Johnson TJ, Hardeman R. The Harmful Effects of Policing—From the Neighborhood to the Hospital. JAMA Pediatr. 2022;176(1):23–25. doi:10.1001/jamapediatrics.2021.2936
Heard-Garris, N., Boyd, R., Kan, K., Perez-Cardona, L., Heard, N. J., & Johnson, T. J. (2021). Structuring poverty: how racism shapes child poverty and child and adolescent health. Academic pediatrics, 21(8), S108-S116.
Kaba, Mariame, et al. No More Police: A Case for Abolition. The New Press, 2022.
Roberts, Dorothy. Torn Apart: How the Child Welfare System Destroys Black Families–and How Abolition Can Build a Safer World. Basic Books, 2022.
Wilkerson, Isabel. Caste (Oprah’s Book Club): The origins of our discontents. Random House, 2020.
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
James J, Heard-Garris N, Krishnamurthy S, Cooper A, Calac A, Watkins A, Onuoha C, Lopez-Carmen VA, Krishnamurthy S, Calac A, Nolen L, Williams J, Tsai J, Ogunwole M, Khazanchi R, Fields NF, Gillette-Pierce K. “Episode 18: Remedying Health Inequities Driven by the Carceral System” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. October 18, 2022.
In this WDx episode, Sharmin and Dr Lekshmi Santhosh delve into the world of written evaluations: why are they important, implicit biases they can contain and how to do a better job in both writing and interpreting evaluations.
Dr. Lekshmi Santhosh
Dr. Lekshmi Santhosh is an associate professor of medicine at UCSF. She specializes in adult pulmonary and critical care medicine with a focus on medical education. She attends in the Medical ICU, the Neuro ICU, on the Internal Medicine teaching wards, and has clinic at the Pulmonary Outpatient Faculty Practice at UCSF-Parnassus. She is the founder and Medical Director of the multidisciplinary long-COVID/post-ICU OPTIMAL Clinic at UCSF Health.
She serves as the Associate Program Director for Curriculum for the Internal Medicine Residency and the Associate Program Director of the Pulmonary and Critical Care Medicine Fellowship. She also is the Director of the Department of Medicine Grand Rounds. She obtained her Master’s in Health Professions Education from UC-Berkeley. Her primary interests in medical education research are related to ICU transitions of care, women in leadership, clinical reasoning, and subspecialty career choice.
This episode is dedicated to the loving memory of Gabriel Talledo, we reflect on how greatly he touched our lives followed by his story, as told by him in the first episode of Queer Rounds.
Please consider donating here to the Gabriel Talledo’s Scholarship benefiting young medical students of the LGTBQIA community in hopes of financially helping them achieve their dreams.
Episode 258: Spaced Learning Series – Pulmonary Granulomas, Headache, and Hyponatremia
Sep 28, 2022
The SLS team tackles the case of a young woman presenting with a prolonged, inflammatory pulmonary syndrome is found to have pulmonary granulomas, headaches and hyponatremia. Join them as they apply CPSolvers schemas to real life Patient care to facilitate the diagnostic reasoning process.
Sharmin, Ann Marie, and Dan discuss a case that takes us on a journey through the pancreas and hepatobiliary systems with schemas at every stop of the way!
We cannot wait to share the new RLR website with you as our time on Patreon is coming to an end. The website is our dream project. You will be notified once the website is up before anyone else. We are a few weeks away!!!
And remember to reach out to us if there are any issues regarding refunds from Patreon as you cancel your annual subscriptions. It is very important to us that each of you are 100% satisfied with RR.
We hope you will continue to follow us and support our work once the new website is up and running. None of this is possible without you. We are so grateful for your support. For now, keep your monthly $5 Patreon subscription active b/c we are uploading audio as usual until the new website is up and running.
We will be offering so much more on the website. We think you will love it.
Enjoy this episode. We hope you don’t get a headache listening to it!!!
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, CPSolvers team member Rafael Medina presents a case of frequent falls for CPSolvers team member Yazmin and Alice.
Rafael Medina dos Santos is a Brazilian medical graduate. Before medicine, Rafael wanted to be a teacher. Unsurprisingly, he loves everything related to teaching and learning, so his passion for the CPSolvers’ mission was only natural. He’s applying this 2023 match season for internal medicine. Beyond medicine, Rafael loves fiction books/movies, pop music, and singing Disney songs.
Yazmin Heredia Allegretti
@minheredia
Yazmin is a Medical Graduate from Mexico, looking forward to applying to an Internal Medicine Residency in the U.S. She is passionate about medical education, health equity, and clinical reasoning and believes knowledge (as well as healthcare) must be accessible to everyone. She looks forward to collaborating with doctors and students worldwide to create the best evidence-based resources to impulse medical practice and patient care. Aside from medicine, you will find her taking care of her wide collection of plants, developing her skills in the fine arts, volunteering for any project she can find, or learning new languages.
Alice Falck
Alice is a 5th-year medical student from Berlin, currently working on her MD doctoral thesis to contribute to the pathophysiology of temporal lobe epilepsy. She aspires to be a neurologist and is interested in neuroscience, electrophysiology, and of course clinical reasoning. She is passionate about gender equality in general and especially in Medicine. In her free time, she loves discussing movies with friends and eating great food.
Dr. Rezigh presents a case of fever in a patient newly diagnosed with HIV to Dr. Woc-Colburn.
Dr. Alec Rezigh
Alec Rezigh is an academic hospitalist at Baylor College of Medicine in Houston, TX. He completed medical school at McGovern Medical School in Houston and his residency at The University of Colorado. His clinical interests include medical education and clinical reasoning. He loves all things basketball, CPSolvers, and playing with his human and doggy daughters.
Dr. Laila Woc-Colburn
Dr. Laila Woc-Colburn is an associate professor in the Division of Infectious Diseases at Emory University School of Medicine in Atlanta. She is a renowned medical educator and has a wide range of clinical interests including tropical medicine, HIV, and fungal diseases.
In this episode, Dr. Ashley McMullen, Dr. Simone Vais, and Jane Lock share stories of setbacks in medicine related to the theme, “I thought I was alone.” Session moderated by Madellena Conte.
Dr. Ashley McMullen is an assistant professor of medicine at the University of California, San Francisco, and a primary care internist based at the San Francisco VA Hospital. She is also a Houston, TX native and lifelong book nerd, who grew up nurtured by her mother, a pediatric nurse, and grandmother, an ordained minister. Dr. McMullen’s work focuses on the role of narrative and storytelling in medical education, and as a mechanism for healing, advocacy, and improving care across differences. She served as the host and producer of The Nocturnists: Black Voices in Healthcare Series, a 2021 Webby Award Honoree, and recently launched a new story-telling podcast with Dr. Kimberly Manning called, The Human Doctor.
Jane Lock
Jane Lock is an MD/PhD candidate at Boston University School of Medicine, currently in her M4 year applying into internal medicine. She was born in Malaysia and grew up in Taiwan before moving to the US for college and medical school. She has a strong interest in oncology research, particularly in mechanisms of DNA damage and repair in cancer. Her PhD thesis was focused on understanding alternative telomere maintenance mechanisms in osteosarcoma. She is also passionate about teaching and improving medical education. Outside of work and studying, she loves being the cool aunt to her 2 year old nephew, reading, crocheting and watching The Office with her husband.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Valeria Roldan presents a case of tremors and myoclonus to Dr. Aaron Berkowitz.
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue Neurology residency. Her interests include neuro-infectious diseases, transgender health and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine she loves running, hiking, cooking pasta and spending time with her dogs.
Dr. Aaron Berkowitz
@AaronLBerkowitz
Aaron recently joined the founding faculty of Kaiser Permanente Bernard J. Tyson School of Medicine as a professor of neurology and director of global health. He previously served as an associate professor of neurology at Brigham and Women’s Hospital and Harvard Medical School, where he directed the Mind-Brain-Behavior course for first-year students and was a teaching attending on the neuro-hospitalist service and in the general neurology resident clinic. As a health and policy advisor to Partners In Health and senior specialist consultant to Doctors Without Borders, he has worked tirelessly to bring neurology care and education to regions where it is limited or non-existent, including co-developing the first neurology residency in Haiti. He is the author of Clinical Pathophysiology Made Ridiculously Simple, Clinical Neurology and Neuroanatomy: A localization-based approach, and most recently One by One by One, which tells the complex, moving, and inspiring stories of patients he and colleagues brought from Haiti to Boston for neurosurgery for brain tumors. When he is not trying to #EndNeurophobia, Aaron loves hiking, backpacking, and obsessively researching outdoor camping gear.
Pratik presents a case of dyspnea and RUQ pain to Fred.
Dr. Fred McLafferty
Fred McLafferty, MD is a fellow in the Division of Pulmonary and Critical Care at the University of California, San Francisco. His research interest is in how certain environmental particles and pathogens drive lung remodeling and pulmonary fibrosis. He is clinically interested in advanced lung disease and transplant, and will begin as the advanced fellow in lung transplant at UCSF in July 2022. Prior to fellowship, he graduated medical school from the David Geffen School of Medicine at UCLA and then completed both his internal medicine residency and chief residency at Northwestern University. Outside the hospital he enjoys skiing in Tahoe, riding his bike through San Francisco, or spending all day cooking a (sometimes) delicious dinner.
Dr. Pratik Doshi
Pratik Doshi, MD MS is a second-year Internal Medicine Resident at the University of Southern California. He completed medical school at Duke University School of Medicine. He is interested in delivering medical content in innovative ways and aspires to be a cardiologist. He is active on Twitter, follow him @PratikDoshiMD!
Dr. Jenn Davis presents a consult question to Dan, Doug, Emma, Sukriti, and Dr. Laila Woc-Colburn.
Dr. Laila Woc-Colburn
Dr. Laila Woc-Colburn is an associate professor in the Division of Infectious Diseases at Emory University School of Medicine in Atlanta. She is a renowned medical educator and has a wide range of clinical interests including tropical medicine, HIV, and fungal diseases.
Dr. Jennifer Davis
Dr. Jennifer Davis is a first year infectious diseases fellow at the Mass General Brigham combined infectious diseases fellowship in Boston. She’s interested in HIV and medical education.
Vale, Brodie, and Gabriel discuss basic terminology of the LGBTQ+ community, the importance of communication in healthcare, and pieces of advice when using gender-inclusive language.
Vale, Brodie, and Gabriel talk about their journey as LGBTQ+ members and the genesis of Queer Rounds, a platform that highlights the reality of gender and sexual diverse communities in healthcare.
Patreon exclusive: RLR 97_2 Cases (Anasarca, Hemoptysis) with Kirtan!!
Jun 22, 2022
Dear Patrons,
You don’t want to miss this episode. Two cases in one hour.
CPSolvers’ team member and extraordinary diagnostician, Kirtan, presents two fascinating cases to RR that have a similar theme.
We highly recommend you follow Kirtan on Twitter to enhance your diagnostic skills @KirtanPatolia.
Kirtan: We wish you the best as you start your IM residency. We are incredibly proud of what you have accomplished but are even more excited about what you are going to accomplish.
In this episode, Maani and Sharmin are joined by Dr. Tara Gadde who presents a clinical unknown case to Dr. Aimee Zaas followed by a discussion on leadership, mentorship, and career transition points.
Uttara (Tara) Gadde
Uttara (Tara) Gadde is an internal medicine resident at the University of Pennsylvania. She went to Cornell University for undergrad and completed a B.S. in Human Biology, Health & Society. She then worked for a year as a research analyst and public health advocate on a CDC funded HIV testing grant in the Bronx. She decided to pursue medicine and went to medical school at Rutgers NJMS and is completing her MPH from Johns Hopkins. Her career interests include infectious disease and global health. During her free time, she loves to cook (and eat!), curl up with a good book, or do anything active (running, hiking, HIIT workouts, yelling at the TV during Nets games).
Aimee K Zaas
Aimee K Zaas MD MHS is a Professor of Medicine in the Division of Infectious Diseases in the Department of Medicine at Duke University School of Medicine. She has served as the Program Director for the Duke Internal Medicine Residency since 2009, a job she considers to be both the best job ever and a continuous welcome challenge! She completed her medical school at the Northwestern Feinberg School of Medicine and her internal medicine residency and chief residency (ACS) at The Johns Hopkins Hospital. After completing her Infectious Diseases fellowship at Duke University, she joined the faculty at Duke where she has remained ever since, and has become a rather obnoxious Duke basketball fan in the process. Her husband David is also a physician and they have two boys, Jake (18) and Jonah (16) so have spent the majority of their family life at kids sporting events and traveling related to kids sporting events.
Summary: This episode centers the roles of reproductive justice and anti-racist action in rectifying inequities faced by Black and Indigenous birthing persons. This discussion is hosted by Naomi Fields, MD, Chioma Onuoha, and Victor Lopez-Carmen MPH, as they interview Dr. Joia Crear-Perry—a physician, policy expert, and highly sought-after birth equity and racial health disparities expert—and Dr. Katy B. Kozhimannil—the Distinguished McKnight University Professor in the Division of Health Policy and Management at the University of Minnesota and Director of the Rural Health Research Center. Our inspiring guests highlight liberation-oriented solutions to addressing inequities and contextualize how we can facilitate birthing experiences grounded in reproductive justice for Black & Indigenous women.
Episode Learning Objectives
After listening to this episode, learners will be able to…
Understand the magnitude of disparities faced by Black and Indigenous birthing persons and how forces of structural racism created and perpetuate these inequities
Define Reproductive Justice and understand how clinicians can promote reproductive justice during pregnancy and birth
Appreciate the importance of cultural reflexivity, community-centered initiatives, and midwifery and doula care in facilitating reproductive justice
Recognize the impacts of climate and land injustices on Black and Indigenous communities and know that climate justice, reproductive justice, and racial justice are all connected
Credits
Written and produced by: Naomi F. Fields MD, Chioma Onuoha, Victor A. Lopez-Carmen MPH, Rohan Khazanchi MPH, Sudarshan Krishnamurthy, Utibe R. Essien MD, MPH, Jazzmin Williams, Alec J. Calac, LaShyra Nolen, Michelle Ogunwole MD, PhD, Jennifer Tsai MD, MEd, Ayana Watkins
Hosts: Naomi F. Fields MD, Chioma Onuoha, and Victor A. Lopez-Carmen MPH
Infographic: Creative Edge Design
Audio Edits: David Hu, MD
Show Notes: Ayana Watkins
Guests: Dr. Joia Crear-Perry and Dr. Katy B. Kozhimannil
Time Stamps
00:00 Introduction
03:57 Magnitude of maternal health disparities for Black & Indigenous birthing people
09:31 Impact of guests’ identities and lived experiences on their work
25: 30 Defining reprodutive justice
29:42 Importance of community-centered initiatives and access to midwifery and doula care
35:15 Impact of Climate and Land Injustice on maternal health inequities
42:43 Role of family planning within reproductive justice
58:00 Key takeaways
Episode Takeaways:
We have a responsibility to unlearn the harmful hierarchies that unequally value people. The institutions of science, medicine, and academia perpetuate and codify racism. We all must recognize the codification of racism within our institutions and work to unlearn these hierarchies in order to better care for Black and Indigenous patients.
Be present in the birthing moment and see the full humanity of the birthing person and the life-changing nature of birth. Dr. Kozhimannil reminds us that birth is transformative and a gift to witness. As healthcare providers, we must listen to our patients and use the power of our presence to see birthing people’s full humanity and empowerment.
Pearls
Black and Indigenous birthing people are 3-13 times more likely to die in childbirth, with the rate varying by location and level of investment in communities.
Dr. Crear-Perry describes the magnitude of maternal health disparities faced by Black and Indigenous birthing people. The exact statistics vary by location and by the overall level of investment in services such as childcare and parental leave within each community. For example, in New York City, Black birthing persons are 8-12 times more likely to die in childbirth, while in other areas, such as in areas in the Deep South where Dr. Crear-Perry is from, the increased likelihood of death in childbirth for Black birthing persons is lower, around 2-3x.
Dr. Kozhimannil reminds us to look past the statistics and zoom into the personal level. She urges us to recognize that maternal mortality changes the life trajectories of individuals and communities. These statistics not only reflect the number of birthing people dying in childbirth but also evince the number of children growing up without a parent and the number of families losing a loved one. She also reminds us that while mortality is the worst possible outcome, it is not the only thing we should be concerned about; that we must also ask the question: What are we doing to ensure that birth is as beautiful and empowering as possible?
“I have worked to imbue the credibility of my lived knowledge into the credibility that I now receive as a fancy person with a Ph.D. and a professor.”
Dr. Kozhimannil describes that her identity and her background—growing up in a rural area, having family living on tribal lands, and the intergenerational impact maternal mortality has had on her family and on her people—inform and motivate her work. She recognizes that academia and medicine traditionally do not listen to the people closest to the harm of structural racism and thus aims to use the credibility and privilege she receives from academia as a “Distinguished Professor” to persuade people with power to change the way they allocate power, resources, and opportunities.
Both Dr. Crear-Perry and Dr. Kozhimannil describe experiencing rejection when submitting their work to journals because of academia’s resistance to acknowledging racism as a cause of disparities.
Defining Reproductive Justice
Dr. Crear-Perry explains that the term “reproductive justice” was coined in 1994 by 12 Black women and is defined as the fundamental human right to personal bodily autonomy, to have children, to not have children, and to have safe and sustainable communities in which to parent children.
Reproductive justice first requires birthing people to be viewed as fully human. As Dr. Crear-Perry notes, Black women and other marginalized people in the United States have never been viewed as fully human. The second tenet of reproductive justice is the right to have children, and the third is the right to not have children. Certain policies have impeded birthing people’s ability to choose to not have children by taking away rights if people do not bear children. For example, at one time in Louisiana, only childbearing adults qualified for Medicaid. This policy reflects a societal belief that humans are not valuable unless they provide a service. Dr. Crear-Perry discusses a policy proposed in Michigan grounded in a similar notion: it required people living in urban areas to have a job in order to qualify for Medicaid. (To expand, this provision in Michigan was initially included in a State Senate bill for Medicaid expansion, but the work requirement was scrapped before the policy passed.) The final tenet of reproductive justice is the right to parent children in a safe, sustainable community. Parents deserve to raise their children in communities that value human life. For example, safe and sustainable communities have access to paid leave and equal pay, parks, and walkways, and lack dangerous aspects, like police violence and mass incarceration.
Impact of climate and land injustices on maternal health equity
Dr. Crear-Perry discusses previous research detailing the impact of climate injustice on maternal health transnationally. For example, Black babies born in communities that experienced redlining were more likely to die, and heat is known to cause premature birth. Additionally, scientists have used climate change to promote population control and to codify eugenics by falsely blaming climate change on high birth rates within poor, Indigenous communities around the world rather than uber-consumptive corporations.
Dr. Kozhimannil asserts that “climate justice and reproductive justice and racial justice are completely the same thing.” The climate crisis indicates a tear in the connection between humans and the earth and between us and one another. Dr. Kozhimannil believes the most powerful way to reconnect humans to each other and to the earth is through a good birth, in which we are connected to the land and are surrounded by loved ones.
Dr. Kozhimannil also describes an Indigenous philosophy of honoring the seven generations of ancestors that came before you and striving to be a good ancestor for the seven generations that will come after you. The process of childbirth is transformative for the birthing person and their community. Clinicians are able to shape the environment in which people give birth by caring for the earth and their patients.
The extent to which “family planning” fits within reproductive justice
Dr. Crear-Perry outlines the history of the term “family planning” and states that the idea of family planning stems from population control and eugenics. She urges us to remember that the abiltity to plan anything, is determined by generational access to power; and calls for discontinuing the use of this term. We should instead prioritize reproductive and sexual well-being and seeing Black and Indigenous birthing people as fully human.
Dr. Kozhimannil discusses her work on rural maternity care and the lack of hospital-based obstetric services. The places with the least access to hospitals in which they can give birth are also the places where people have experienced forced sterilization, where people do not have access to choices surrounding contraception, sexuality, or termination of pregnancies. Dr. Kozhimannil asks what moms and families can do if they do not have access to pregnancy prevention or termination and yet also have no place to give birth.
Asking the right questions, having the right intentions
Dr. Kozhimannil shares an important story about how her groundbreaking work showing maternity deserts in rural areas only came about by centering and engaging community members. In research we always begin with the research question and perhaps wonder if we are asking the “right” question. Dr. Kozhimannil offers a different approach, and stresses the importance of “answering the right question, from the people [communities impacted], who know the right question.”
Dr. Crear-Perry offers additional wisdom about interventions: “If your intention is off, your outcome is going to be off.”
Clarification: In this episode, Dr. Crear-Perry talks about eligibility for Medicaid expansion in Michigan requiring folks who lived in urban areas to have a job vs folks who lived in rural areas not needing to meet this requirement. What Dr. Crear-Perry mentions was a proposal that the State Senate wanted, but ended up doing away with before passing Medicaid expansion. See Reference 20 below for additional information.
References
Hardeman RR, Karbeah J, Kozhimannil KB. Applying a critical race lens to relationship-centered care in pregnancy and childbirth: An antidote to structural racism. Birth. 2020;47(1):3-7. doi:10.1111/birt.12462
Bekkar B, Pacheco S, Basu R, DeNicola N. Association of Air Pollution and Heat Exposure With Preterm Birth, Low Birth Weight, and Stillbirth in the US: A Systematic Review. JAMA Network Open. 2020;3(6):e208243-e208243. doi:10.1001/jamanetworkopen.2020.8243
Kozhimannil KB, Hardeman RR, Attanasio LB, Blauer-Peterson C, O’Brien M. Doula care, birth outcomes, and costs among Medicaid beneficiaries. Am J Public Health. 2013;103(4):e113-e121. doi:10.2105/AJPH.2012.301201
National Birth Equity Collaborative. Dr. Joia on BMHW & Why Black Women & Birthing People Are Experiencing Poor Outcomes | NBEC.; 2021. https://youtu.be/GPAlyT8tuhE
Improving Equity in Birth Outcomes, a Community-based, Culturally-centered Approach. Robert Wood Johnson Foundation Interdisciplinary Research Leaders Program. Published January 16, 2019. https://irleaders.org/team/improving-equity-in-birth-outcomes/
Henning-Smith C, Kozhimannil KB. Missing Voices In America’s Rural Health Narrative. Health Affairs Blog. Published April 10, 2019. 10.1377/hblog20190409.122546
Hostetter M, Klein S. Restoring Access to Maternity Care in Rural America. Published online 2021. doi:10.26099/CYCC-FF50
Hardeman RR, Karbeah J, Almanza J, Kozhimannil KB. Roots Community Birth Center: A culturally-centered care model for improving value and equity in childbirth. Healthcare. 2020;8(1):100367. doi:10.1016/j.hjdsi.2019.100367
Kozhimannil KB, Henning‐Smith C, Hung P. The practice of midwifery in rural US hospitals.. Journal of Midwifery & Women’s Health. 2016;61(4):411-418. doi:10.1111/jmwh.12474
Lopez-Carmen VA, Erickson TB, Escobar Z, Jensen A, Cronin AE, Nolen LT, Moreno M, Stewart AM. United States and United Nations pesticide policies: Environmental violence against the Yaqui indigenous nation. The Lancet Regional Health – Americas. https://www.sciencedirect.com/science/article/pii/S2667193X22000722#bib0044
Kozhimannil KB, Casey MM, Hung P, Prasad S, & Moscovice IS. (2016). Location of childbirth for rural women: implications for maternal levels of care. American journal of obstetrics and gynecology, 214(5), 661.e1–661.e10. https://doi.org/10.1016/j.ajog.2015.11.030
The hosts and guests report no relevant financial disclosures.
Citation
Crear-Perry J, Kozhimannil KB, Fields NF, Onuoha C, Lopez-Carmen VA, Krishnamurthy S, Calac A, Nolen L, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 17: ‘Just’ Births: Reproductive Justice & Black/Indigenous Maternal Health Equity.” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. May 31, 2022.
RLR discussed an intriguing case of a chronic consolidation
Thank you to our dear friend and colleague Dr. Kelley Chuang for her help with the production of this episode. (You are a legend, Kelley!) @kelleychuang
Patreon exclusive: RLR 93_Live from San Diego!!!
May 23, 2022
Dear Patrons!!!
We wish you a lovely week full of learning.
Huge shout out to our guest and dear friend, Anand, on this week’s episode. Anand is a trail blazer in making the invisible, in clinical reasoning, visible for undergradute medical trainees. https://twitter.com/AnandJag1
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time Dr. Doug Pet presents a case of slurred speech to Angelita and Diane.
Doug is a resident in neurology at UCSF. He grew up surrounded by cow farms and crab-apple trees in New Milford, CT. He completed a dual-degree program at Tufts and the New England Conservatory studying medical anthropology, community health, and jazz saxophone. He later worked for a non-profit in Berkeley, CA on bioethical and social justice issues related to genetic and reproductive technologies. Doug attended Vanderbilt University School of Medicine, after which he returned to the Bay Area for neurology residency at UCSF. He loves Brazilian music, playing Spikeball, and making custom wooden pens on his lathe.
Angelita Pusparani is a junior doctor (2ndY+) working in a small town in Indonesia. She is interested in discussing any cases (from neonate to geriatric), all patients inspire her. In her free time, Angelita is a basketball and marvel fan. She can also be found making a coffee or fried rice.
Diane Lebrun
Diane is an Internal Medicine Physician from Haiti. Her interest in Neurology started when she was a PGY-3 resident at Hopital Universitaire de Mirebalais (HUM), during her rotation in the Neurology Clinic. She has a special interest for Neuro-ICU, clinical reasoning, and medical education. In her free time, she enjoys spending quality time with family and friends, listening to faith-based music or podcasts, and dancing.
RR often discuss their fortune in finding such a supportive community.
We hope you enjoy the 2nd episode of the week. Huge shout out to the residents at Legacy Health in Portland. They are smart, kind, and hungry for diagnostic expertise. #Gratitude
Next Sunday we will learn what happened to part 2 of the Mathematician’s presentation – the patient w/ alc hep who returned with blood “per orum.”
Your grateful Mathematician and Magician (math + magic = RLR)
Patreon exclusive: RLR 90 w/ Krishna Ravindra
May 09, 2022
Hi Patrons,
You won’t want to miss this episode. Trust us. #EpicCase
Krishna is finishing his last week of MS3 year @ VCU School of Medicine. He did a PHENOMENAL job presenting the case.
Huge shout out to Dr. Patrick Fadden @ptfaddenMD, a superb clinician-educator, for guiding Krishna and being a great colleague to RR and CPSolvers.
RR are grateful to Krishna for his kindness, preparation, and stellar execution. Krishna, we will cheer on Madrid in the UEFA Champions League Final b/c we owe you for this special hour.
Episode 236: ARM Episode 16 – Live from SGIM: Best of Antiracism Research at the Society of General Internal Medicine’s 2022 Annual Meeting
May 03, 2022
Episode 16 – Live from SGIM: Best of Antiracism Research at the Society of General Internal Medicine’s 2022 Annual Meeting
Show Notes by Sudarshan Krishnamurthy
May 3, 2022
Summary: This episode was recorded in front of a live audience at the Society of General Internal Medicine’s 2022 Annual Meeting in Orlando, FL. In this episode, we gain insights from three antiracism scholars, Drs. Yannis Valtis, Ebi Okah, and Carine Davila, about research in their respective fields. Dr. Valtis is a 4th year Med-Peds Resident at Brigham & Women’s Hospital and Boston Children’s Hospital, and his research focuses on race and the utilization of security responses in the inpatient hospital setting. Dr. Okah is a family medicine clinician and NRSA research fellow at the University of North Carolina School of Medicine, and she studies the association between the use of race in medical decision-making and beliefs regarding the etiology of disparities in health outcomes. Dr. Davila is a palliative care physician at Massachusetts General Hospital and her work examines racial and ethnic inequities in patient-clinician communication. This episode was led by Rohan Khazanchi, and was hosted by Sudarshan Krishnamurthy and Utibe R. Essien.
Episode Learning Objectives
After listening to this episode learners will be able to:
Understand the association of race with the utilization of security responses in hospital settings
Understand the association between the use of race in medical decision-making and beliefs regarding the etiology of racial differences in health outcomes
Understand racial/ethnic inequities in trust-building healthcare experiences and describe the importance of improving trust in the healthcare system through trust-building experiences with historically marginalized communities
Credits
Written and produced by: Rohan Khazanchi MPH, Sudarshan Krishnamurthy, Utibe R. Essien MD, MPH, Jazzmin Williams, Alec J. Calac, Victor A. Lopez-Carmen MPH, Naomi F. Fields, LaShyra Nolen, Michelle Ogunwole MD, Jennifer Tsai MD, MEd, Chioma Onuoha, Ayana Watkins
Hosts: Sudarshan Krishnamurthy and Utibe R. Essien MD, MPH
Infographic: Creative Edge Design
Audio Edits: David Hu
Show Notes: Sudarshan Krishnamurthy
Guests: Drs. Yannis Valtis, Ebi Okah, and Carine Davila
Time Stamps
0:00 Introduction
4:20 Context and background of Yannis’ project
7:40 Framing of Ebi’s research
11:25 Inspiration for Carine’s work
14:50 Yannis’ explanation of his findings and potential next steps to intervene
25:45 Results from Ebi’s research
33:55 Carine’s findings from her work
40:00 Audience Questions
Episode Takeaways
Our Black patients are nearly twice as likely to experience a security utilization as our White patients.
Along with previous literature demonstrating a higher use of restraints in our Black patients in the emergency department setting, Yannis’ work shows a higher use of security responses in Black patients compared to White patients. Simulation-based training interventions are currently being studied to help combat these inequities.
Individuals who believe that genetic differences explain racial differences in health outcomes are more likely to practice race-based medicine.
Ebi’s research found that those physicians who possessed the belief that the etiology of racial differences in health outcomes was rooted in genetic differences were more likely to practice race-based medicine. On the other hand, those who believed that differences in social conditions explain racial differences in health outcomes were less likely to practice race-based medicine.
Our Black and Hispanic patients are less likely to have had trust-building experiences and more likely to have had trust-eroding experiences with the healthcare system.
Carine’s research illustrated the presence of trust-building experiences and trust-eroding experiences at every touchpoint with the health care system. Further, her research shows that Black and Hispanic patients are less likely to have had positive experiences and more likely to have had negative experiences. In addition to a need for culturally competent interpersonal communication, health systems and structures must actively work to build trust with historically marginalized communities.
Pearls
“When we heard the Code Gray bell go off in the hospital, all of us knew that there was a very high likelihood that we would be entering the room a Black patient.”
In the landscape of the murder of George Floyd, Yannis described how his team began to ask questions about how they could better protect their Black patients from police brutality. Although they began with a large focus on police brutality as a whole, they realized that the presence of police within the hospital had not been sufficiently examined. Although it had not been objectively measured, their clinical and personal experiences indicated that security responses were more often utilized for minoritized patients in the hospital.
“It did not make sense that an innate risk for poor health was attributed to Blackness, instead of thinking about how society assigns privileges and benefits by race that results in varying health outcomes.”
Ebi discussed the context behind what inspired her project, explaining that her journey began in medical school when students challenged race-based medical curricula and the use of race as a risk factor for disease. While starting residency, she was exposed to the use of race in clinical risk calculators and was confused by the rhetoric around the innate risk conferred by Blackness, instead of the influences of racism and inequitably distributed social determinants on health outcomes.
“There are known inequities in patient-clinician communication in historically marginalized populations that have immediate and downstream effects on health outcomes for these patients.”
Carine talked about her expertise in empathically communicating with patients as a palliative care physician. As she embarked on her project, she realized that improving serious illness care would require improving serious illness communication. She explained that the willingness for patients to engage in communication is rooted in how much they have been listened to in the past. Importantly, there is literature demonstrating inequities in patient-clinician communication with impacts on immediate outcomes, such as patient satisfaction and trust-building, along with downstream health outcomes
“… we found that the chance of having security called on our Black patients was nearly double that of our White patients.”
Yannis described previous studies demonstrating that Black patients have a higher likelihood of being restrained than White patients in the emergency department and psychiatric settings. However, there seemed to be a lack of literature exploring this in the inpatient hospital setting, where patient clinical presentations are more varied and management depends more on clinician behaviors. His team found that 1.5% of White patients had a security response called, in comparison to almost twice as many (2.8%) Black patients. Yannis posited that this difference was due to explicit and implicit biases rooted in racism in our broader societal context. When thinking about an intervention to combat these inequities, Yannis described a project at the Brigham leveraging simulation-based training on interacting with agitated patients followed by a debrief session to have clinicians reflect on their actions towards patients and the role of race.
“… we found that the belief in genetic differences explaining racial differences in health outcomes is associated with the practice of race-based medicine.”
Ebi’s work focused on how physicians think about race and how they engage in race-based medicine. Her project asks three main questions: 1) To what extent do racial differences in genetics explain racial differences in health outcomes? 2) How do values related to diet, exercise, and other cultural differences between racial groups explain racial differences in health outcomes? and 3) How do differences in social conditions, such as the environment and socioeconomic status, influence racial differences in health outcomes? Ebi found that the belief in genetic differences as an explanation for racial health disparities was associated with use of race-based clinical practices. Additionally, the belief that social inequalities explained racial health disparities was not associated with race-based practice.
“Our Black and Hispanic patients are less likely to have had positive experiences and more likely to have had negative experiences with the healthcare system.”
People engage in positive trust-building and negative trust-eroding experiences at every touch point or every interaction with someone in the healthcare system. Carine explains that this forms the framework for how experiences within the healthcare system can be evaluated. Unsurprisingly, it was found that Black and Hispanic patients were less likely to have had trust-building experiences and more likely to have had trust-eroding experiences with the healthcare system. Trust in the healthcare system is dependent on so many factors, and boils down to what the system has done to demonstrate that they are trustworthy. The onus is on us as a system to build and earn the trust of our patients through trustworthy behaviors, especially when the system has historically not done that. An important way of improving trust in the system within historically marginalized communities includes the recruitment of clinicians to the healthcare system from within these communities, to increase representation and better reflect the diversity of our patient population. The presence of these diverse clinicians also changes the inherent nature of the space that healthcare occupies.
References
Valtis YK, Stevenson K, Murphy E, Hong J, Ali M, Shah S, Taylor AD, Sivashanker K, Shannon E. Race and the Utilization of Security Responses in a Hospital Setting. Oral Presentation at Society of General Internal Medicine 2022 Annual Meeting. Orlando, FL.
Okah E, Cronholm P, Crow B, Persaud A, Westby A, Bonham V. The use of race in medical decision-making is associated with beliefs regarding the etiology of racial differences in health outcomes. Oral Presentation at Society of General Internal Medicine 2022 Annual Meeting. Orlando, FL.
Davila C, Ravicz M, Jaramillo C, Wilson E, Chan S, Arenas Z, Kavanagh J, Feltz B, McCarthy B, Gosline A. Talking the Talk: Examining racial and ethnic inequities in patient-clinician communication. Oral Presentation at Society of General Internal Medicine 2022 Annual Meeting. Orlando, FL.
Okah E, Thomas J, Westby A, Cunningham B. Colorblind Racial Ideology and Physician Use of Race in Medical Decision-Making. J Racial Ethn Health Disparities. 2021 Sep 7:10.1007/s40615-021-01141-1. doi: 10.1007/s40615-021-01141-1.
Ogunwole SM. Without Sanctuary. N Engl J Med. 2021 Mar 4;384(9):791-793. doi: 10.1056/NEJMp2030623.
Corbie-Smith G, Henderson G, Blumenthal C, Dorrance J, Estroff S. Conceptualizing race in research. J Natl Med Assoc. 2008 Oct;100(10):1235-43. doi: 10.1016/s0027-9684(15)31470-x.
Nash KA, Tolliver DG, Taylor RA, Calhoun AJ, Auerbach MA, Venkatesh AK, Wong AH. Racial and Ethnic Disparities in Physical Restraint Use for Pediatric Patients in the Emergency Department. JAMA Pediatr. 2021 Dec 1;175(12):1283-1285. doi: 10.1001/jamapediatrics.2021.3348.
Carreras Tartak JA, Brisbon N, Wilkie S, Sequist TD, Aisiku IP, Raja A, Macias-Konstantopoulos WL. Racial and ethnic disparities in emergency department restraint use: A multicenter retrospective analysis. Acad Emerg Med. 2021 Sep;28(9):957-965. doi: 10.1111/acem.14327.
The hosts and guests report no relevant financial disclosures.
Citation
Valtis Y, Okah E, Davila C, Krishnamurthy S, Essien UR, Calac A, Fields NF, Lopez-Carmen VA, Nolen L, Onuoha C, Watkins A, Williams J, Tsai J, Ogunwole M, Khazanchi R. “Episode 16: Live from SGIM: Best of Antiracism Research at the Society of General Internal Medicine’s 2022 Annual Meeting” The Clinical Problem Solvers Podcast – Antiracism in Medicine Series. https://clinicalproblemsolving.com/antiracism-in-medicine/. May 3, 2022
Dr. Blythe Butler presents a case to Dr. Alexandra “Jay” Teng, followed by a discussion about her experience as a woman in an Internal Medicine procedural subspecialty.
Alexandra “Jay” Teng
Alexandra “Jay” Teng hails from Berkeley and graduated from Harvard with a bachelor’s degree in history and science. After college, she worked at UCSF as a clinical research coordinator and patient navigator for women newly diagnosed with breast cancer, helping them prepare questions for their doctor and accompanying them to appointments. That experience helped convince her to pursue medicine. Dr. Teng earned her medical degree from UCSF, then completed internal medicine residency at UCLA. A competitive skier, she was originally interested in orthopedics, but she had a dramatic pivot at the end of her first year of medical school. “On the morning of my last final, I went into cardiac arrest and was admitted to Moffitt Hospital,” she said. The hospital team did an extensive workup, eventually diagnosing her with a rare condition called congenital long QT syndrome and implanting a cardiac defibrillator to prevent future life-threatening complications. “I was incredibly lucky, and feel a very personal connecting to cardiology,” she said. “I feel fortunate to train in the place and with the people who saved my life.”She completed Cardiology and Interventional Cardiology subspecialty fellowship at UCSF. She now works at Kaiser.
Blythe Butler
Blythe Butler is a first-year internal medicine resident at the University of California, San Francisco. She grew up in Spokane, Washington and attended Dartmouth College where she studied chemistry and mathematics. She went on to pursue a career in education and spent four years teaching general and AP chemistry as a high school teacher in San Jose, CA. She decided to switch careers to pursue medicine and completed medical school at UCSF. She enjoys running through Golden Gate Park, hiking and backpacking, and baking. Her career interests include medical education, communication in medicine, and health equity.
The only way we significantly grow is through reflection! Listen to this episode, reflect, and become better for the patient you treat tomorrow and the student you teach tomorrow.
We thank you for your support.
Is it Reza loves Rabih or Rabih loves Reza … it is the best palindrome …
In this case, Anna and Moses work through the schemas of dyspnea, AMS, HIV & infection, and lymphocytic pleocytosis as they discuss a case presented by Simone.
Episode 232: Anti-Racism in Medicine Series – Episode 15 – Housing is Health: Racism and Homelessness – Clinician + Community Perspectives
Apr 05, 2022
Episode 15: Housing is Health: Racism and Homelessness – Clinician + Community Perspectives
Show Notes by: Victor Anthony Lopez-Carmen, MPH
April 5, 2022
Summary: This episode highlights homelessness’ impact on health, the structural and racialized nature of homelessness, and practical interventions to address housing inequities. This is the last of three episodes interrogating the relationships between race, place, housing, and health. During this episode, we gained insight from special guests Dr. Margot Kushel and Mr. Bobby Watts about what brought them into their fields, how their work reaches the most marginalized, and what can be done at the community and structural level to address homelessness. Dr. Margot Kushel is a Professor of Medicine and Division Chief at the Division of Vulnerable Populations at Zuckerberg San Francisco General Hospital and Trauma Center and Director of the UCSF Center for Vulnerable Populations and UCSF Benioff Homelessness and Housing Initiative. Mr. Bobby Watts is the chief executive officer of the National Health Care for the Homeless Council. This episode was hosted by Sudarshan Krishnamurthy, Jazzmin Williams, and Alec Calac.
Episode Learning Objectives:
After listening to this episode, learners will be able to:
Learn about non-stigmatizing language for healthcare providers when talking about individuals experiencing homelessness
Understand how systemic racism, including injust housing policies and over-policing, are at the root of homelessness and its disproportionate impact on Black and Brown communities
Understand the systemic factors that have increasingly led to the aging population experiencing homelessness today
Learn how homelessness contributes to adverse health outcomes, especially in the context of the COVID-19 pandemic
Describe the utility of medical respite care when working with patients experiencing homelessness
Credits
Written and produced by: Sudarshan Krishnamurthy, Jazzmin Williams, Alec J. Calac, Victor A. Lopez-Carmen, MPH, Naomi F. Fields, LaShyra Nolen, Rohan Khazanchi, MPH, Michelle Ogunwole, MD, Utibe R. Essien, MD, MPH, Jennifer Tsai MD, MEd, Chioma Onuoha, Ayana Watkins
Hosts: Sudarshan Krishnamurthy, Jazzmin Williams, Alec J. Calac
Infographic: Creative Edge Design
Audio edits: David Hu
Show notes: Victor Anthony Lopez-Carmen, MPH
Guests: Dr. Margot Kushel and Mr. Bobby Watts
Time Stamps
00:00 Introduction
04:31 Guest career paths
11:58 Non-stigmatizing language around homelessness
19: 30 Structural racism and homelessness
33:09 Increasingly older population experiencing homelessness
42:01 Medical respite care
48:30 Criminalizing and over-policing homelessness
53:19 Key takeaways
Episode Takeaways
We must know the housing status of our patients, and how to ask about it.
Our guests remind us to ask our patients about their housing status using non-judgmental and non-stigmatizing language. If we do not know the housing status of our patients, then we do not know one of the most fundamental things that is going to affect their health and wellbeing.
2. Know your community resources.
Our guests emphasize that physicians must be familiar with community resources. Do you have a medical respite center? Do you have a coordinated entry system (CES) in your community? Can you refer your patient there?
3. If we are not part of the solution, we are complicit in structural injustice.
Dr. Kushel and Mr. Watts remind healthcare providers to speak out about the structural causes of homelessness. Push back against individual narratives that blame individuals for systemic injustice. Push back against dehumanizing language. Push back against discussions that homelessness is caused by substance use or mental health problems.
4. Disaggregated data on homelessness is vital.
Missing racial and ethnic data on homelessness is an example of structural racism. We must know who we are serving to truly be able to tackle the systemic injustices that cause disproportionate rates of homelessness in America.
Pearls
Formative Career Moments:
Dr. Kushel explained how discharging patients experiencing homelessness only for them to come back a few days later in worse shape was unacceptable. This pattern led Dr. Kushel towards work on solving the systemic failures causing “catastrophic” health outcomes in populations experiencing homelessness.
Mr. Watts added a tangible example where people experiencing homelessness would be dropped off by ambulances in front of the center for homelessness where he worked, which was not equipped to deal with their medical circumstances. They would eventually end up back at where the hospitals they came from. Experiences like this made him want to contribute to solutions in the community.
Speaking about Homelessness:
Dr. Kushel encouraged people to go past the textbooks and learn from people on the frontlines of homelessness. This humanizes the crisis and also centers the lived experiences of persons experiencing homelessness as the experts who can teach us more than any textbook.
Dr. Kushel emphasized that we should use person-first language because homelessness is an experience and there is no such thing as an inherently homeless person. Some people also prefer to use unhoused instead of homeless.
Mr. Watts encouraged use of the term neighbor, such as “neighbors without homes, unhoused neighbors, or neighbors experiencing homelessness. Another term he uses is “people with the lived expertise of homelessness,” which centers them as experts in solution-making.
Dr. Kushel detailed how the use of dehumanizing language equates to complicity in a narrative that systemically harms our neighbors with lived expertise in homelessness.
Dr. Kushel emphasized that we must speak to the structural racism at the root of disproportionate rates of homelessness in communities of color, instead of just focusing on mental health and substance use.
Restrictive Housing Policy and Homelessness Today:
Mr. Watts described how property tax laws give more public funding to school districts in higher socioeconomic neighborhoods than poorer neighborhoods, leading to worse educational outcomes and thus higher rates homelessness in low-income neighborhoods.
Dr. Kushel and Mr. Watts remarked that housing, especially expensive house ownership, is massively subsidized in comparison to apartment renting, meaning populations who are less likely to own houses receive less financial support from state and federal housing programs.
Dr. Kushel described how the wealth gap created by discriminatory housing policies also means that more racial minorities are renting properties, making them more vulnerable to gentrification and eviction, contributing further to the housing crisis.
Mr. Watts explained that predatory home or apartment lending targets Black and Brown people, leading to higher rates of poverty and homelessness in those communities. He also described how other policies like redlining and racist policing practices contribute to the mass incarceration of Black and Brown people, increasing homelessness in those communities.
Aging Compositions of the Population Experiencing homelessness across the US:
Dr. Kushel explained that in the early ’90s in San Francisco, 11% of those experiencing homelessness were 50 and older. By 2003, 37% were 50 and older. Now, among single adults experiencing homelessness, the median age is much closer to 50, meaning about half are under 50 and half are over 50. 44% had never once been homeless before the age of 50. So, the population experiencing homelessness is increasingly older.
Mr. Watts noted that the aging population experiencing homelessness came of age during mass incarceration, over policing, and thus many of them had histories with the prison system. Most were due to drug-related non-violent crimes that haunted them and limited employment opportunities throughout their lives.
Dr. Kushel also noted that housing became less and less affordable, adding on to the vulnerability of those in this generation who could not obtain well-paying jobs due to non-violent criminal histories.
Mr. Watts described how life expectancy among those experiencing homelessness is 20-30 years shorter than those with stable housing. This means they don’t benefit from social security because they are dying before they can receive it.
Health and Homelessness:
Dr. Kushel emphasized that people experiencing homelessness have elevated hospitalization rates and longer stays due to more comorbidities, and are more likely to be re-hospitalized.
Mr. Watts described how care for people experiencing homelessness needs to take into account the realities of being without a house, such as having medications stolen or going bad because of lack of refrigeration (e.g. insulin), greater decompensation after discharge because of a lack of a place to rest, and other factors that lead to poorer health outcomes.
Our guests explained that inpatient and outpatient treatment plans need to prioritize knowing the patients’ housing status, shared decision-making, and creating plans that take homelessness into account so treatment regimens are effective.
Dr. Kushel commented that in order to create systemic changes that will decrease rates of homelessness and improve the health outcomes of those experiencing homelessness we need disaggregated data to fully understand which groups in society are most impacted and why.
Medical Respite Care:
Mr. Watts advocated for medical respite, a safe place to heal and “short circuit” the street-emergency room-street-emergency room cycle as a way to treat people experiencing homelessness who are not sick enough for inpatient service, but too sick to send back out to the streets, only for their sickness to worsen. Because of less hospitalization return rates, Dr. Kushel emphasized that medical respite programs also save taxpayer money.
Dr. Kushel and Mr. Watts emphasized that respite medical care needs to be integrated into the continuum of care and homeless response systems.
Dr. Kushel explained that medical respite care via the National Institute for Medical Respite Care was very successful during the COVID-19 pandemic and is inspiring more and more communities to integrate respite care into their practices.
Policing:
Mr. Watts noted how the crack cocaine epidemic shifted the race demographics of homelessness in NYC from largely older, white drinkers to “50/50 young African American and Latinx”, with many cycling in and out of the carceral system due to over-policing and mass incarceration, which only made the crisis worse.
Mr. Watts emphasized that to this day, you are still more likely to be arrested for drug charges if you are Black or Brown, even though rates of drug use are equal across races. This is due to over policing of Black and Brown communities, which leads to higher rates of homelessness in those populations.
Mr. Watts and Dr. Kushel described how criminalizing homelessness is counter-productive and increases stigma, especially when the media focuses on one’s homelessness in the context of a crime. He states that people who are experiencing homelessness are actually more vulnerable to crimes happening to them, so they deserve more protection and service from the criminal justice system. Mr. Watts highlighted a program called CAHOOTS (Crisis Assistance Helping Out On The Streets) as a great, evidence-based mobile response model for addressing urgent needs among those experiencing homelessness.
Hahn JA, Kushel MB, Bangsberg DR, Riley E, Moss AR. BRIEF REPORT: the aging of the homeless population: fourteen-year trends in San Francisco. J Gen Intern Med. 2006;21(7):775-778. doi:10.1111/j.1525-1497.2006.00493.x
Semere W, Kaplan L, Valle K, Guzman D, Ramsey C, Garcia C, Kushel M. Caregiving Needs Are Unmet for Many Older Homeless Adults: Findings from the HOPE HOME Study. J Gen Intern Med. 2022 Feb 15:1–9. doi:10.1007/s11606-022-07438-z
Kushel M. Older homeless adults: can we do more?. J Gen Intern Med. 2012;27(1):5-6. doi:10.1007/s11606-011-1925-0
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Watts B, Kushel M, Krishnamurthy S, Williams J, Calac AJ, Lopez-Carmen VA, Fields NF, Nolen L, Tsai J, Ogunwole SM, Onuoha C, Watkins A, Essien UR, Khazanchi R. “Episode 15: Housing is Health: Racism and Homelessness – Clinician and Community Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. April 5, 2022.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Vijay presents a case of left upper extremity weakness to Vale and John.
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue a Neurology residency. Her interests include neuro-infectious diseases, transgender health, and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine, she loves running, hiking, cooking pasta, and spending time with her dogs.
John Acquaviva
@DrJAStrange
John Acquaviva is a third-year medical student attending Lake Erie College of Osteopathic Medicine in Erie, Pennsylvania. He has a passion for both clinical and academic neurological concepts and plans to practice neurology after medical school. He has a special interest in autoimmune neurology and neuroimmunology, but is excited about all neurological clinical presentations. In his free time, he enjoys hanging out with friends, long-boarding, and running while listening to neurology podcasts.
Vijay Balaji
@VijayBramhan
Vijay is currently a third-year internal medicine resident at Ramaiah Medical College & Hospital, Bangalore, India, and has interests in medical education and clinical reasoning. Outside academics, his interests include playing basketball, cooking, and philosophy.
Dr. Aisha Rehman, thank you for taking the time to present your patient’s case.
We are still awaiting a final diagnosis. Dr. Rehman and RR would appreciate any thoughts you might have regarding her patient. Please comment below or send us a private message. There will definitely be a part 2 as more data returns.
Patreon exclusive: RLR 80 with Uncle Bob – Hyperkalemia
Feb 28, 2022
It is hard to believe we are already at 80 episodes with 719 patrons. We cannot thank each of you enough for allowing RR to chase their dream of teaching/learning diagnostic reasoning. We all are on an epic journey together.
This episode is very special because we feature a mentor, advisor, and supporter of CPSolvers’ effort from day 1 and episode 2 (hyponatremia). We feel lucky to know Uncle Bob. He is a great human being, physician, and teacher.
Make sure to listen after our outro theme song for case updates by UB.
Cardionerds, Tommy and Dinu, present a case to Dr. Vaidya, Lindsey, and Dan.
Dr. Anjali Vaidya
Dr. Vaidya is a heart failure and transplant cardiologist at the Lewis Katz School ofMedicine at Temple University, where she serves as the co-director of the Pulmonary Hypertension, right heart failure, and CTEPH program, as well as APD for the cardiology fellowship program and residency advisor for the internal medicine residency.
Episode 14: Race, Place, and Health: Clinician and Community Perspectives
Show Notes by Alec Calac
February 15th, 2022
Summary: This episode highlights how racism manifests in the built environment, and how community and individual-level efforts can mitigate these inequities. This discussion is the second of three planned conversations around the connections between race, place, and health. Our latest episode welcomes first-time guests Dr. Eugenia South, a physician-scientist and Vice Chair for Inclusion, Diversity, and Equity in the Department of Emergency Medicine at the Perelman School of Medicine, and Noelle Warford, Executive Director of the grassroots organization Urban Tree Connection. Hosted by team members Naomi Fields and LaShyra Nolen,our guests present their community-based work in Pennsylvania and lay bare the connections between race, place, and health.
Episode Learning Objectives:
After listening to this episode, learners will be able to…
Understand the historical and present-day role of land dispossession and property rights in determining health along lines of race and place.
Learn how advancing individual agency and distributive justice can empower community organizers and initiatives.
Understand the factors that promote and inhibit long-term resiliency and sustainability of place-based initiatives.
Learn how we can reimagine health by decolonizing wealth and philanthropy in modern society.
Credits
Written and produced by: Naomi F. Fields, LaShyra Nolen, Rohan Khazanchi, MPH, Michelle Ogunwole, MD, Alec Calac, Victor Lopez Carmen, MPH, Utibe R. Essien, MD, MPH, Jennifer Tsai MD, MEd, Sudarshan Krishnamurthy, Chioma Onuoha, Dereck Paul, MD, MS, Ayana Watkins, Jazzmin Williams
Hosts: Naomi F. Fields, LaShyra Nolen
Infographic: Creative Edge Design
Audio edits: David Hu
Show notes: Alec Calac
Guests: Dr. Eugenia South, MD, MSPH, and Noelle Warford, MSW
Time Stamps
00:00 Introduction
05:40 Built environments and structural racism
11:18 Agricultural perspective, land rights, and settler colonialism
15:00 Responsible community engagement and catalyzing individual agency
21:58 Engaging communities outside of the ivory tower
27:00 Scaling up interventions to the community level
32:29 Intervention sustainability
37:18 Decolonizing philanthropy and place-based investments
42:40 Navigating trade-offs and mitigating ethical tensions
49:20 Key takeaways
Episode Takeaways
1. Your “why” has to be clear before you engage in community-based work.
Ms. Warford reminds us that we need strong, sound ideological positions and guiding principles before engaging with the communities around us. She asks to think about what we are doing today to make it easier for people to live in the future. Our ancestors considered our present to be impossible, so how can we use our ideas and experiences to effect positive change in our communities? These movements require action, not passivity.
2. Take time to learn from your patients. Be curious.
Clinicians are incredibly privileged individuals. Dr. South reminds us that it is our great honor to talk to people in an exam room. Our patients are not just a list of problems. They are individuals who interact with environments that affect their health. She encourages us to see beyond these problems, and ask patients about their lives, challenges, and successes. Everything is important. Unfortunately, medical practice does not always allow us to slow down and take this time to listen. But, finding ways to do so can prove illuminating as well as rewarding.
Pearls
Built Environment, Physical Health, and Mental Health
Dr. South detailed that there are clear physical health benefits associated with place-based interventions, but unfortunately many lots and buildings sit vacant and destitute across the US. There’s also more. When interviewing community members in Philadelphia, she shared that longstanding disinvestments in their communities made them feel “unimportant” and “neglected” by society, which had effects on their mental health.
The 2021 Build Back Better Act recognized the impact that the built environment has on health, calling for environmental improvements such as planting trees.
Ms. Warford is the Executive Director of Urban Tree Connection, a grassroots organization in West Philadelphia that uses land-based strategies and urban agriculture as tools for fostering community leadership and power. She presented a powerful argument that connected settler colonialism, Indigenous genocide, and chattel slavery with modern-day property rights and tax codes. By preventing Black and Brown people from developing relationships with the land and using it as a way of forming social connection, as well as communal sustenance, structural racism manifests along lines of race and place.
Lash echoed this and also reaffirmed points made by Dr. South that the built environment changes how individuals see themselves, limiting their ability to push back on the status quo.
Individual Agency and Redistribution of Resources
Ms. Warford centered the conversation and reminded the audience that it is not just healthcare systems that are being pushed to the brink. Non-profit organizations are experiencing the same organizational stress. Working with Dr. South and others, Urban Tree Connection is helping community members realize their inherent agency and leadership capacity.
In the process of redesigning the Memorial Garden in West Philadelphia, Ms. Warford and Dr. South foregrounded the reality that spaces have to be rooted in people’s experiences. There is often a sentiment that “If you build it, they will come”; however, one should not make assumptions about what community members want. It is important to get their perspectives and figure out what the “little things” are. The vision for any community-informed project has to meet community members where they are. What are their priorities? What are their needs?
Continuing this conversation, Dr. South shared that “solutions have to be solutions, not fantasies.” Approaching community problems with an academic approach will not necessarily have community interests in mind (or prioritize them). By moving outside of this academic mindset, organizers and facilitators can work to effect meaningful, long-lasting change in the community.
Sustainability
Dr. South has studied a variety of place-based interventions including vacant lot greening, abandoned house remediation, tree planting, and structural repairs to homes. She was recently awarded a $10 million grant from the National Institutes of Health that will allow her and her team to conduct a randomized-controlled trial that combines many interventions instead of just one. A serious concern that she and many others have is the sustainability of interventions after grant funding ends. Funding structures, especially from government agencies, are not exactly permissive of this.
To promote sustainability, Dr. South and Ms. Warford encouraged the audience to confront the ethical tension between place-based interventions and long-term sustainability after funding streams dry up. It is important to educate and engage key stakeholders such as policymakers who can work to address these limitations.
Ms. Warford shared that funding priorities are not necessarily community priorities. In limited funding environments, non-profit organizations often apply for any and all available funding streams, which may gradually shift the organization’s priorities, a phenomenon often referred to as mission creep.
Decolonizing Wealth and Philanthropy
Our panelists detailed how much wealth is generated from the labor of Black and Brown people. Unfortunately, it is difficult for that wealth to be reinvested in those very same communities. Ms. Warford encouraged our listeners to think about how we can decolonize wealth and philanthropy, noting that place-based investments have to be gradual and intentional. She shared that funding entities must recognize the labor of community members and provide funds for their work. “People power” is a resource that must be cultivated, respected, and valued.
Recognizing Your Role
Naomi recapped much of the discussion and shared that it was clear that “there is no quick fix.” Much of the work involves education, finances, time, and people power. Dr. South shared that there are many ways to be a part of dismantling structural racism. Some people are more front-facing, while others work behind-the-scenes. All perspectives and skillsets are welcome in this process. Ms. Warford shared that it will take time to navigate away from capitalist structures and extractive economies. It is important to celebrate the small wins and strive for the greater vision. LaShyra shared some personal reflections to this effect. The goal for this work will always be liberation and agency. When you’re just trying to make it every day, you don’t always have the privilege to do anything else.
“A Randomized Controlled Trial of Concentrated Investment in Black Neighborhoods to Address Structural Racism as a Fundamental Cause of Poor Health.” National Institutes of Health RePORTER. Accessed January 2, 2022. https://reporter.nih.gov/project-details/10413510#description
The hosts and guests report no relevant financial disclosures.
Citation
South E, Warford N, Fields NF, Nolen L, Calac A, Lopez-Carmen V, Tsai J, Krishnamurthy S, Ogunwole M, Onuoha C, Watkins A, Williams J, Paul D, Essien UR, Khazanchi R. “Episode 14: Race, Place, and Health: Clinician and Community Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. February 15, 2022.
Patreon exclusive: RLR 77 – Jaundice and weight loss
Feb 03, 2022
Dear Patrons,
We enjoyed this tremendously. It was an honor to discuss a case at the University of Pittsburgh Medical Center.
We hope you enjoy it.
Ryan, we cannot thank you enough for being such an amazing friend and colleague. You put the case together expertly. You presented it flawlessly. You made it an experience we will cherish forever.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Maria presents a case of increased drowsiness to Dr. Mathieu Brunet and Dr. Mattia Rosso.
Maria Jimena Aleman María Jimena Alemán was born and raised in Guatemala where she currently works in community and rural health care. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Ella Fitzgerald. Outside of medicine she enjoys modern art, 21st century literature, and having hour long conversations over a nice hot cup of coffee or tequila.
Mathieu Brunet
Mathieu Brunet is an emergency physician and trauma team leader at the Hôpital du Sacré-Coeur-de-Montréal and an assistant professor of emergency medicine at Université de Montréal in Canada. After his emergency medicine training, he completed a Fellowship in Resuscitation & Reanimation at Queen’s University in Canada and a Master of Traumatology with the University of Newcastle in Australia. Mathieu has been a regular listener of the podcast and the daily Virtual Morning Reports. He finds The Clinical Problem Solvers to be an invaluable resource to progress and maintain motivation on the lifelong journey toward clinical reasoning expertise.
Mattia Rosso
Mattia Rosso is a neurology resident at the Medical University of South Carolina (MUSC) in Charleston. He is interested in movement disorders, behavioral neurology, and autoimmune neurology. He is also passionate about the intersection between the humanities and medicine, with a focus on the fields of medical history and bioethics. Outside work, he enjoys photography, cinema, and discovering new music. Since starting residency, Clinical Problem Solvers have been an irreplaceable source of learning and inspiration.
In this episode, Dr. Elliot Tapper discusses a clinical unknown case presented by Dr. Jennifer Mundell
Jennifer Mundell
Jennifer Mundell, MD FACP is the associate program director for Ascension St Vincent Internal Medicine Residency Program. She graduated from University of Louisville School of Medicine and completed IM residency at Ascension St. Vincent in 2016. The residents best know her for building differentials, baking cakes, and owning more cars than garage spaces. During her free time, she enjoys writing up interesting cases with residents, taking her family to a beach, and planning next year’s Halloween decorations.
Elliot Tapper, MD is an Assistant Professor in the Division of Gastroenterology at the University of Michigan in 2016. His clinical activity and research efforts focus on the outcomes of patients with cirrhosis, particularly those with hepatic encephalopathy. He did his residency and was resident, chief resident, and a fellow in gastroenterology and transplant hepatology, at Beth Israel Deaconess Medical Center where he served as Director of Quality Improvement for the Liver Center. He is very active on twitter and tweets at @ebtapper
Emma presents a case to Dr. Yao Heng, followed by a discussion about her experience as a woman in Internal Medicine procedural subspecialty.
Dr. Yao Heng
Dr. Yao Heng was born in Bangkok, Thailand. She immigrated to the US in her 20’s. After graduating from the University of California, Berkeley with a Bachelor of Arts in Biochemistry, she received her medical degree at the University of California, San Francisco. She completed her residency in Internal Medicine at the University of California, San Francisco and specialty fellowship in Gastroenterology at the University of Washington. She went to University of Brugmann in Brussel, Belgium for special training in biliary tract disorders. She has been practicing gastroenterology and hepatology at Kaiser Permanente since 1992. She is currently in charge of the capsule endoscopy and balloon enteroscopy programs at San Francisco Kaiser. She has a strong interest in small bowel disorders, the microbiome and gut directed hypnotherapy.
Doug presents an unknown case of vision loss to Dr. Cherayil, Lindsey and Dan.
Dr. Neena Cherayil. Dr. Cherayil is an Assistant Professor of Neurology in the Departments of Neurology and Ophthalmology at Northwestern University Feinberg School of Medicine in Chicago, Illinois. She completed her neurology residency followed by a neuro-ophthalmology fellowship at the University of Pennsylvania. She is currently associate clerkship director of the neurology clerkship at Feinberg as well as co-module leader for the MS2 Neurosciences course. She enjoys leading morning report every week with the neurology residents and students and seeing the fascinating spectrum of afferent and efferent neuro-ophthalmic complaints in clinic. Her particular academic interests include diagnostic reasoning and curricular development with a focus on neuro-anatomic localization. Her favorite cranial nerve is, of course, CN III – the oculomotor nerve.
Episode 215: Vaccine Hesitancy – with Dr. Davis and Dr. Villela
Dec 27, 2021
CPSolvers team members Rafael Medina and Simone Vais take a moment to reflect on what is going on in the world of medicine focusing on vaccine uptake with two incredible experts on the matter about what their experiences have been.
Dr. Davis is the Director of Health for the City of St. Louis. Dr. Hlatshwayo Davis received her medical degree from Cleveland Clinic Lerner College of Medicine and a Master’s in Public Health Degree from Case Western Reserve University. She completed her internal medicine residency at University Hospitals Case Medical Center. She went on to complete her Infectious Diseases fellowship at the Washington University School of Medicine (WUSM), also completing a one year HIV fellowship and a Sexually Transmitted Infections (STI) fellowship. She has held many, many positions throughout her illustrious career in medicine. Dr. Hlatshwayo Davis is now a national and international medical contributor on COVID-19 with a particular focus on marginalized populations, as well as the Director of Health for the city of St. Louis (among much else). Her career passions include community engagement, the care of people living with HIV and the impact of COVID-19 infection in marginalized populations.
Dr. Villela is a graduate of Tucson High School, Yale University, and the University of Connecticut School of Medicine. She currently serves as Chief of Family and Community Medicine at San Francisco General Hospital and is Professor and Vice Chair in the UCSF Department of Family and Community Medicine.
Her interests include chronic illness care, family medicine education, reproductive health, health of Latinxs in the U.S., and health care disparities. Her clinical practice includes inpatient adult medicine, short-term nursing home care, and ambulatory family medicine. She lives with her partner in the Mission district of San Francisco; they have a daughter who is a junior in college. All three are vaccinated against COVID and 2 of 3 have had boosters.
Patreon exclusive: RLR 73 – the case of a patient phone call…
Dec 26, 2021
Episode 13: Centering Asian Americans: Racism, Violence, and Health
Show Notes by Naomi F. Fields
December 21, 2021
Summary: This episode is about racism faced by Asian-Americans, why it often goes unrecognized, and how we can work to rectify these wrongs. This discussion is hosted by Jazzmin Williams, Rohan Khazanchi, MPH, and Jennifer Tsai MD, MEd, as they interview Thu Quach, PhD, an epidemiologist and galvanizing leader who has led the Asian Health Services (Oakland, CA) in addressing racial disparities in COVID-19, and Tung Nguyen, MD, a Professor of Medicine at the University of California, San Francisco, and a nationally-renowned health disparities researcher. Our inspiring guests help us to contextualize struggles faced by Asian-Americans even as they outline and energize within us a path forward – together.
Content Warning: This episode contains themes of violence, trauma-induced mental health concerns, and brief mentions of suicide. If you or someone you know is struggling with suicidal thoughts, please call the National Suicide Prevention Hotline at 800-273-8255, that’s 800-273-TALK.
Episode Learning Objectives:
After listening to this episode learners will be able to…
Define the myth of the “Model Minority” and explain how it impacts the racism experienced by Asian-Americans.
Describe how divisiveness amongst minoritized groups was and remains politically orchestrated, and how minority groups can work together in solidarity against White oppression.
Appreciate how intergenerational trauma may surface amongst Asian-Americans, and how these intergenerational relationships may also offer fertile ground for generating understanding.
Highlight how structural racism against Asian-Americans surfaces in clinical settings, and describe means of counteracting such structures.
Understand how engaged community-based work, centered on trust and accountability, has supported the health of communities served by Oakland, CA’s Asian Health Service.
Reckon with the health disparities that exist amongst Asian-Americans, how such disparities are related (in part) to insufficient data-gathering, inequitable clinical settings, and violence, and how they were further exacerbated by the COVID-19 pandemic.
Credits
Written and produced by: Jazzmin Williams, Rohan Khazanchi, MPH, Jennifer Tsai MD, MEd, Alec Calac, Victor Lopez-Carmen, MPH, Utibe R. Essien, MD, MPH, Sudarshan Krishnamurthy, Naomi F. Fields, LaShyra Nolen, Chioma Onuoha, Ayana Watkins, and Michelle Ogunwole, MD
Hosts: Jazzmin Williams, Rohan Khazanchi, MPH, and Jennifer Tsai MD, MEd
Infographic: Creative Edge Design
Audio edits: David Hu
Show notes: Naomi F. Fields
Guests: Thu Quach, PhD, and Tung Nguyen, MD
Time Stamps
00:00 Introduction
04:00 How Dr. Thu Quach’s and Dr. Tung Nguyen’s journeys shape their work
11:40 Policy work as a way of mitigating burnout
12:55 Balancing individual and communal focus (include?)
16:35 Impact of the COVID-19 pandemic on Asian communities in Oakland
17:40-17:50 Content Warning: Mention of suicide
22:25 Forms of Anti-Asian racism
25:17 The danger of gaslighting Asian-Americans and of comparing oppressions
27:51 Explanation of the model minority myth and a deeper dive into comparative oppressions
30:03 Engaging with community members via validation, and operationalizing means of working against anti-Asian racism
33:58 Dr. Jennifer Tsai reflecting on her father’s experience
37:10 Dr. Nguyen on pathways to intergenerational connection and combatting erasure
39:45 Dr. Quach on intergenerational trauma and reconciliation
43:56 Rohan Khazanchi reflecting on Asian-American disparities in Nebraska and community strength
46:30 Data collection and disaggregation: strengths, challenges, and insufficiencies
56:14 Structural anti-Asian racism in clinical settings
59:22 Clinical tools and takeaways
Episode Takeaways:
Recognize that structural barriers can embed anti-Asian racism into clinical settings.
Insufficient language services (i.e., provision in only English +/- Spanish), limitations of medical technology (i.e., difficulty of sending patient messages through the electronic medical record in languages other than English), limited healthcare literacy, and English-only signage on healthcare campuses are just a few of the structurally racist barriers faced by many Asian folks seeking healthcare. Dr. Nguyen encourages us to recognize how such barriers represent assumptions about people’s capabilities, how they can worsen people’s healthcare, and how they communicate exclusion to our Asian patients.
See the world through others’ eyes, and act.
Dr. Nguyen calls us to ask ourselves: “If [my] mother and father were like this person, how would they negotiate the system that I’m in? What can I do to either ameliorate those problems, or to fix those problems behind the scenes, so they don’t have to deal with them on a day to day basis?” This can help us reach the goal of taking care of patients in the ways that they want to be taken care of, by operationalizing the vision Dr. Quach shared for “letting lived experiences guide us.”
Create spaces to have conversations about the broader contexts affecting patients.
Dr. Quach reminds us that environmental factors and the political landscape affect patients’ wellbeing everyday. Creating spaces where these experiences can be shared by patients as well as by practitioners can highlight the structural nature of seemingly individualized problems. By appreciating the impact of factors affecting entire communities, we can be better positioned to act upon them.
Remember that more deeply understanding your patients can provide meaning!
Seeking to more deeply understand your patients is not an additional burden: ultimately, it is an additional benefit. Dr. Nguyen describes that in his experience, striving for understanding deepens the patient-provider relationship over time and offers fulfillment to him as well as to his patients.
Pearls
Case study: Oakland, CA’s Asian Health Services’ origin, ethos, and lessons
Dr. Quach describes the community- and advocacy-based origins of Asian Health Services, a Federally Qualified Health Center in Oakland, CA. She also describes their role in detecting and relaying the double-bind of challenges (COVID-19 and racism) being faced by community members throughout the pandemic, and how her team generated solutions that signaled their ongoing responsibility to the communities they served.
Asian-Americans face both apparent and enshrouded forms of racism, both of which have directly related health effects.
Dr. Nguyen goes on to expand on these forms. One form includes the eye-catching racist acts that explicitly manifest anti-Asian sentiments, such as violence toward elders, verbal abuse, and gun violence. In addition to the physical wrongs done to the victims, these acts function as community stressors that harm the mental, emotional, and physical wellbeing of so many others.
Another more insidious form of racism is erasure. This often manifests in a glaring lack of recognition of many of the problems faced by many Asian Americans. In the healthcare space, it can also result in a lack of data collection to demonstrate and understand issues faced by these groups. As a result, there are often failures to address their unique needs.
The “Model Minority” myth engenders both the racist erasure of Asian-Americans and division amongst minority groups.
Created in the 1960s by conservatives seeking to divide minority groups during the Civil Rights Movement, the model minority myth projects the relative success of some Asian-Americans onto all Asian-Americans; and subsequently casts them as an “ideal” group unaffected by the problems and negative stereotypes that plague other minority groups. In so doing, the model minority myth obscures how White supremacy actually affects Asian-Americans, and perpetuates a zero-sum game which pits minority groups against each other rather than alongside each other in solidarity.
Data on the problems faced by Asian Americans is lacking. This perpetuates further erasure of Asian-American health disparities, and there are multiple needed interventions to redress this injustice disparity.
Erasure often conceals the need for the collection of information that would spotlight challenges/inequities faced by Asian-Americans. For instance, Dr. Nguyen describes how the National Academy of Medicine and the Centers for Disease Control, amongst other major health organizations, issued valid and needed statements about the impact of COVID-19 on other minority groups, but did not mention the problems faced by Asian- Americans – nor the fact that the data was insufficient. The resulting message implied to the public was that no problems existed.
Additionally, data collection practices often do not capture all experiences due to usage of inaccessible language, or neglecting to spotlight voices from the most marginalized community members.
Data disaggregation, which seeks to spotlight specific ethnic groups within the Asian diaspora, can be a helpful step in better understanding the experiences unique to Asian-American communities we serve. It requires recognizing the diversity of experiences and gaining buy-in from community members.
“You don’t fight fire with fire, you fight fire with water.” – Fred Hampton
Dr. Nguyen mentioned this quote, and expounded upon it to say, “You don’t fight racism, with more racism you fight racism with solidarity and partnership and coalition building.” Although the Model Minority myth has generated divisiveness amongst minority groups, true power can come from folks turning away from gaslighting and the wrly named “Oppression Olympics” to recognize that we all need to work together against the real enemy: Oppression writ large by White supremacy.
Within Asian-American communities, intergenerational relationships can be a critical strength.
Multiple members of this episode describe challenging experiences with bridging understanding of their elder family members that may mirror dynamics within Asian-American communities more broadly.
On the one hand, these relationships convey the intergenerational traumas (of migration, of racism, and the like) that impact elders’ experiences, yet may differ from those of younger individuals.
Simultaneously, these relationships present opportunities to connect interpersonally as “genuine human beings,” and to find solution-generating commonalities.
Relatedly, our guests both describe experiences acting as “cultural brokers” to assist with healthcare needs of their elders that impacted their own journeys into medicine. These insights primed them to understand what challenges community members might be facing now.
Public Broadcasting Service. “Asian Americans: The history of identity, contributions, and challenges experienced by Asian Americans.” https://www.pbs.org/show/asian-americans/
Chu JN, Stewart SL, Gildengorin G, et al. Effect of a media intervention on hepatitis B screening among Vietnamese Americans. Ethn Health. 2019;1-14. doi:10.1080/13557858.2019.1672862
Quach T, Von Behren J, Tsoh J, et al. Improving the knowledge and behavior of workplace chemical exposures in Vietnamese-American nail salon workers: a randomized controlled trial. Int Arch Occup Environ Health. 2018;91(8):1041-1050. doi:10.1007/s00420-018-1343-2
Yan BW, Hwang AL, Ng F, Chu JN, Tsoh JY, Nguyen TT. Death Toll of COVID-19 on Asian Americans: Disparities Revealed. J Gen Intern Med. 2021 Nov;36(11):3545-3549. doi: 10.1007/s11606-021-07003-0.
Jones CP, Maybank A, Nolen L, Fields N, Ogunwole M, Onuoha C, Williams J, Tsai J, Paul D, Essien UR, Khazanchi, R. “Antiracism in Medicine – Episode 5: Racism, Power, and Policy: Building the Antiracist Health Systems of the Future.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/antiracism-in-medicine/. January 19, 2021.
Kawai, Yuko. (2005). Stereotyping Asian Americans: The Dialectic of the Model Minority and the Yellow Peril, Howard Journal of Communications, 16:2, 109-130, DOI: 10.1080/10646170590948974
Smith, Andrea. “Chapter Six: Heteropatriarchy and the Three Pillars of White Supremacy: Rethinking Women of Color Organizing”. Color of Violence: The INCITE! Anthology, edited by INCITE! Women of Color Against Violence, New York, USA: Duke University Press, 2016, pp. 66-73. https://doi.org/10.1515/9780822373445-008
The hosts and guests report no relevant financial disclosures.
Citation
Quach T, Nguyen T, Williams J, Tsai J, Fields NF, Calac A, Lopez-Carmen V, Krishnamurthy S, Nolen L, Onuoha C, Watkins A, Williams J, Essien UR, Ogunwole M, Khazanchi R. “Antiracism in Medicine – Episode 13: Centering Asian Americans: Racism, Violence, and Health.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/antiracism-in-medicine/. December 21, 2021.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Maria presents a case of episodic transient loss of consciousness to Gabriel and Ravi.
Maria Jimena Aleman was born and raised in Guatemala where she currently is a medical student in Universidad Francisco Marroquin. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She also looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Louis Armstrong. Outside of medicine she enjoys modern art, 21st century literature and having hour long conversations over a nice hot cup of coffee or tequila.
Gabriel Talledo
Gabriel is a MS2 student from Cayetano Heredia University. When it comes to medicine, he enjoys dermatology, infectiology, and LGBTQ+ health. He fell in love with his career when he understood medicine not just as a concept of knowledge but a combination of knowledge and social justice pursuit. He loves cooking Peruvian cuisine (one of the best in the world), eating, jogging and watching TV series. Recently he is doing a transgender education program at his university and a volunteering of sexual education in Lima schools.
Dr. Kushal Vaishnani is a Hospitalist at Atrium Health. He finished his medical school at B.J. Medical College, Ahmedabad, India. He completed his transitional year at Brandon Regional Hospital and Internal Medicine residency at LSUHSC – University Hospital and Clinics in Lafayette. His academic interests include clinical reasoning, medical education, high value care, and infectious diseases.
Saman is from Tucson, AZ. He graduated from the University of Arizona College of Medicine, finished internal medicine residency at Columbia, and his infectious diseases fellowship at Johns Hopkins. He is now working as a transplant ID physician at the University of Arizona. He is also completing his Master’s of Education in the Health Professions. He enjoys cooking with Reza and washing the dishes. In his spare time, he loves to watch PJ Masks with his wife and son, who was featured in Episode 42 as AstroBoy.
Brandon Pearce is a third-year Internal Medicine resident at Ascension St. Vincent in Indianapolis. His medical interests include pulmonary critical care and clinical education. In his spare time, he enjoys basketball, hiking with his fat Labradors, and traveling.
Episode 209: Antiracism in Medicine Series – Episode 12 – Our Land is Our Health: Addressing Anti-Indigenous Racism in Medicine
Nov 22, 2021
Episode 12: Our Land is Our Health: Addressing Anti-Indigenous Racism in Medicine
Show Notes by LaShyra Nolen
November 23rd, 2021
Summary: This episode is about the ways we can combat anti-Indigenous sentiments and actions in our efforts to promote anti-racism in medicine and public health. This discussion is hosted by our new team members Alec Calac and Victor Lopez-Carmen, as they interview Dr. Tom Sequist, member of the Taos Pueblo Tribe and Chief Patient Experience and Equity Officer at Mass General Brigham, and Dr. Sophie Neuner, proud member of the Karuk Tribe, and a Research Associate at the Johns Hopkins Center for American Indian Health. Together, these two phenomenal guests help us understand the structural and individual challenges of Indigenous peoples in academic medicine, public health, and beyond.
Episode Learning Objectives:
After listening to this episode learners will be able to…
Understand the historical and present-day role of settler colonialism behind health disparities in Indigenous populations.
Learn ways to address the lack of representation of Indigenous peoples in academia and how to create safe learning environments for Indigenous peoples in these academic spaces.
Understand the importance of disaggregated health data and how the burden of proof for “blood quantum” requirements can be detrimental to Indigenous peoples.
Learn the ways COVID-19 and climate change have exacerbated health inequities within Indigenous populations.
Learn tangible ways to center the Indigenous communities in advocacy efforts at the interpersonal and institutional level.
Credits
Written and produced by: Rohan Khazanchi, MPH, Michelle Ogunwole, MD, Alec Calac, Victor Lopez Carmen, MPH, Utibe R. Essien, MD, MPH, Jennifer Tsai MD, MEd, Sudarshan Krishnamurthy, Naomi F. Fields, LaShyra Nolen, Chioma Onuoha, Dereck Paul, MD, MS, Ayana Watkins, Jazzmin Williams
Hosts: Alec Calac and Victor Lopez Carmen, MPH
Infographic: Creative Edge Design
Audio edits: David Hu
Show notes: LaShyra Nolen
Guests: Dr. Tom Sequist, MD, MPH and Dr. Sophie Neuner, MD, MPH
Time Stamps
00:00 Introduction
05:25 What do I call you?
10:37 “Blood quantum” and the burden of proof
18:05 Challenges of Indigenous Peoples in medical spaces
24:50 COVID-19 and climate change’s impact on Indigenous Peoples
30:27 Racism in academia and creating safe spaces
41:22 “Data genocide”
50:11 What can listeners do going forward?
62:10 Key takeaways
Episode Takeaways:
Take the time to learn about how Indigenous Peoples influence the world around you.
From the street names of the cities in which we live to the nature that surrounds us, Dr. Sequist reminds us of the importance of taking the time to learn about how Indigenous Peoples have influenced and continue to influence every aspect of our lives. He encourages us to learn about the original inhabitants of lands on which we reside and to do the work to learn about the ongoing contributions from tribes around us. This is especially important when we consider the lasting role colonialism, genocide, and racism has played in attempted erasure of these communities and their culture.
Learn about the good and the ugly when it comes to the history of Indigenous Peoples.
Victor reminds us that we can hold two truths at the same time. Dr. Sequist also encourages us to, in addition to learning about the rich cultural traditions and invaluable contributions of Indigenous Peoples, to also acknowledge the historical and ongoing oppression these communities face. Indigenous Peoples continue to suffer disproportionately from health inequities, mental illness, poverty, climate change and police brutality, all of which have been exacerbated by the COVID-19 pandemic. We must recognize these struggles were born out of settler colonialism and learn this history while actively working to undo present harms.
Do not exclude Indigenous peoples in your research narratives. If you’re going to, acknowledge your limitations.
Dr. Neuner reminds us of the importance of centering Indigenous Peoples in our research and data because this information helps drive policy and health initiatives that can address barriers to health in the community.
Pearls
Common Terms Used to Refer to Indigenous Peoples
Our guests and hosts remind us of the importance of not making assumptions about someone’s identity. It is often preferable to use tribal affiliation when referring to Indigenous Peoples rather than terms like Indigenous or Native American. By not doing so, we obscure critical knowledge about relationality, Indigenous clans, and communal origins.
The term “American Indian or Alaska Native” is a legal racial and ethnic identifier which is why we might see it used in legal documents and research manuscripts. Many manuscripts have moved towards using Black, Indigenous, People of Color (BIPOC), but this term may be doing more harm than good for Indigenous Peoples. Read III.A.I-2 of Why BIPOC Fails (Deo, M., 2021) to understand why.
The term “Native American” is frequently used but does not cover Indigenous Peoples from across the world
The Burden of Proof
Dr. Sequist discusses “blood quantum”, which is an attempt by the federal government to reduce one’s identity as an Indigenous person to a percentage of blood affiliated with specific Tribes in the US. This flawed measure can be harmful for many reasons. It notably creates a burden of proof for Indigenous trainees to prove their identity, which can provide additional stress during application and interview cycles.
COVID-19 and Indigenous Peoples
Alec reminds us that Indigenous Peoples represent 6% of the global population across more than 70 countries, but around 15% of the global population experiencing poverty.
Many of the health inequities we have seen for Indian Country during COVID-19 are directly linked to settler colonialism. This is further exacerbated by poverty, lack of cell phone coverage, food insecurity, broadband internet, and a shortage of trusted messengers with appropriate training in Tribal communities.
Dr. Neuner reminds us that many Native communities live in multigenerational housing (over 65% of communities have elders living with them) which made it challenging to socially distance during the pandemic.
Data Genocide
Dr. Neuner reminds us about the importance of data for advocacy for Indigenous communities, especially during COVID-19. More background here from the Urban Indian Health Institute.
“Without data you can’t change anything.”
Some of the challenges with data collection discussed were:
Limited availability disaggregated data and how being listed as “other” on surveys leads to compounded distrust in medical systems
Limited accessibility to that data for Tribal communities being surveyed
Logistical challenges of collecting necessary data, including the training and funding of community members
Ways to Help Uplift Indigenous Peoples in Academia
Our guests share some ways we can help support and uplift Indigenous peoples:
Community-based participatory research that benefits Tribal communities in meaningful ways
Working towards making education free for Native students
Promoting Tribal sovereignty
Advocating for climate justice
Aligning institutional missions to support Indigenous peoples locally, nationally, and globally
Creating Supportive Spaces
Our guests remind us of the importance of thinking beyond addressing the “pipeline” to increase representation of Indigenous Peoples in medicine, but also emphasize the importance of creating safe spaces for these students to thrive.
This includes being mindful of language and the etiology of the words we use in academic and medical spaces (e.g., “low on the totem pole”, “let’s have a powwow”)
This also includes understanding the unique challenges Indigenous students face when away from their communities in predominantly white institutions, which can often affect their mental health and wellbeing.
Perspective by Dr. Tom Sequist “Paving the Way — Providing Opportunities for Native American Students” N Engl J Med 2005; 353:1884-1886. doi:10.1056/NEJMp058218
The hosts and guests report no relevant financial disclosures.
Citation
Sequist T, Neuner S, Calac A, Lopez-Carmen V, Tsai J, Krishnamurthy S, Ogunwole M, Fields NF, Nolen L, Onuoha C, Watkins A, Williams J, Paul D, Essien UR, Khazanchi R. “Episode 12: Our Land is Our Health: Addressing Anti-Indigenous Racism in Medicine.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. November 23, 2021.
Anisha B. Dua MD, MPH is an Associate Professor of Medicine in the Division of Rheumatology, Rheumatology Fellowship Program Director and Director of the Northwestern Vasculitis Center at Northwestern University Feinberg School of Medicine. Dr. Dua interests are in rheumatology, education, and vasculitis. She completed her Rheumatology fellowship at Rush University as well as fellowships in medical education at The University of Chicago and Integrative Medicine at Northwestern. She is a former member of the Committee on Training and Workforce for the American College of Rheumatology, worked with the ACGME to develop the new subspecialty milestones for Rheumatology, and is currently the Chair of the ACR In-Training-Exam committee. Dr. Dua currently leads a multidisciplinary team in the clinical management of vasculitis patients. She recently assisted in the development of the American College of Rheumatology (ACR) Guideline for the Treatment and Management of Vasculitis, is on the Board of Directors for the Vasculitis Foundation and a member of the Scientific Advisory Council for the Rheumatology Research Foundation. She has served in leadership capacities both locally and nationally through the American College of Rheumatology, the Vasculitis Foundation, and the ACGME in the areas of education as well as vasculitis. You can follow her on twitter @anisha_dua
Patreon exclusive: RLR 69 – Power of the frame
Nov 14, 2021
In the diagnostic journey, nothing is more important than the frame. The wrong frame leads to the wrong diagnosis. However, sometimes you need multiple frames with the flexibility to pivot from one frame to another like Lionel Messi and his left foot. Rabih shows us the power of the frame in this episode.
Happy Sunday!
And consider advertising RLR to a friend. We thank you.
Sharmin and Dr. Kaylin Nguyen delve deeper into the imposter phenomenon. They discuss the origin of the term, the problems with the mainstream definition, and how it should be reframed.
Dr. Kaylin Nguyen was born in Vietnam and grew up in Southern California. After graduating from UCLA, she completed both medical school and Internal Medicine residency at UCSF. She is currently a second year Cardiology fellow at Stanford and has interests in cardiovascular imaging, health disparities, and digital health. She enjoys hiking, drinking copious amounts of herbal tea, and well-timed puns.
Episode 205- Global VMR Special Episode – The Mock Interview – The Do’s and Don’ts with Dr. Ravi Singh – Part 2
Nov 04, 2021
Dr. Ravi Singh interviews CPSolvers team members Rafael Medina, Sukriti Banthiya, and Rabih Geha who illustrate the Do’s (Rafael and Sukriti) and Don’ts (Rabih) of a residency application interview. This is for anyone interviewing, but especially for IMGs.
Doctor Ravi Singh graduated from the University Medical School of Debrecen in Hungary. He did residency at the MedStar Health Internal Medicine Residency program in Baltimore, Maryland. He then moved to Sinai hospital/Johns Hopkins internal medicine residency program as an academic hospitalist. Dr Singh is currently an associate Program Director Internal Medicine Residency Program at Sinai Hospital, in Baltimore and also a clerkship site director at Sinai for Johns Hopkins School.
Episode 205- Global VMR Special Episode – The Mock Interview – The Do’s and Don’ts with Dr. Ravi Singh – Part 1
Nov 04, 2021
Dr. Ravi Singh interviews CPSolvers team members Rafael Medina, Sukriti Banthiya, and Rabih Geha who illustrate the Do’s (Rafael and Sukriti) and Don’ts (Rabih) of a residency application interview. This is for anyone interviewing, but especially for IMGs.
Doctor Ravi Singh graduated from the University Medical School of Debrecen in Hungary. He did residency at the MedStar Health Internal Medicine Residency program in Baltimore, Maryland. He then moved to Sinai hospital/Johns Hopkins internal medicine residency program as an academic hospitalist. Dr Singh is currently an associate Program Director Internal Medicine Residency Program at Sinai Hospital, in Baltimore and also a clerkship site director at Sinai for Johns Hopkins School.s
Patreon exclusive: RLR 67 – Not so fast
Nov 02, 2021
We hope you enjoy! And as always, thank you for your support. The RLR series is only possible because of you.
In this episode, Simone & Emma review the schemas of Altered Mental Status and Microangiopathic Hemolytic Anemia as they work through a case presented by Moses.
Lisa Sanders, MD, founder and writer of the popular Diagnosis column for New York Times Magazine, and Laura Glick, MD, STUMP RR through a very exciting case.
We hope you enjoy it as much as we enjoyed being stumped.
Join us on Patreon for more cases with Dr. Sanders, and 5 bonus episodes a month with RLR.
Episode 202: Global VMR Special Episode – Residency Applications for IMGs Part 2
Oct 19, 2021
CPSolvers team members–Rafael Medina (lead organizer),Valeria Roldán, Gabriel Talledo, and Andrea Guzman facilitate a conversation with Drs. Gallo and Singh who shared authentic, practical, and inspirational insight into the IMG journey to apply to residency in the USA.
Dr Alice Gallo
Doctor Alice Gallo graduated from the Medical School of the Pontifícia Universidade Católica do Rio Grande do Sul in Brazil. She did residency at the Hospital Nossa Senhora da Conceição, repeated it at the University of Miami Miller School/Jackson Memorial Hospital/VA Hospital. She did a Pulmonary and Critical Care Fellowship at Mayo Clinic in Rochester, and joined the Critical Care staff at Mayo in 2017. Dr. Gallo is an Associate Professor of Medicine and Associate Program Director for the Internal Medicine Residency Program Mayo Clinic in Rochester.
Dr Ravi Singh
Doctor Ravi Singh graduated from the University Medical School of Debrecen in Hungary. He did residency at the MedStar Health Internal Medicine Residency program in Baltimore, Maryland. He then moved to Sinai hospital/Johns Hopkins internal medicine residency program as an academic hospitalist. Dr Singh is currently an associate Program Director Internal Medicine Residency Program at Sinai Hospital, in Baltimore and also a clerkship site director at Sinai for Johns Hopkins School.
CPSolvers team members–Rafael Medina (lead organizer),Valeria Roldán, Gabriel Talledo, and Andrea Guzman facilitate a conversation with Drs. Gallo and Singh who shared authentic, practical, and inspirational insight into the IMG journey to apply to residency in the USA.
Dr Alice Gallo
Doctor Alice Gallo graduated from the Medical School of the Pontifícia Universidade Católica do Rio Grande do Sul in Brazil. She did residency at the Hospital Nossa Senhora da Conceição, repeated it at the University of Miami Miller School/Jackson Memorial Hospital/VA Hospital. She did a Pulmonary and Critical Care Fellowship at Mayo Clinic in Rochester, and joined the Critical Care staff at Mayo in 2017. Dr. Gallo is an Associate Professor of Medicine and Associate Program Director for the Internal Medicine Residency Program Mayo Clinic in Rochester.
Dr Ravi Singh
Doctor Ravi Singh graduated from the University Medical School of Debrecen in Hungary. He did residency at the MedStar Health Internal Medicine Residency program in Baltimore, Maryland. He then moved to Sinai hospital/Johns Hopkins internal medicine residency program as an academic hospitalist. Dr Singh is currently an associate Program Director Internal Medicine Residency Program at Sinai Hospital, in Baltimore and also a clerkship site director at Sinai for Johns Hopkins School.
Any topic in medicine is more enjoyable once you learn the topic. I did not have a systematic approach to ataxia one year ago and it was a tough day at work. I used that energy to create an approach with a dear friend.
We hope you are kind to yourselves and use such reminders as a stimulus to grow rather than defeat.
Episode 11: Racism, Redlining, and the Path Towards Reconciliation
Show Notes by Sud Krishnamurthy, Michelle Ogunwole, Chioma Onuoha
October 12th, 2021
Summary: This episode is part of a 3-part series on Race, Place, and Health. In this episode, we invite Mr. Richard Rothstein, distinguished Fellow of the Economic Policy Institute and acclaimed author of the book, The Color of Law: A Forgotten History of How Our Government Segregated America, and Professor Fernando De Maio, PhD director of research and data use at the AMA’s Center for Health Equity, professor of sociology at DePaul University, and co-editor of the recently published book, Unequal Cities: Structural Racism and the Death Gap in America’s Largest Cities, to share their expertise on structural racism, neighborhood segregation, and health inequities.
Episode Learning Objectives:
After listening to this episode learners will be able to…
Explain the differences between de jure and de facto segregation
Explore the historical and present-day implications of neighborhood redlining and housing segregation on health disparities
Explain the importance of precise definitions when discussing structural racism
Explore short and long term remedies to segregation
Credits
Written and produced by: Utibe R. Essien, MD, MPH, Jennifer Tsai MD, MEd, Rohan Khazanchi, MPH, Michelle Ogunwole, MD, Sudarshan Krishnamurthy, Naomi F. Fields, LaShyra Nolen, Chioma Onuoha, Dereck Paul, MD, MS, Ayana Watkins, Jazzmin Williams
Hosts: Utibe R. Essien, MD, MPH, Jennifer Tsai MD, MEd, Rohan Khazanchi, MPH
Infographic: Creative Edge Design
Audio edits: David Hu
Show notes: Sudarshan Krishnamurthy, Michelle Ogunwole, Chioma Onuoha
Guests: Richard Rothstein, Fernando De Maio, PhD
Time Stamps
00:00 Introduction
02:29 De Jure and De Facto Segregation: The Color of Law
06:45 Health Inequities and Segregation: Unequal Cities
12:07 Defining Structural Racism
18:05 Federal Policy and Suburbanization
24:50 The Racial Wealth Gap and its Consequences
30:27 The Role of Health Equity Promoting Policy
32:00 Potential Remedies for Past Harms
39:45 Segregation of Medical Care
41:20 What Can Listeners Do Going Forward?
Episode Takeaways:
1. Terminology and Definitions of de jure and de facto segregation: The myth that segregation in modern societies has to do with private activities (e.g individual bias or bigotry that leads to a failure to sell a home to a person of color) and personal choices ( e.g. Black people prefer to live among other Black people) is referred to as de facto segregation. Adopting this worldview removes any obligation to remedy the consequences of segregation. In contrast, de jure segregation refers to the involvement of federal, state, and local governments in creating, structuring, designing, reinforcing, and perpetuating segregation. This reality of de jure segregation helps us understand that we have an obligation to remedy this constitutional violation.
2. Segregation relates to crucial public health outcomes that ultimately have an effect on life expectancy: The average life expectancy across the United States is 78.6 years; however, there exists a 10 year gap in life expectancy among the 30 largest cities in the US, from 72.9 years in Baltimore to 82.9 years in San Francisco and San Jose. Across the country, we see a 4 year gap in life expectancy between Black and White Americans; and this gap between and Black and White individuals ranges from 12 years in Washington DC, more than 8 years in Chicago, to no gap in El Paso. These gaps are not a product of lifestyle choices, biology or individual behaviors. They are a product of deep-rooted man-made policies that extend to many sectors (healthcare, education, criminal justice etc). These policies have systematically disadvantaged some groups, and have advantaged others. These policies are woven deeply into the fabric of the United States, and are intimately related to residential segregation, life expectancy, and mortality.
3. Unconstitutional housing policy in the mid-20th century led to the present day wealth gap and has implications for disparities: Discriminatory policies prohibited African Americans from being homeowners, while allowing White Americans to purchase homes and accumulate generational wealth. These policies established the wealth gap between Black and White Americans that persists today. Nationally, African Americans’ income is 60% of that of White Americans. Although one would think this leads to a 60% wealth gap as well, household wealth of African Americans is 5% (95% wealth gap) of that of White Americans. This extreme disparity between the 60% income ratio and the 5% wealth ratio is attributable to consequences of federal housing policy practiced in the mid-20th century. You can draw a line from these discriminatory housing policies, to the wealth gap, to disparities in education, health, and police brutality.
Pearls
On the importance of considering place based inequities
Variability of health inequities between communities in a single city or across different cities is critical to consider when discussing health inequity.
“We tend to think of health inequities as big, monolithic, deeply entrenched patterns, and they are, but their variability is really important. It gives us a sense of how different things can be.”-Professor Fernando De Maio
On language and the use of the term ‘structural racism’
Structural racism is a word that is used often, however many people do not know what it really means. Professor DeMaio notes that confusion around terminology is not a reason to shy away from discussions around it. He declares that one of our greatest challenges, and also one of our obligations, is to address structural racism head on.
“It’s our collective responsibility to explain it, to define it, to communicate it in effective ways to physicians, to healthcare systems, to the public at large and in detail, with data and with narratives, all the ways through which racism impacts our health.” -Professor Fernando De Maio
On Remedies to segregation
Mr. Rothstein shares two examples of potential remedies to segregation. The first would specifically address the constitutional violation that prohibited African Americans from becoming homeowners. The remedy would be for the government to buy up homes at market value in neighborhoods where African Americans were not allowed to buy homes, and sell them back to qualified African American buyers at deeply discounted rates.
The second remedy would correct a policy– the low-income housing tax credit– that reinforces segregation. Currently, low-income housing tax credit is a federal program distributed to housing developers who build housing for low-income families. However, this program reinforces segregation as developers are more inclined to build low-income housing in low-income neighborhoods. This can be reversed by placing a priority on use of these tax credits in higher-opportunity communities and prohibiting the use of this credit for creating more segregated communities.
Mr. Rothstein notes that the challenge is not in thinking of ideas or potential remedies…
“ We know what the policies are to create equality, a more equal society and a non-segregated society. What’s missing is not policy ideas. What’s missing is a new civil rights movement that’s going to create the political environment where those policies have to be implemented.”-Mr. Richard Rothstein
On being a citizen and the collective effort needed to change the status quo
Mr. Rothstein leaves us with these wise words to consider as we head back into our professional roles in medicine.
“In addition to being a physician, you’re a citizen. And I think the most important thing you can do is align yourself with other citizens in whatever profession they are, because this is going to take a community effort” -Mr. Richard Rothstein
References
Rothstein, R. (2017). The Color of Law: A Forgotten History of How Our Government Segregated America.
Benjamins MR, De Maio F. Unequal Cities: Structural Racism and the Death Gap in America’s 30 Largest Cities. Baltimore: Johns Hopkins University Press; 2021.
De Maio F, Ansell D. “As Natural as the Air Around Us”: On the Origin and Development of the Concept of Structural Violence in Health Research. Int J Health Serv. 2018;48(4):749-759. doi:10.1177/0020731418792825
Benjamins MR, Silva A, Saiyed NS, De Maio FG. Comparison of All-Cause Mortality Rates and Inequities Between Black and White Populations Across the 30 Most Populous US Cities. JAMA Netw Open. 2021;4(1):e2032086. doi:10.1001/jamanetworkopen.2020.32086
Metzl JM, Maybank A, De Maio F. Responding to the COVID-19 Pandemic: The Need for a Structurally Competent Health Care System. JAMA. 2020;324(3):231-232. doi:10.1001/jama.2020.9289
Liao TF, De Maio F. Association of Social and Economic Inequality With Coronavirus Disease 2019 Incidence and Mortality Across US Counties. JAMA Netw Open. 2021;4(1):e2034578. doi:10.1001/jamanetworkopen.2020.34578
Krieger M, Boyd R, De Maio F, Maybank A. “Medicine’s Privileged Gatekeepers: Producing Harmful Ignorance About Racism And Health, ” Health Affairs Blog, April 20, 2021. doi: 10.1377/hblog20210415.305480
Wilkinson RG. Unhealthy Societies: The Afflictions of Inequality. London: Routledge; 2005.
Metzl JM, Hansen H. Structural competency: theorizing a new medical engagement with stigma and inequality. Soc Sci Med. 2014;103:126-133. doi:10.1016/j.socscimed.2013.06.032
The “Redress Project,”, i.e. the New Movement to Redress Racial Segregation, will launch early next year. For anyone who wants to receive more information about the launch of the New Movement to Redress Racial Segregation, please click here NMRRS.
The hosts and guests report no relevant financial disclosures.
Citation
De Maio F, Rothstein R, Khazanchi R, Tsai J, Krishnamurthy S, Ogunwole M, Fields NF, Nolen L, Onuoha C, Watkins A, Williams J, Paul D, Essien UR. “Episode 11: Racism, Redlining, and the Path Towards Reconciliation.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. October 12, 2021.
We continue our campaign to #EndNeurophobia, with the help of Dr. Aaron Berkowitz. This time, Gabriela presents a case of impairment of speech to Gabriel and Valeria.
Gabriela has graduated from Medical School at Unicamp and recently finished her neurology residency at Unesp, both in Brazil. She is interested in Medical Education and Clinical Reasoning and has obviously fallen in love with CPSolvers and VMRs since day 1. In her free time, she likes to practice pilates, play with her dogs, binge-watch Netflix comedy series, read biography books, go out with her friends (pre-COVID), drink wine, and cook (still learning).
Gabriel Talledo
Gabriel is a MS2 student from Cayetano Heredia University. When it comes to medicine, he enjoys dermatology, infectiology, and LGBTQ+ health. He fell in love with his career when he understood medicine not just as a concept of knowledge but a combination of knowledge and social justice pursuit. He loves cooking Peruvian cuisine (one of the best in the world), eating, jogging and watching TV series. Recently he is doing a transgender education program at his university and a volunteering of sexual education in Lima schools.
Valeria Roldan
Valeria is a medical student at Universidad Peruana Cayetano Heredia. She was born and lives in Lima, Perú. She hopes to pursue Neurology residency. Her interests include neuro-infectious diseases, transgender health and medical education. Her work with CPSolvers involves being a part of the Virtual Morning Report team and serving on the Spanish schemas team. Outside of Medicine she loves running, hiking, cooking pasta and spending time with her dogs.
On this episode, Rabih presents two cases at once for Reza.
We truly hope you enjoy these cases.
If you are not driving or doing an activity that needs your full attention, pause after each aliquot and share your thoughts out loud. Then compare your thoughts to RR’s thoughts. Think like no one is watching and get better one rep at a time!
Thank you as always.
RR
Episode 198: HumanDx Unknown with Laura, Stef, and Jack – hematochezia and abdominal pain
Sep 22, 2021
Alec presents a case of abdominal pain and hematochezia to Laura, Stef, and Jack.
Laura Geiszler
Laura Geiszler is a third-year Internal Medicine resident at Lankenau Medical Center in Wynnewood, Pennsylvania.
Laura completed her medical school at Philadelphia College of Osteopathic Medicine. She has a passion for humanizing medicine and promoting health and wellness to prevent disease.
Outside of work she is a proud cat mom, fitness lover, fiction book enthusiast, and fashion addict.
Stefanie Gallagher
Stefanie is a PGY-3 internal medicine resident at Lankenau Medical Center, located in Wynnewood, PA.
She earned her medical degree from the Philadelphia College of Osteopathic Medicine, with a dual-degree in Bioethics from the University of Pennsylvania.
She is an aspiring gastroenterologist and has a passion for disorders of the gut-brain axis.
Outside of medicine, she enjoys her English bulldog (Boomer), cycling, and reading non-fiction.
Alec Rezigh
Alec Rezigh is an academic hospitalist at Baylor College of Medicine in Houston, TX.
He completed medical school at McGovern Medical School in Houston and his residency at The University of Colorado.
His clinical interests include medical education and clinical reasoning.
He loves all things basketball, CPSolvers, and playing with his human and doggy daughters.
Dr. Titer, Dr. Williams, Maani and Lindsey discuss macro/microaggressions in the clinical setting.
Dr. KeAndrea Titer
Dr. KeAndrea Titer is an Assistant Professor in the Division of General Internal Medicine at University of Alabama at Birmingham. She was born and raised in Tampa, Florida. She received her Bachelor of Science in Biology from Oakwood University in Huntsville, Alabama. She went on to earn her medical degree from Loma Linda University School of Medicine in Loma Linda, California. She completed her residency and chief residency at the University of Alabama at Birmingham Tinsley Harrison Internal Medicine Residency Program. Her academic interests include physical exam-focused medical education where she co-directs the Enhanced Clinical Skills Residency Track and serves as Investigator for the AMA Reimagining Residency Grant awarded to John Hopkins, Stanford, and UAB focused on studying clinical skills as it relates to resident wellness. She is also passionate about diversity, equity, and inclusion and serves as the Assistant Director of Diversity and Inclusion for the Tinsley Harrison Internal Medicine Residency Program where she works to design initiatives and curriculum focused on recruitment, education, and building community.
Dr. Karla Williams
Dr. Karla Williams is an assistant professor in the Division of General Internal Medicine and Hospital Medicine at UAB in Birmingham, AL. She serves as an assistant program director and the director of diversity and inclusion for the Tinsley Harrison Internal Medicine Residency Program. She has a passion for advancing diversity, equity and inclusion in graduate medical education and care delivery and was recognized as a recipient of the 2020 Dean’s Excellence Award in Diversity. She has recently worked with colleagues to develop a formal curriculum, Supporting Trainees by Addressing Inappropriate Behaviors by Patients, to address microaggressions and other inappropriate behaviors in the medical environment. This initiative has created a platform to have safe and honest discussions about the presence and effect of bias, including racial and gender derogations, in the medical environment and has been presented and implemented at numerous academic institutions at the UME and GME levels. The ultimate goal is to bring awareness to our implicit and explicit biases in an effort to cultivated more inclusive learning and clinical environments for trainees, faculty and patients.
Patreon exclusive: RLR 62 – Lisa Sanders, MD, presents a case to R&R
Sep 13, 2021
Lisa Sanders, MD, founder and writer of the popular Diagnosis column for New York Times Magazine, and Laura Glick, MD, STUMP RR through a very exciting case.
We hope you enjoy it as much as we enjoyed being stumped. There will be exclusive schema(s) and/or illness script(s) with this episode for tier 2 and tier 3 Patrons. We thank you for your continued support.
RLR are back on the podcast with a fascinating case. Over the summer, they’ve been releasing a lot of cool content on Patreon. Check it out here for much more RLR content.
Gabriela has graduated from Medical School at Unicamp and recently finished her neurology residency at Unesp, both in Brazil. She is interested in Medical Education and Clinical Reasoning and has obviously fallen in love with CPSolvers and VMRs since day 1. In her free time, she likes to practice pilates, play with her dogs, binge-watch Netflix comedy series, read biography books, go out with her friends (pre-COVID), drink wine, and cook (still learning).
Maria Jimena Aleman
Maria Jimena Aleman was born and raised in Guatemala where she currently is a medical student in Universidad Francisco Marroquin. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She also looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Louis Armstrong. Outside of medicine she enjoys modern art, 21st century literature and having hour long conversations over a nice hot cup of coffee or tequila.
Kirtan Patolia
Kirtan is a final year medical student from B.J. Medical College, Ahmedabad, Gujarat, India. He is looking forward to joining Internal Medicine Residency in the USA by applying through this year’s Match Cycle.
He loves to solve clinical cases and was delighted when he got the opportunity to join the CPSolvers team. He is so grateful to Dr. Geha and Dr. Manesh for this opportunity. Clinical reasoning is his biggest passion and he strives to enhance his diagnostic skills every day. Discussing and sharing clinical cases with his friends gives him distinct pleasure. Outside of medicine, I like to read Agatha Christie and Nancy Drew novels. He also loves kite-flying, as he finds the various techniques and maneuvers to fly kites fascinating.
Patreon exclusive: RLR 55 – Headache + Support Rabih’s Internet Bill
Aug 10, 2021
Dr. Marion Stanley is a hospitalist and an internal medicine residency associate program director at Northwestern Memorial Hospital. She completed medical school at University of Chicago, Pritzker School of Medicine and graduated from University of California, San Francisco for residency. She spends her clinical time on the general medicine teaching services as well as the general medicine and oncology hospitalist units. She enjoys spending time with her husband and two daughters, ages 4 and 1.
Dr. Geralyn Palmer
Dr. Geralyn Palmer is a first year internal medicine resident at the University of Wisconsin. She completed her undergraduate and medical education in her home state of South Dakota. After residency, Geralyn hopes to pursue a career in medical education, and is currently considering a broad specialty differential. In her free time she enjoys long walks outside (preferably with dogs), experimenting in the kitchen, and The Great British Bake Off.
Dr. Julia Armendariz presents a clinical unknown to Dr. Laura Huppert.
Dr Laura Huppert
Laura Huppert, MD, is a third year Hematology/Oncology Fellow at the University of California, San Francisco (UCSF). Her clinical interest is in solid tumor malignancy, including the treatment of breast cancer and melanoma. She is also interested in medical education, and recently published a handbook for internal medicine entitled “Huppert’s Notes”, published by McGraw Hill. Dr. Huppert earned her M.D. from Harvard Medical School. She completed her Internal Medicine Residency and Chief Residency at UCSF.
Dr. Julia Armendariz
Julia Armendariz, MD is a general medicine hospitalist. Her interests lie in medical education, trainee wellness, and effective communication. She is a faculty member of the Stanford Internal Medicine Residency Wellness Committee and the Stanford GME Women in Medicine group. Dr. Armendariz earned her M.D. from Oregon Health and Science University in Portland, OR and completed her Internal Medicine Residency at Stanford.
Shanthi presents a clinical unknown to Sam, Michael, and Jack.
Want to test your learning? Take our episode quiz here
Michael Vu
Michael Vu is a second year Internal Medicine resident at Methodist Dallas. He completed his undergraduate education at the University of Texas at Dallas and his medical training at the University of North Texas Health Science Center – Texas College of Osteopathic Medicine. His current career interests include clinical reasoning, medical education, and cardiology. In his free time, he enjoys working out, cooking, and spending time with his wife.
Samantha Etienne
Sam is a PGY3 and chief resident at Methodist Dallas Medical Center in Dallas, TX. She attended the University of Texas Medical Branch at Galveston and is an aspiring hematologist/oncologist. Outside of medicine, she enjoys spending quality time with friends and family and has a real passion for food. She is considered by many a connoisseur of tacos.
Shanthi Kappagoda
Shanthi Kappagoda was born in United Kingdom and grew up in the UK and Canada. She graduated from UC Davis School of Medicine and completed her internal medicine residency at Brigham and Women’s Hospital in Boston. She completed her Infectious Disease fellowship at the Stanford School of Medicine and after fellowship remained at Stanford as a clinical faculty member. She works primarily on the ICU-ID consult service. In her free time, she enjoys spending time with her two children, growing vegetables and hiking around California State parks.
In this episode, we invite the powerful sister duo Oni Blackstock, MD, MHS and Uché Blackstock, MD to share their experiences on leaving public health and academia to become social entrepreneurs, creating their own organizations in health equity.
Episode Learning Objectives
After listening to this episode learners will be able to…
Recognize some common factors that influence Black women’s decisions to leave traditional health careers
Define counterspaces and understand their value
Apply tools to combat burnout that could be applied to traditional or alternative health careers
Credits
Written and produced by: Michelle Ogunwole, MD, Naomi F. Fields, LaShyra Nolen, Chioma Onuoha, Rohan Khazanchi, MPH, Dereck Paul, MD MS, Utibe R. Essien, MD, MPH, Jazzmin Williams, and Jennifer Tsai MD, M.Ed
Hosts: Michelle Ogunwole, MD, Naomi Fields, and LaShyra Nolen
Infographic: Creative Edge Design
Audio edits: David Hu
Guests: Oni Blackstock, MD, MHS and Uché Blackstock, MD
Time Stamps
00:00 Introduction
03:49 Defining “CounterSpaces”
5:22 Why Drs. Uché and Oni Blackstock created their counterspaces
17:54 Value gained outside of academia, public health
24:08 Finding balance in racial equity opportunities
34:17 On challenging the self-sacrificing mentality in medicine
42:26 On “doing the work” within academia
49:01 The meaning of sisterhood
52:20 Closing Remarks
Episode Takeaways:
Definition of CounterSpaces: CounterSpaces are academic and social safe spaces that allow underrepresented faculty to promote their own learning, wherein their experiences are validated and viewed as critical knowledge; they have space to vent frustrations by sharing stories of isolation, microaggressions or overt discrimination; and they can challenge the deficit notion of people of color and establish and maintain a positive collegial racial climate for themselves.
Root causes of the exodus Black women physicians from academia and public health: In many academic and public health institutions, Black women feel undervalued, untitled, underfunded, and undersupported. Their contributions to diversity, equity, and inclusion efforts are expected, but not compensated or rewarded. They are disproportionately passed over for promotions and opportunities despite quality work. These factors directly contribute to the growing trend of Black women physicians leaving these fields to pursue nontraditional health careers.
You are gifted!: “Sometimes you’re in these environments [academic, public health] for so long where you’re undervalued and underappreciated, you’re not supported the way that you should be, that you actually start thinking that– or start forgetting that you’re actually someone with gifts to share.” — Dr. Uché Blackstock
Self-sacrifice is not the highest virtue: Medicine is its own subculture where people are expected to make sacrifices of their time, personal and family life, and finances in order to demonstrate that they are good physicians. It is okay to say that you don’t want that for yourself, and work to actively counter this cultural norm in order to live a fulfilling personal and professional life.
There are opportunities to advance racial equity inside and outside of academia: For those who feel driven to pursue racial and health equity work within academia and/or public health: (1) understand what you value from working at an academic institution and recognize that there may be options to do that work outside of academia (e.g. research), and (2) build a support structure that enables you to stay true to your values as you work to create change from within.
For those having a hard time deciding if they should stay in academia or other traditional research or public health roles, Dr. Oni Blackstock offers important advice about listening to and trusting oneself:
“… just listening to your intuition, that’s like our main form of knowing. We have all these other forms of knowledge in books and what we’re taught in school, but really many times, the answer lies within us. So, again, just making sure that we’re in tune and listening to what we feel like our needs are. And if they’re telling us to leave, that we are true to those voices and we leave. And if they’re saying there’s work for us to do here, we want to stay and we have the support to be able to do that, then do that.” — Dr. Oni Blackstock
Pearls
“The work of liberation is the work of freeing the soul to be exactly who we were meant to be.” — GirlTrek
The role of an abundance mindset in achieving work/life balance
Many of us operate from a scarcity mindset; we feel that opportunities are limited and therefore take all opportunities that come our way without regard for our genuine interest in the opportunity or our true time availability. Especially for people early in their careers, there is an unspoken pressure to accept all opportunities that could possibly advance one’s career. It is impossible to achieve work/life balance when operating from this mindset, and as a consequence, it leads to burnout.
However, with an abundance mindset, one recognizes that opportunities are not finite and that saying no to one opportunity frees up our ability to say yes to a better opportunity that comes along later down the line. Dr. Uché Blackstock shared an example of how she experienced a tension between a scarcity mindset and an abundance mindset when deciding whether to continue part-time clinical work or to devote full-time effort to the organization she founded. When she embodied an abundance mindset and let go of her clinical career, she was free to say yes to even more fulfilling opportunities that came her way.
Relatedly, Dr. Oni Blackstock discussed the importance of pausing before committing to opportunities. White supremacy culture creates an artificial sense of urgency so we often respond reflexively. By taking a moment to pause and reflect, one can take on opportunities that align with one’s values and that one has adequate time for without sacrificing personal responsibilities. Taking a moment to pause ensures that we react from our authentic self and not from institutional culture.
Cultivate tools to sustain a career in traditional and alternative health careers
Cultural norms rooted in white supremacy and capitalism create an environment that extracts goods, time, and energy from people without providing a source from which to renew those resources. Dr. Oni Blackstock advises listeners to be “cognizant of the day to day ways in which these systems work against us,” and to actively fight against this culture with things that replenish ourselves. Tools that Dr. Oni Blackstock uses include: daily meditation, creating a gratitude list of 3 things each morning, and yoga and exercise several times a week. Additionally, she spoke about the importance of mentorship and a strong support network so you have people to turn to for advice and encouragement.
Finding effective strategies to replenish oneself is important for anyone advancing racial equity work in their careers as social entrepreneurs, academicians, public health officials.
Dr. Oni Blackstock shared a treasured quote around this idea: “ Learn to drink as you pour, so the spiritual heart cannot run dry and you always have love to give”-Ma Jaya
Self-reflection is a vital component of professional development
It is easy to become consumed by various career opportunities that are presented to us. In order to maintain one’s ability to effectively transform the existing culture of medicine into an anti-racist one, it is important to find time to reflect on one’s journey and direction. Below are some questions that CPSolvers ARM host Dr. Michelle Ogunwole synthesized after this conversation with Drs. Oni and Uché Blackstock.
What are the things (situations, contexts, people) that are making you question your gifts?
What are the wake up calls that we need in our life? How can they help you in your next step?
Who are you taking advice from?
What is keeping you from being your authentic self?
References
National Academies of Sciences, Engineering, and Medicine 2020. Promising Practices for Addressing the Underrepresentation of Women in Science, Engineering, and Medicine: Opening Doors. Washington, DC: The National Academies Press. https://doi.org/10.17226/25585.
National Academies of Sciences, Engineering, and Medicine 2021. Impact of COVID-19 on the Careers of Women in Academic Sciences, Engineering, and Medicine. Washington, DC: The National Academies Press. https://doi.org/10.17226/26061.
Doll KM, Thomas CR Jr. Structural Solutions for the Rarest of the Rare – Underrepresented-Minority Faculty in Medical Subspecialties. N Engl J Med. 2020;383(3):283-285. https://www.nejm.org/doi/full/10.1056/NEJMms2003544
The hosts and guests report no relevant financial disclosures.
Citation
Blackstock O, Blackstock U, Ogunwole M, Fields NF, Nolen L, Onuoha C, Williams J, Tsai J, Essien UR, Paul D, Khazanchi R. “Episode 10: CounterSpaces in Medicine: Finding Safe Spaces and Redefining Value.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. July 15, 2021.
Dr. Frederick Weber is a Clinical Professor of Medicine at the University of Alabama Birmingham in the Division of Gastroenterology and Hepatology. He is the former Medical Director of the Division.
Want to test your learning? Take our episode quiz here
Gabriela Pucci
Gabriela has graduated from Medical School at Unicamp and recently finished her neurology residency at Unesp, both in Brazil. She is interested in Medical Education and Clinical Reasoning and has obviously fallen in love with CPSolvers and VMRs since day 1. In her free time, she likes to practice pilates, play with her dogs, binge-watch Netflix comedy series, read biography books, go out with her friends (pre-COVID), drink wine, and cook (still learning).
Kirsten Austad MD, MPH is an Assistant Professor of Family Medicine at Boston University School of Medicine and a hospitalist at Boston Medical Center. She earned her undergraduate degree in English Literature and Medical Microbiology and Immunology from the University of Wisconsin-Madison and her medical degree from Harvard Medical School in the New Pathway Program. She completed her residency in Family Medicine at Boston Medical Center, the largest safety-net hospital in New England. Following residency, she completed a research fellowship at Brigham and Women’s Hospital in Global Women’s Health and earned a Masters in Public Health from the Harvard T.H. Chan School of Public Health. During this time she worked clinically as a nocturnist at Brigham and Women’s Hospital / Dana Farber Cancer Institute. After fellowship she returned to Boston Medical Center where she is a hospitalist and the Medical Director of the HealthNet Inpatient Family Medicine service, one of the largest family medicine hospitalist services in the country.
Her research focuses on global implementation science aimed at improving the delivery of women’s health care in low-resource settings, including respectful maternity care and family planning. In addition to global health research, she also has extensive experience in program development, having spent 6 years as the Director of Women’s Health for Maya Health Alliance, a non-profit providing care to indigenous Maya patients in the highlights of Guatemala, where she trained and supervised a team of over 20 nurses and doctors to provide community-based patient-centered women’s health care.
Mohit is a current Chief Resident in the Department of Internal Medicine at WashU. He is from Huntington, West Virginia and attended Marshall University School of Medicine in his hometown. He loves clinical reasoning and has a special interest in Hospital Medicine. Outside of work, he enjoys cooking new recipes, hiking, walks in the park, and has recently developed a green thumb with over 30 house plants and a garden.
Kai Jones
Kai Jones is from Tulsa, Oklahoma and studied Biology and Anthropology at Washington University in St. Louis. She attended Washington University for medical school and is now a second-year resident in Internal Medicine at Barnes-Jewish Hospital. She is interested in Endocrinology, and community based participatory research. Her hobbies include golf, and cooking.
Bronson Knuzler
Bronson Kunzler was born and raised in Salt Lake City, Utah, he studied finance at Utah State University and is currently an MS3 at Penn State University College of Medicine. He is interested in Internal Medicine with hopes to become a Cardiologist. In his free time he enjoys cheering for the Utah Jazz, barbeque, and visiting museums.
Nicholas Hornstein is a PGY-3 at UCLA Ronald Reagan Medical Center. He was born and raised in Los Angeles, earned his undergraduate degree from Brandeis University, and graduated from Columbia University with an MD and a PhD in Computational Biology. He has a passion for climbing, cooking, furry animals, and the advancement of medical genomics/technology. He will be furthering his education next year with a Fellowship in Hematology Oncology at MD Anderson Cancer Center and couldn’t be more excited.
Suellen Li
Suellen Li is a PGY-2 internal medicine resident at Massachusetts General Hospital. She grew up in Roanoke, VA and attended Duke University, where she studied Environmental Sciences & Policy and Global Health. She then moved to Chicago to complete medical school at the University of Chicago Pritzker School of Medicine. After finishing residency, she hopes to pursue a career in hospital medicine. In her free time, she enjoys reading, eating chips and being a cat mom.
Jennifer Plotkin
Jennifer Plotkin is a PGY2 in internal medicine at UCLA. She was born and raised in Los Angeles. She attended MIT for undergrad where she majored in Chemistry. She completed her medical school training at Johns Hopkins. She loves internal medicine for its problem solving and meaningful therapeutic relationships with patients. Her interests include primary care, endocrinology, and medical education, particularly in the veteran population. Outside of medicine, she enjoys running, rooting for the Lakers and Dodgers, and exploring restaurants.
In this special episode of the Antiracism in Medicine Series, originally recorded for the 2021 Society of General Internal Medicine Annual Meeting, the CPSolvers Antiracism team discusses what must be done to make medical education more antiracist. The conversation spans stages of academic medical career progression, ranging from recruitment to training to retention. The ARM team draws upon their own research and personal experiences to provide listeners with recommendations and actionable next steps.
Learning Objectives
After listening to this episode, listeners will be able to…
Explore the common barriers to entering the medical profession that minoritized trainees face and discuss strategies that trainees and institutions can adopt to overcome them.
Recognize how racist ideologies are often perpetuated in medical education and ways that academic medical centers can revise their curricula to prepare a physician workforce that is invested in recognizing and addressing the root cause of health disparities.
Understand the “minority tax” that minoritized trainees and faculty experience in diversity, equity, and inclusion reform efforts; identify models to properly compensate individuals for their time and expertise.
Credits
Written and produced by: Dereck Paul, MD, MS; Chioma Onuoha, Utibe R. Essien, MD, MPH; Rohan Khazanchi, MPH; LaShyra Nolen; Naomi F. Fields; Michelle Ogunwole, MD; Jazzmin Williams; and Jennifer Tsai MD, M.Ed
Host: Chioma Onuoha
Infographic: Creative Edge Design
Guests: Rohan Khazanchi, MPH; Naomi F. Fields; Michelle Ogunwole, MD; Utibe R. Essien, MD, MPH; Jazzmin Williams
Timestamps:
00:00 Introduction
02:15 Barriers to Entry in Medicine
05:15 How to Identify an Uplifting Institutional Home
11:40 Racism Ingrained in Medical Education
15:10 Imagining an Ideal Medical School Curriculum
17:40 A Roadmap to Engaging Hyperlocal Communities in Medical Education
20:30 Moving Beyond Ahistorical Conversations about Health Disparities
27:05 Engaging All Learners as Stakeholders for Health Equity and Antiracism
33:40 Re-examining Who the Experts Are
42:40 Recognizing Privilege and Positionality
45:25 Patient Safety Analogy and “Racism Saps the Strength of the Whole”
49:44 Where Do You Find Your Hope?
Takeaways:
Reimagining the learning environment: Creating a more antiracist learning environment will require institution-level commitments and broader reforms in the medical education regulatory environment (i.e. board examinations and mandated competencies).
Valuing health equity work: antiracism and health equity work must be properly compensated at all levels of training. Such compensation could be monetary or come in the form of academic currency, like co-authorship of publications.
How to be a good ally and co-conspirator: Power and access are needed to sustain and amplify antiracist justice within medicine. Many times, granting this power and access will require that individuals with privileged identities historically possessing a disproportionate amount of power transfer that power to individuals from marginalized backgrounds. Rather than centering the importance of individual advancement, we can remember that whenever racism is operational, as Dr. Camara Jones says, it “saps the strength of the whole society.” Using justice to guide our distribution of power will improve everyone’s livelihood.
Advancing beyond ahistorical teaching on racial health disparities: Health equity education must include racism as a driver of health inequities. As prior podcast episodes have highlighted, misleading theories of racialized biological differences cannot be presented as the cause of racial health disparities.
Pearls:
Acculturation to Medical Education
While the process of medical education is exciting, progressing through clinical training involves acculturation for all. This acculturation can differentially affect learners based on their own backgrounds and experiences. It is important for learners to reach out to mentors and peers who can offer insight into learning the ropes, and a safe place to land; it is also important for educators to recognize this and offer this to their learners. Additionally, it is important that institutions create environments where students have educators and faculty of similar backgrounds as theirs to learn from.
For trainees: What to consider when evaluating medical schools and residency programs
It can be challenging for students and residents to decide if an institution is truly committed to antiracism, social justice and equity. While time and action are true measures of this commitment, some things to consider include:
Is there diversity, which is more than skin deep, in the leadership?
Does the institution involve community members in training?
What is the relationship between community members and the academic medical center?
How does the institution respond to issues of injustice that affect trainees?
Is advocacy celebrated or at least respected and encouraged?
Does the institution recognize past historical transgressions? What have they done to address a painful history if one exists?
Does the curriculum equip learners with a vocabulary to discuss racism?
Does the curriculum include historical context about the communities served by the academic medical center?
Engaging All Students as Stakeholders
Antiracism education can seem relegated to students with niche interests. Nevertheless, there are ways to engage all students as stakeholders.
Board exam writers can shape their learning objectives toward antiracism based on our evolving knowledge base and more accurate paradigms of racism-as-the-risk factor, given that board exams shape what educators include in their curricula.
On an institutional level, we can incentivize scientifically accurate, ethically responsible, justice-based means of representing and incorporating race, racism, and health equity within faculty members’ work. These are the people that learners often look up to and after whom they model their careers.
Finally, we might eschew the idea that learners are disinterested in these topics, and commit to deep education regarding race/racism in medicine. Learners are often intellectually curious with a heart to learn what is needed to provide the best care for their patients.
Curricular Reforms to Operationalize Antiracism
Curricula seeking to address health inequities cannot be ahistorical. Health disparities are not created in a vacuum; thus, discussion of disparate outcomes should include conversations about the systemic and structural underpinnings of inequity.
Similarly, medical curricula must become comfortable reframing who the “experts” are on health disparities topics. In brief, community stakeholders are crucial experts on the lived experiences and health of their neighbors. Community engagement, as well as prioritization of hyperlocal issues impacting communities proximate to academic institutions, can and should be integrated in health equity curricula.
References:
Amutah C, Greenidge K, Mante A et al. Misrepresenting Race — The Role of Medical Schools in Propagating Physician Bias. New England Journal of Medicine. 2021;384(9):872-878. doi:10.1056/nejmms2025768
Nolen L. How Medical Education Is Missing the Bull’s-eye. New England Journal of Medicine. 2020;382(26):2489-2491. doi:10.1056/nejmp1915891
Sharma M, Pinto A, Kumagai A. Teaching the Social Determinants of Health. Academic Medicine. 2018;93(1):25-30. doi:10.1097/acm.0000000000001689
Phelan S, Burke S, Cunningham B et al. The Effects of Racism in Medical Education on Students’ Decisions to Practice in Underserved or Minority Communities. Academic Medicine. 2019;94(8):1178-1189. doi:10.1097/acm.0000000000002719
Khazanchi R, Keeler H, Marcelin J. Out of the Ivory Tower: Successes From a Community-Engaged Structural Competency Curriculum. Academic Medicine. 2021;96(4):482-482. doi:10.1097/acm.0000000000003927
Tsai J, Ucik L, Baldwin N, Hasslinger C, George P. Race Matters? Examining and Rethinking Race Portrayal in Preclinical Medical Education. Academic Medicine. 2016;91(7):916-920. doi:10.1097/acm.0000000000001232
Jones C. Toward the Science and Practice of Antiracism: Launching a National Campaign Against Racism. Ethn Dis. 2018;28(Supp 1):231. doi:10.18865/ed.28.s1.231
Tsai J, Lindo E, Bridges K. Seeing the Window, Finding the Spider: Applying Critical Race Theory to Medical Education (MedCRT) to Make Up Where Biomedical Models and Social Determinants of Health Curricula Fall Short. Front Public Health. 2021. doi: 10.3389/fpubh.2021.653643
Mr. Khazanchi is a member of the American Medical Association’s Council on Medical Education, but the views presented herein represent his own and not necessarily those of the AMA or the Council. The hosts and guests report no other relevant financial disclosures.
Citation
Onuoha C, Khazanchi R, Fields N, Ogunwole M, Williams J, Essien UR, Tsai J, Nolen L, Paul D. “Episode 9: Moving Towards Antiracism in Medical Education.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. June 10, 2021.
Episode 180: Clinical Unknown – Global VMR
Jun 03, 2021
Want to test your learning? Take our episode quiz here
Dr. Hernán Carrillo
Hernán Carrillo is Head of the Internal Medicine Department at Las Higueras Hospital in Talcahuano, Chile. He’s also an Assistant Professor at Concepción’s University. He is passionate about his work in public health care and is specially crazy about diagnostic process. Loves to play guitar and singing, and he’s learning a little bit of piano. Also enjoys photography. He is totally in love with his family!
Description: We continue our campaign to #EndNeurophobia led by Aaron Berkowitz! This time, Doug presents a case of headache and blurry vision to Hannah and Dhruv.
Dhruv Srinivasachar is a soon-to-be 1st year Medicine-Pediatrics resident at Western Michigan University and a graduate of Virginia Commonwealth University School of Medicine (the Medical College of Virginia for all the veteran attendings out there). Introduced to medicine through research, Dhruv has shifted his passions to empathetic clinical care and medical education, as a contributor to the CPSolvers (especially through VMR as a case presenter, discussant, and compiler of cases) and team member for the Not Just Little Adults podcast (CPedsSolvers, if you will). When he’s not looking for apartments or stressing about intern year, he can be found biking, gardening, and cooking.
Hannah Roberts
Hannah is currently finishing medical school in Arizona with plans for emergency medicine. She graduated from the US Naval Academy and completed active duty before starting med school. Her interests in medicine include nuclear weapons safety, medical education, and clinical applications of evolutionary biology. Outside of medicine she is a dog person and loves being outside mountain biking, running, and camping.
Doug Pet
Doug Pet is a resident in neurology at UCSF. He grew up surrounded by cow farms and crab-apple trees in New Milford, CT. He completed a dual-degree program at Tufts and the New England Conservatory studying medical anthropology, community health, and jazz saxophone. He later worked for a non-profit in Berkeley, CA on bioethical and social justice issues related to genetic and reproductive technologies. Doug attended Vanderbilt University School of Medicine, after which he returned to the Bay Area for neurology residency at UCSF. He loves Brazilian music, playing Spike ball, and making custom wooden pens on his lathe.
Dr. Katrina Armstrong and Dr. Vineet Arora join the #bosslady Wdx team to discuss navigating negotiations as women in medicine
Dr. Katrina Armstrong
Dr. Katrina Armstrong is the Jackson Professor of Clinical Medicine at Harvard Medical School, Chair of the Department of Medicine and Physician-in-Chief of Massachusetts General Hospital. She is an internationally recognized investigator in medical decision making, quality of care, and cancer prevention and outcomes, an award winning teacher, and a practicing primary care physician. She has served on multiple advisory panels for academic and federal organizations and has been elected to the American Society of Clinical Investigation and the Institute of Medicine. Prior to coming to Mass General, she was the Chief of the Division of General Internal Medicine of the Robert Wood Johnson Clinical Scholars Program at the University of Pennsylvania.
Dr. Vineet Arora
Vineet Arora, MD, MAPP is an academic hospitalist and Associate Chief Medical Officer for Clinical Learning Environment and Assistant Dean for Scholarship & Discovery at the University of Chicago. Through her role, she bridges educational and hospital leadership to engage frontline staff into the institutional quality, safety, and value mission. An accomplished researcher, she is PI of numerous NIH grants to evaluate novel interventions that combine systems change with learning theory to improve care which has resulted in publications that have been cited over 11,000 times. She is an elected member of the National Academy of Medicine and the American Society of Clinical Investigation. As an advocate for women in medicine, she was featured in the New York Times for an editorial that called to end the gender pay gap in medicine. She is a founding member of the 501c3 Women of Impact dedicated to advancing women leaders in healthcare. She is on the leadership group of the National Academy of Science Engineering and Medicine’s Action Collaborative to End Sexual Harassment in Higher Education.
“There’s nothing new under the sun, but there are new suns” – Octavia E. Butler
Summary: We invite social justice champion and acclaimed scholar of race, gender, and the law, Dorothy E. Roberts, JD, to discuss the history of race-based medicine and the movement for health equity and justice.
Episode Learning Objectives
After listening to this episode learners will be able to…
Understand race as a social construct and political invention
Explore the history of race as a proxy for genetics and ancestry
Explore the history of race-based pharmaceuticals
Explore the history of race-based clinical algorithms
Credits
Written and produced by: Naomi Fields, Rohan Khazanchi, LaShyra Nolen, Michelle Ogunwole, MD, Chioma Onuoha, Jenny Tsai, MD, Jazzmin Williams, Dereck Paul, MS, and Utibe R. Essien, MD, MPH
13:40 Responses to Common Race Based Medicine Arguments
20:40 Race as a Proxy for Racism
31:00 BiDiL and Race Based Medicine Definition
42:00 Dr. Duana Fullwiley and the “African Gene”
49:30 Debunking Folklore Health Narratives
53:30 Slavery Hypertension Hypothesis
57:00 Importance of Intentional and Plausible Research Methods
1:00:00 Race in Medical Algorithms
1:12:00 Moving Away from Relying on Simplistic Biological Concepts of Race
1:15:48 Advice for Listeners
1:21:00 Closing Remarks
Takeaways:
Definition of Race: Race is not a biological category, instead it is a permeable, flexible, and unstable social construction and political invention that facilitates political and economic inequality. However it is important to remember that this political invention DOES affect biology because of the way that it creates social inequity.
Historical Context: Historically, laws such as interracial marriage bans have protected established structures of white supremacy and reinforced the social construct of race.
Race is a Poor Proxy for Genetics: Diseases with genetic or population associations are often evolutionary adaptations to specific geo-environments. Race, a social construction, groups people from large swaths of of global territory based on superficial phenotype is often a poor proxy for these genetic associations with disease.
Race is a proxy for Racism: race was invented as a way to classify people into subordinate groups and support the political sanctioning of inequity. The very function of race is thus to support and uphold racism. When we evaluate race in medicine we have to recall this origin story and not rely on race as a placeholder for anything else except racism.
The Root of Inequities: Health inequities are overwhelmingly caused by differences in social status, living conditions, and experiences of discrimination. When we cling to race as the cause of health inequities, we obscure and divert attention away from these social factors that need to be addressed.
Intersectionality: Race and racism intersect with socioeconomic status, education, geography, sexual orientation, religion, immigration status, gender and other identities with differential impact.
Our responsibility in medicine: “What we have to do is include medicine in the political movement to bring down the structures of racism and white supremacy and the way in which medicine incorporates those and promotes those. And [this] HAS to be in conjunction with broader social movements…that are dedicated to radically transforming our world into one in which human beings are equally valued…”-Dorothy E. Roberts JD
For the patient I see tomorrow: Beyond recognizing that race is not a proxy for biology, we can all ask ourselves “What way is structural racism affecting my patient and what can I do about it?” The answer to this question may not be easily answered and may not always be found in the clinical setting.
Pearls:
“Genetics is not the end all be all of understanding disease” – Dorothy E. Roberts JD
An Emphasis on Genetics is Not the Solution to Race-Based Medicine
Being antiracist in medicine does not mean being more precise in our understanding of genetics. Rather we need a deeper and broader understanding of the influence of the structural and political determinants of health inequities. Part of the problem with focusing on race in medicine is that it limits our perspectives and encourages research practices that lack the rigor required to identify root causes of racial health inequities. We should be focusing on root causes rather than proxies. It does not mean that we should stop exploring genetic causes of disease, but rather that we should not pretend that understanding genetics is the solution to addressing disparities. Dr. Roberts put it expertly: “to be anti-racist, it doesn’t mean, well, then let’s just be more precise in our genetics. It means being anti all the things that race and racism do.”
Medicine Must Move Beyond Othering Black People
All too often in medicine, Black people are singled out from all other human beings as having different bodies from the norm, aka whiteness. Examples of this include: BiDiL, the blood pressure drug marketed solely to black people; arguments for race-based medicine that cite sickle cell, a disease that is most common in Black people because of geographic varietion rather than innate difference; and the slavery hypertension hypothesis which posits that hypertension disparities observed in Black people are a result of the stress of slavery and the middle passage rather than the longitudinal impacts of structural racism. Rather than searching for obscure explanations for inequalities, we must instead recognize the ways that racism impedes health at both individual and structural levels.
Race-based algorithms can produce inequity and there is a moral dilemma we must attend to
There is a persistent question about whether race-based clinical algorithms disadvantage patients and how we should think through use of them in clinical medicine. Professor Roberts offers some guidance: whenever you are stuck, go back to the origin story- what is race? Then you can ask yourself, how is race being used and does that use further inequity?
Professor Roberts also offers a few scenarios.
Race-based algorithms: Race is being used as a biological construct AND it can produce harm. For example, GFR- race correction for Black patients. The use of race is based on a false/biological concept of race AND many studies show that this can harm patients ( i.e. clinical resources are withheld based on results of algorithm). This is the rationale for NOT using these kinds of race-based algorithms.
Race “neutral” algorithms, which are used for allocation of resources for most fit patients. Race is not included in the algorithm, however because of the experiences of structural racism, certain groups will have worse scores. These worse scores may lead to the withholding of resources and ultimately further inequity. For example, the proposal of race neutral ventilator algorithms that were set up to allocate ventilators to the most fit patients during the COVID-19 pandemic. This race neutral algorithm could disadvantage Black patients, who because of structural racism may have lower fitness scores. This could worsen existing disparities in COVID-19 outcomes among Black patients.
Moral dilemma: Including race as a biological construct in clinical algorithms can lead to inequity. However whenever structural racism isn’t included in clinical algorithms, we also risk denying a group who has experienced structural racism access to much needed resources. We have not thought about this enough in medicine and we don’t have a gold standard of how to include race as a proxy for structural racism in our clinical algorithms. As we move forward we must continue to think critically about the ethical and just way to include race or rather structural racism in clinical algorithms and ensure that our algorithms do not further inequity.
References:
Lindo E, Nolen L, Paul D, Ogunwole M, Fields N, Onuoha C, Williams J, Essien UR, Khazanchi R. “Episode 140: Dismantling Race-Based Medicine, Part 1: Historical & Ethical Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. November 17, 2020.
Eneanya A, Tsai J, Williams J, Essien UR, Paul D, Fields NF, Nolen L, Ogunwole M, Onuoha C, Khazanchi R. “Episode 4: Dismantling Race-Based Medicine, Part 2: Clinical Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. December 17, 2020.
Roberts D. Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-first Century. The New Press: 2012.
Roberts D. “The problem with race-based medicine.” TEDMED 2015. Link to talk.
Roberts DE. What’s Wrong with Race-Based Medicine?: Genes, Drugs, and Health Disparities. Minnesota Journal of Law, Science & Technology. 2011;12(1):1-21.
Yudell M, Roberts D, DeSalle R, Tishkoff S. NIH must confront the use of race in science. Science. 2020;369(6509):1313-1314. doi:10.1126/science.abd4842
Roberts DE. Is race-based medicine good for us?: African American approaches to race, biomedicine, and equality. J Law Med Ethics. 2008;36(3):537-545. doi:10.1111/j.1748-720X.2008.302.x
Taylor AL, Ziesche S, Yancy C, Carson P, D’Agostino R Jr, Ferdinand K, Taylor M, Adams K, Sabolinski M, Worcel M, Cohn JN; African-American Heart Failure Trial Investigators. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004 Nov 11;351(20):2049-57. doi: 10.1056/NEJMoa042934.
The Slavery Hypertension Hypothesis: Dissemination and Appeal of a Modern Race Theory. (2003). Epidemiology, 14(1), 111-118. Retrieved May 9, 2021, from http://www.jstor.org/stable/3703292
Roberts, Dorothy E. Killing the Black Body: Race, Reproduction, and the Meaning of Liberty. New York: Pantheon Books, 1997.
Sjoding MW, Dickson RP, Iwashyna TJ, Gay SE, Valley TS. Racial Bias in Pulse Oximetry Measurement. N Engl J Med. 2020 Dec 17;383(25):2477-2478. doi: 10.1056/NEJMc2029240.
Hansen H, Netherland J. Is the Prescription Opioid Epidemic a White Problem?. Am J Public Health. 2016;106(12):2127-2129. doi:10.2105/AJPH.2016.303483
Bibbins-Domingo K, Fernandez A. BiDil for heart failure in black patients: implications of the U.S. Food and Drug Administration approval. Ann Intern Med. 2007 Jan 2;146(1):52-6. doi: 10.7326/0003-4819-146-1-200701020-00009. Erratum in: Ann Intern Med. 2007 Apr 17;146(8):616. PMID: 17200222.
Roberts DE. Abolish race correction. Lancet. 2021 Jan 2;397(10268):17-18. doi: 10.1016/S0140-6736(20)32716-1. PMID: 33388099.
The hosts and guests report no relevant financial disclosures.
Citation
Roberts, DE, Onuoha C, Khazanchi R, Nolen L, Fields N, Tsai J, Essien UR, Paul D, Ogunwole M,. “Episode 8: Dismantling Race Based Medicine Part 3: Towards Justice and Race-Conscious Medicine.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. May 10, 2021.
Episode 175: The Consult Question #2: Back pain & double vision
Apr 29, 2021
Kaitlyn Thomas is a 3rd year medical student at Lake Erie College of Osteopathic Medicine at their Seton Hill campus in Greensburg, Pennsylvania. She is interested in medical education, advocacy and assisting underserved populations. She has contributed to the CPSolvers on Virtual Morning Report on several occasions and produced a few videos for their illness scripts. In her free time, she enjoys hiking, spending time with family, and finding new recipes to cook.
Sherry Chao
Sherry Chao is a 4th year medical student at University of North Carolina at Chapel Hill. She is interested in medical education and is also an aspiring physician-scientist hoping to apply computational systems biology to understanding hematologic diseases. In her free time, she likes to travel and explore outdoors with her husband, try out new escape rooms, and play with her bearded dragon, Toothless.
Gabriela Pucci
Gabriela has graduated from Medical School at Unicamp and recently finished her neurology residency at Unesp, both in Brazil. She is interested in Medical Education and Clinical Reasoning and has obviously fallen in love with CPSolvers and VMRs since day 1. In her free time, she likes to practice pilates, play with her dogs, binge-watch Netflix comedy series, read biography books, go out with her friends (pre-COVID), drink wine, and cook (still learning).
Episode 173: Clinical unknown with Reza and Rabih at VMR: Dyspnea and finger swelling
Apr 21, 2021
Dr. Usha George, MBBS (MAHE India), MSc (Respiratory Medicine) Imperial College University of London, FRCP London, is at present attached to Sunway Medical Centre, Malaysia. It is a 650 bedded private tertiary hospital, also involved in training medical students. I practice as a Respiratory and General Medicine Physician. My special interest is in clinical and diagnostic reasoning.
Ana Clara Miranda is a 4th-year medical student from Brazil. She grew up in Belo Horizonte and moved to Rio de Janeiro in 2017 to attend medical school. Her medical interests are Pediatrics and Infectious Diseases. Today, she intends to go to the United States for an international clinical experience as a visiting student and, in 2023, apply for a Residency Program. Outside medical environment, she loves going to the beach with friends, enjoying nature and baking cakes.
Elena Vasti
Elena Vasti is a second year resident at Stanford in the department of Internal Medicine. She attended UC Davis to study Human Development and Exercise Biology and went on to UCLA Fielding School of Public Health to complete an MPH in Epidemiology and Community Health Sciences. She decided to switch careers to pursue clinical medicine and matriculated at UCSF School of Medicine in 2015. She enjoys running every day, analyzing movie trailers and both listening to and joining the CPSolvers any chance she gets! She plans to pursue a career in academic cardiology.
Episode 171: Human Dx Unknown with Sharmin – Face and leg weakness
Apr 08, 2021
Shub Agrawal is a PGY-2 at Emory’s J. Willis Hurst Internal Medicine Residency. She grew up in Athens, GA and attended New York University for undergraduate degrees in neuroscience and anthropology. She attended the AU UGA Medical Partnership for medical school where she first became passionate about medical education. She is currently doing medical education research about how to best use podcasts in UME and GME curriculum. She hopes to spend her career teaching and designing curriculum in academic medicine. Outside of medicine, she enjoys spending time with her family, friends and imagining all the trips she will take once it is safe to travel again!
Dr. Sadjadi
Raha Sadjadi is a PGY2 internal medicine resident at Emory University School of Medicine. She grew up in the San Francisco Bay Area and attended UC Berkeley for undergrad. After spending her whole life in the Bay Area, she moved to Atlanta to complete medical school at Emory University. At Emory she pursued her passion for caring for underserved populations while rotating at Grady Hospital and she found wonderful mentors invested in her growth as a physician and human. For these very reasons, she remained at Emory to complete her internal medicine residency. She is interested in transplant hepatology and in reducing healthcare disparities.
Dr. Rubiano
Carlos Rubiano is an Inpatient Medicine chief at UNC Hospitals where he also completed his internal medicine residency training. Prior to moving to North Carolina with his wife with whom he couples matched with, he completed his medical school training at Florida State University and undergraduate training in Biology at Florida Gulf Coast University. In medicine, he has a particular interest in medical education and hopes to be a clinician-educator as a soon-to-be hospitalist and one day as an ID clinician. Outside of medicine he loves playing pickleball and invites everyone to try this booming sport.
Episode 170: Human Dx Unknown with Jack – generalized itching
Apr 06, 2021
Eamonn hails from Charleston, West Virginia. He attended Marshall University for medical school and is currently in his final year of Dermatology residency at SLU. He will complete a Complex Medical Dermatology fellowship at NYU next year and hopes to practice with a focus on cutaneous lymphomas, connective tissue diseases, and immunobullous disorders. Outside of work he enjoys jiu jitsu, playing soccer, and spending quality time with his wife.
Ashley Boerrigter
Ashley Boerrigter is a third-year OBGYN resident at St. Louis University, where she will be Administrative Chief Resident for the 2021-2022 academic year. She attended medical school at the University of Kentucky and her academic interests include medically complex pregnancies and curriculum development. Hobbies include tennis, sailing, and alternating between beach sunning and mountain skiing.
In this episode of Clinical Problem Solvers: Anti-Racism in Medicine, we are joined by Michelle Morse, MD, MPH, Deputy Commissioner for the Center for Health Equity and Community Wellness (CHECW) and the inaugural Chief Medical Officer at the NYC Department of Health and Mental Hygiene (NYCDOHMH), and Paul Farmer, MD, PhD, Kolokotrones University Professor of Global Health and Social Medicine at Harvard University. Together, we discuss what global health equity looks like in the age of COVID-19.
Learning Objectives
After listening to this episode listeners will be able to…
Recognize that global health equity and global vaccine equity are everyone’s responsibility
Understand what decolonizing global health really means
Appreciate the importance of solidarity and human interconnectedness
Credits
Written and produced by: Dereck Paul, MS, Chioma Onuoha, Utibe R. Essien, MD, MPH, Rohan Khazanchi, LaShyra Nolen, Naomi Fields, Michelle Ogunwole, MD, Jazzmin Williams, and Jennifer Tsai MD, M.Ed
Guests: Michelle Morse, MD, MPH (@michellemorse) and Paul Farmer, MD, PhD
Timestamps
00:00 Introductions
04:00 What Brought You to Global Health Work?
11:50 Why is Global Health Equity Everyone’s Problem?
23:40 How has COVID-19 Changed Global Health Work and Perspectives?
40:30 The Role of Identity in Global Anti-Racism Work
49:00 Decolonize Global Health Movement
1:02:49 Hope for the Future
Takeaways
1. The Global COVID-19 Response Must Be Anti-Racist
An anti-racist COVID-19 response means that quality care, quality vaccines, and quality public health information must be provieded to all. From social distancing to contact tracing to vaccin distribution, every step should be considered through an anti-raicst framework. This includes financing vaccine acquisition for all countries and avoiding the global north vaccine hoarding that is happening today. It is important that we avoid vaccine tunnel vision and recognize the broader social context and need for social support systems worldwide.
2. The Four S’s
As Dr. Paul Farmer often says, an effective infectious disease global health response requires:
Staff – caregivers with the knowledge and passion to address health concerns
Stuff – the physical materials required for effective treatment or intervention
Space – places where people can safety receive appropriate care
Systems – policies and institutional systems that facilitate needed health responses
3. Why should everyone care about global vaccine equity?
“Unless everyone is safe, no one is” – Dr. Paul Farmer
The world is incredibly interconnected and, as COVID-19 has shown, we have to recognize the idea of collective survival. Health and well being is a global endeavor and an interdependent fight. Furthermore, we must reclaim the heart and soul of medicine: caretaking, healing, and the creative aspects of the profession that oftentimes get pushed to the side. American physicians and health professionals have immense power and a duty to use that power for the greater good to interrupt, and interrogate the colonial and imperial practices perpetrated by our own government. We must hold our government accountable. At the heart of this is a need for global solidarity.
Pearls
The Importance of this Moment
Both of our guests highlighted the HIV/AIDS movement as a catalyst for their continuing passion for global health equity. The COVID-19 pandemic provides a similar opportunity today for us to scale up our critical consciousness and re-examine the functioning of our society. People are naming racism, settler colonialism, and imperialism more than ever. In this current moment we can build on that momentum, shift perspectives and work towards long lasting equitable and anti-racist change.
Dangers of American Exceptionalism
It is imperative that we look beyond the walls of our nation and the privileges that living in the United States afford us in order to recognize the danger of American exceptionalism and how it impacts people across the world. For example, currently the United States, and other wealthy countries, are hoarding COVID-19 vaccines making it difficult for other countries to vaccinate their populations. Considering the interconnectedness of our world, by preventing equitable vaccine distribution we will only lengthen the current pandemic. As a country, we must expand our global critical consciousness and strive towards global equity by financing vaccine acquisition, investing in our education systems, interrogating American privilege and more.
Decolonizing Global Health – Allow the Global South to Lead
Part of decolonizing global health means being willing to take a backseat when it comes to defining, researching, and executing global south health priorities. This is especially true for large outside universities and institutions that habitually fail to engage domestic stakeholders in research and health decision making processes. We must trust the communities we serve to teach us and to guide initiatives.
Richardson, E. T., Malik, M. M., Darity, W. A., Mullen, A. K., Morse, M. E., Malik, M., . . . Jones, J. H. (2021). Reparations for Black American descendants of persons enslaved in the U.S. and their potential impact on SARS-CoV-2 transmission. Social Science & Medicine, 113741. doi:10.1016/j.socscimed.2021.113741
The hosts and guests report no relevant financial disclosures.
Citation
Morse M, Farmer PE, Onuoha C, Khazanchi R, Nolen L, Fields N, Ogunwole M, Tsai J, Essien UR, Paul D. “Episode 7: Anti-Racism, Global Health Equity, and the COVID-19 Response.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. April 1, 2021.
Episode 168: Clinical unknown with Reza and Rabih at VMR
Mar 24, 2021
Dr. Usha George (MBBS (MAHE India), MSc (Respiratory Medicine) Imperial College University of London, FRCP London) is at present attached to Sunway Medical Centre, Malaysia. It is a 650 bedded private tertiary hospital, also involved in training medical students. I practice as a Respiratory and General Medicine Physician .My special interest is in clinical and diagnostic reasoning.
Episode 167: Unilateral sensory changes
Mar 23, 2021
Maria Jimena Aleman was born and raised in Guatemala where she currently is a medical student in Universidad Francisco Marroquin. After suffering from long standing neurophobia, she has embraced her love for neurology and will pursue a career in this field. She also looks forward to dedicating her life to breaking barriers for Latin women in medical fields and improving medical care in her country. Maria is one of the creators of a medical education podcast in Spanish called Intratecal. Her life probably has a soundtrack of a mix between Shakira and Louis Armstrong. Outside of medicine she enjoys modern art, 21st century literature and having hour long conversations over a nice hot cup of coffee or tequila.
Mohamed Elashwal
Mohamed is a senior medical student at Alfaisal University in Riyadh Saudi Arabia. He was born in Egypt before he moved with his family to Saudi. Mohamed is interested in adult neurology; his neurophilia started in one morning report during his neuroscience rotation when he could feel his heart racing and his brain twisting thinking about the cases. He plans to apply to neurology residency next year. In his free time, Mohamed enjoys baking, and cooking; he also likes playing the piano (level: very amateur).
Kannu Bansal
Kannu is a junior resident at All India Institute of Medical Sciences, New Delhi, India working in the Kidney Transplant Wing. Despite my current affiliation with transplantation, I love to explore everything related to medicine. My passions include quizzing, teaching, and learning, and that’s how I came to know about CPSolvers. I plan to pursue Internal Medicine Residency in United States. Outside of medicine, I like to watch soccer, Formula 1, and sketch pencil portraits.
Patreon Exclusive: RLR 41- Bilateral vision loss
Mar 23, 2021
Want to test your learning? Take our episode quiz here
Dr Ann Marie Kumfer is a new residency graduate and academic hospitalist at UNC. After completing medical school at Texas Tech University, she moved up to North Carolina for residency. She liked UNC so much, she decided to stay as an academic hospitalist after completing residency in June. She also serves as a section editor for the Human Diagnosis project. She is passionate about diagnostic reasoning, teaching, and guacamole.
Dr. Debra Bynum is the Director for the Internal Medicine Residency Program at the University of North Carolina. Originally from eastern North Carolina, she graduated from Davidson in 1990 with a degree in Biology and a focus on ecology and marine biology. From there, she came to Chapel Hill for medical school and stayed at UNC for residency training. After completing a year as Chief Resident, she joined the faculty at WakeMed hospital where she worked in the clinic caring for Raleigh’s underserved, attended on the inpatient service with UNC residents and students, and helped to found one of the first hospitalist programs in the area.
After three years at WakeMed, she returned to UNC for further training as a fellow in the Geriatric Medicine program and was appointed to a faculty position in 2001. During the subsequent fourteen years, she held multiple leadership positions within the School of Medicine, the Department of Medicine, and the Geriatric Medicine Fellowship and Internal Medicine Residency programs. She directed the Acting Internship for senior students as well as co-directed the clinical skills course for second year students, served on the School of Medicine education committee, and helped to design, implement, and co-direct both a transition course for new third year students as well as a teaching elective for fourth year students. She served as the Program Director for the Geriatric Medicine Fellowship from 2008-2014 and was selected to lead the Internal Medicine residency program in May of 2014.
Want to learn more about the Women in Diagnosis (WDx) series?
Episode 164: Spaced Learning Series – Abdominal pain and hypotension
Mar 04, 2021
Scott Walker grew up in Knoxville, Tennessee (Go Vols) where he completed his Bachelors in Kinesiology and Nutrition. He currently attends The University of Central Florida College of Medicine as a third year medical student. He is interested in entering the field of Emergency Medicine and is passionate about medical education and medical mission trips. He spends his spare time watching The Office with his wife or weight lifting.
Dr. Devika Gandhi
Devika Gandhi is a third-year internal medicine resident at Indiana University. She is originally from Dayton, Ohio and received her undergraduate degree from the University of Akron. She earned her medical degree from Northeast Ohio Medical University in Rootstown, Ohio (Go Walking Whales!). After residency she will be an incoming gastroenterology/hepatology fellow at Loma Linda University in California. During her free time, she enjoys reading, cooking, and going out to trivia with friends.
Episode 162: Antiracism in Medicine Series – Episode 6 – Racism, Trustworthiness, and the COVID-19 Vaccine
Feb 25, 2021
In Episode 6 of the Antiracism in Medicine series, “Racism, Trustworthiness, and the #COVID19 vaccine,” we are joined by two forces in the field of health equity and academic medicine, Dr. Giselle Corbie-Smith and Dr. Kimberly Manning, to discuss why the pandemic is the moment to ensure trust in medicine.
Learning Objectives
After listening to this episode listeners will be able to…
Recognize the importance of yielding privilege and power to better center marginalized voices and communities through individual, interpersonal, institutional, and systemic actions.
Understand the importance of looking beyond isolated and individual instances of mistrust, in recognition that the continued and ubiquitous insults of structural and systemic racism are the primary forces perpetuating mistrust among minoritized communities.
Identify potential individual, institutional, and policy-level actions to address COVID-19 vaccine inequities.
Credits
Written and produced by: Utibe R. Essien, MD, MPH, Rohan Khazanchi, LaShyra Nolen, Naomi Fields, Dereck Paul, MS, Michelle Ogunwole, MD, Chioma Onuoha, Jazzmin Williams, and Jennifer Tsai MD, M.Ed
Show Notes – Episode 6: Racism, Trustworthiness, and the COVID-19 Vaccine
Rohan Khazanchi
February 23rd, 2021
Summary
In this episode of Clinical Problem Solvers: Anti-Racism in Medicine, we are joined by Dr. Kimberly Manning, Professor of Medicine and Associate Vice Chair for Diversity, Equity, and Inclusion at Emory University, and Dr. Giselle Corbie-Smith, the Kenan Distinguished Professor of Social Medicine and Director of the Center for Health Equity Research at University of North Carolina-Chapel Hill. We dig into Dr. Manning’s leading perspectives on trust in the Black community and Dr. Corbie-Smith’s longstanding community-engaged research agenda, and we discuss implications for ongoing discourse about COVID-19 vaccine equity.
Timestamps
00:00 Music/Intro
1:25 Guest Introductions
02:34 Reflecting upon the current “moment of hope” in the COVID-19 pandemic
07:46 Why is Mistrust the “Tip of a 400-Year-Old Iceberg”?
12:04 Getting to the Individual “Why” of Declining the COVID-19 Vaccine
13:01 Is Mistrust the True Root Cause?
16:28 Moving past our preconceptions about vaccine mistrust
19:01 “When your immune system is knuckin’ and buckin’, it’s gonna be a little raucous!”
22:43 Shifting our framing from “vaccine hesitant” to vaccine deliberations
27:58 Recognizing our biases, centering the margins, and avoiding diluted generalizations
37:20 Valuing diversity rather than classifying minoritized groups as monoliths
43:34 Why Dr. Manning chose to participate in the Moderna vaccine trial
49:20 The “allostatic load” of the minority tax in a white supremacist system
55:45 Performative advocacy and the “musical chairs” of representation in medicine
58:12 The fallacy of the meritocracy
59:10 What can health systems do to reduce vaccine disparities?
1:06:20 Takeaways and conclusions
1:08:51 Outtakes Takeaways
Medical Mistrust in the Black Community is More than Tuskegee
Framing medical mistrust solely around watershed incidents like the U.S. Public Health Service Study of Untreated Syphilis at Tuskegee is harmful. It treats Black Americans as a monolith, when there is an enormous diversity and heterogeneity within the Black community. It treats mistrust as an isolated construct, when medical mistrust is intertwined with broader societal injustices. Lastly, our rhetoric often treats mistrust as an individual failing or “uninformed belief”, rather than a consequence of structural inequity.
In contrast, scholarship and clinical care which acknowledges within-group differences and shifts from a deficit-based to an asset-based view of marginalized groups can help us better serve our minoritized patients. Dr. Manning reaffirmed what Dr. Camara Jones told us last episode– that solutions lie in simultaneously emphasizing the importance of individual humanity and value in “hard to reach” (hardly reached) communities and dismantling the structures which push those communities down.
“Black Why’s Matter”
“Simply telling people what to do doesn’t work on your children, and it doesn’t work on your patients.” – Dr. Kimberly Manning
Every person who declines a COVID-19 vaccine has a reason to do so which is theirs, and theirs alone. As clinicians, we need to slow down and demonstrate our willingness to hear the “why’s” of our patients, colleagues, neighbors, and community members. In particular, racial concordance is a key piece of doing this work; authentic communication styles from people who personally understand the needs of their community and can better help motivate a “slow yes” through shared decision-making.
Addressing Racial Vaccine Inequities Requires Race and Community-Informed Solutions
This pandemic has highlighted a faultline between public health and medicine. Crossing that breach must involve organizing with faith-based and community-based organizations, community health workers, and beyond. Geographically-based interventions need to prioritize individuals from those communities, rather than allowing outsiders to take designated slots. Scapegoating mistrust can no longer be an excuse for not meeting people where they are and addressing longstanding, long-understood barriers.
Pearls
Reframe “Vaccine Hesitancy” as “Vaccine Deliberations”
“Vaccine hesitancy” is a symptom of a larger, chronic issue about the way Black and Brown people are treated in the United States. Yet, our narrow focus on the individual drives us to assign blame to those who decline a vaccine as “hesitant” or “distrusting” when there are a plurality of reasons why. Deliberating on big decisions is quite normal, especially when the lived experiences of individuals in historically marginalized groups inform their reasonable apprehension about inequities in U.S. systems writ large.
Minority Tax and the “Musical Chairs” of Representation in Medicine
“My taxation is not without representation… [musical chairs] is all fun and games until somebody has to give up their seat. If everything has been built on privilege, you have to be willing to give something up” – Dr. Kimberly Manning
Dr. Manning presented an analogy to us about a game of musical chairs, in which everyone is happy to participate and speak up for marginalized groups until the music stops and only one seat is left. Minoritized clinicians and researchers face the allostatic burden of stepping up to fix a broken system designed within a white supremacist culture. Performative activism only goes so far; when our colleagues with privilege aren’t willing to give up that power, the needle doesn’t get moved.
“I’m not interested in changing hearts and minds; I’m interested in seeing behavior change and changes in policies, practices, and norms.” – Dr. Giselle Corbie-Smith
References Mentioned
08:14
Manning KD. More than medical mistrust. The Lancet. 2020 Nov; 396(10261): 1481-1482. doi:10.1016/S0140-6736(20)32286-8.
13:01
Corbie-Smith G, Thomas SB, St George DM. Distrust, race, and research. Arch Intern Med. 2002 Nov 25;162(21):2458-63. doi: 10.1001/archinte.162.21.2458. PMID: 12437405.
32:18
Corbie-Smith G, Miller WC, Ransohoff DF. Interpretations of ‘appropriate’ minority inclusion in clinical research. Am J Med. 2004 Feb 15;116(4):249-52. doi: 10.1016/j.amjmed.2003.09.032. PMID: 14969653.
33:56
Corbie-Smith G, Thomas SB, St George DM. Distrust, race, and research. Arch Intern Med. 2002 Nov 25;162(21):2458-63. doi: 10.1001/archinte.162.21.2458. PMID: 12437405.
Corbie-Smith G, Thomas SB, Williams MV, Moody-Ayers S. Attitudes and beliefs of African Americans toward participation in medical research. J Gen Intern Med. 1999 Sep;14(9):537-46. doi: 10.1046/j.1525-1497.1999.07048.x. PMID: 10491242; PMCID: PMC1496744.
39:42
Wilkerson, I. (2020). Caste: The origins of our discontents.
Sengupta S, Corbie-Smith G, Thrasher A, Strauss RP. African American elders’ perceptions of the influenza vaccine in Durham, North Carolina. N C Med J. 2004 Jul-Aug;65(4):194-9. PMID: 15481486.
Quinn SC, Jamison A, An J, Freimuth VS, Hancock GR, Musa D. Breaking down the monolith: Understanding flu vaccine uptake among African Americans. SSM Popul Health. 2017 Nov 14;4:25-36. doi: 10.1016/j.ssmph.2017.11.003. PMID: 29349270; PMCID: PMC5769118.
Disclosures
The hosts and guests report no relevant financial disclosures.
Citation
Manning KD, Corbie-Smith G, Khazanchi R, Nolen L, Fields N, Ogunwole M, Onuoha C, Tsai J, Paul D, Essien UR. “Episode 6: Racism, Trustworthiness, and the COVID-19 Vaccine.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. February 23, 2021.
Patreon Exclusive: RLR 39 – Fever, dyspnea, and back pain
Feb 22, 2021
Rabih and Reza tackle a case of fever, dyspnea, and back pain presented by guest presenter Lawrence Yuen.
We kick off our new series, “The Consult Question”, aimed at highlighting the clinical reasoning of our subspecialty colleagues, with a case of hypoglycemia presented to master endocrinologist Dr. Elizabeth Murphy.
Dr. Elizabeth Murphy is a professor of Medicine at the University of California, San Francisco, where she serves as the Deborah Cowan Endowed Professor of Endocrinology and chief of the Endocrinology and Metabolism Division at Zuckerberg San Francisco General Hospital.
Episode 160: Neurology VMR: Hiccups + vertigo
Feb 16, 2021
Dhruv Srinivasachar is a 4th year medical student at Virginia Commonwealth University School of Medicine (the Medical College of Virginia for all the veteran attendings out there). Introduced to medicine through research, Dhruv has shifted his passions to empathetic clinical care and medical education, as a contributor to the CPSolvers (especially through VMR as a case presenter, discussant, and compiler of cases) and team member for the Not Just Little Adults podcast (CPedsSolvers, if you will). When he’s not interviewing for Med-Peds residency, he can be found biking around Richmond, VA, gardening, and cooking.
Elena Vasti
Elena Vasti is a second-year resident at Stanford in the Department of Internal Medicine. She attended UC Davis to study Human Development and Exercise Biology and went on to UCLA Fielding School of Public Health to complete an MPH in Epidemiology and Community Health Sciences. She decided to switch careers to pursue clinical medicine and matriculated at UCSF School of Medicine in 2015. She enjoys running every day, analyzing movie trailers and both listening to and joining the CPSolvers any chance she gets! She plans to pursue a career in academic cardiology.
Patreon Exclusive: RLR 38 – Dyspnea (with guest presenter Sean Carter!)
Feb 16, 2021
Sean presents a case of dyspnea to Rabih and Reza.
Maani, Priyanka, and Lindsey discuss a clinical unknown with Dr. Jori May.
Want to test your learning? Take our episode quiz here
Dr. Jori May
Jori May, MD, is Assistant Professor of Medicine in the Division of Hematology/Oncology at the University of Alabama at Birmingham (UAB). Her clinical interest is non-malignant hematology, focusing on the care of patients with thrombosis and coagulation disorders. Additionally, she focuses on systems-based hematology, which works to improve hematologic care delivery across health systems. Dr. May earned her M.D. from Washington University School of Medicine in St. Louis. She completed her residency, chief residency, and fellowship in Hematology/Oncology at UAB.
Want to learn more about the Women in Diagnosis (WDx) series?
Erica Smith is a fourth year Internal Medicine-Pediatrics resident at the University of Michigan. She is from Detroit, MI and attended Wayne State University School of Medicine for medical school. She is planning to pursue a career in hospital medicine. In her free time, she enjoys golf, yoga, and hiking.
Dr. Mansour Alkhunaizi
Mansour Alkhunaizi went to the Royal College of Surgeons in Ireland for medical school and is currently an Internal Medicine Resident at Baylor College of Medicine. He is interested in a career in pulmonary/critical care medicine. Outside of work, he enjoys hiking, working out, and watching his favorite soccer team Manchester United!
Dr. Kristin Andres
Kristin Andres is currently a third year Internal Medicine-Pediatrics resident at the University of Michigan. She grew up in Lexington Kentucky and attended the University of Kentucky for both undergraduate and medical school. She hopes to pursue Pediatric Cardiology fellowship with a career goal of optimizing transitional care for patients with congenital heart disease. Outside of the hospital, Kristin enjoys musical theatre, pub-style trivia, making ice-cream, and snuggling on the couch with her husband Andrew and dog Nutmeg.
Episode 156: Human Dx Unknown with Sharmin – Bilateral wrist pain
Jan 25, 2021
Want to test your learning? Take our episode quiz here
Dr. Sonya Davey
Sonya Davey attended medical school at the Perelman School of Medicine at the University of Pennsylvania and is currently an Internal Medicine PGY-1 at Brigham & Women’s Hospital. She loves to travel, read, and enjoy meals with family and friends.
Dr. Nicky Singh
Nicky Singh attended medical school at the Perelman School of Medicine at the University of Pennsylvania and is a current PGY-3 resident at Massachusetts General Hospital. As a resident, he has been involved with several educational initiatives, including co-leading the Residents in Medical Education interest group and the Point of Care Ultrasound group and serving as an Education Council representative and Simulation Program Chief. He is interested in cardiology and medical education. Outside of medicine, he enjoys hiking, South Asian dance, exploring new recipes with his Instant Pot, and trying to up his Peloton numbers.
Dr. Aaron Sabal
Aaron is currently a PGY-3 at Mercy Health Muskegon aspiring for a career in hospital medicine. He was born and raised in Westland, MI (Detroit metro area) and went to Wayne State University for his undergraduate studies thinking he would be a physical therapist, massage therapist, and dietitian (yes, all three of those). However, one week prior to starting a massage therapy program, he had an epiphany and decided to go to medical school instead. He was fortunate to be accepted at MSUCOM and fell in love with Internal Medicine. His passions include all things medical. In particular, he is passionate about medical education, how best to help physicians learn, diagnostic reasoning, and creating an environment of learning where no one is afraid to express what they’re thinking. When he is not pursuing his love of learning, he is spending time with his wife and their boys (2 cats and a dog), playing with his animals, preparing to be a father to his soon-to-be-born son, crossfitting, doing DIY home-improvement projects, exploring national parks, or reading good nonmedical fiction with a cat or dog in his lap begging for his love and attention.
Patreon Exclusive: RLR 35 – Abdominal pain
Jan 25, 2021
In this episode of Clinical Problem Solvers: Anti-Racism in Medicine, we are joined by Aletha Maybank MD, MPH, the American Medical Association’s (AMA) inaugural Chief Health Equity Officer and director of the AMA’s Center for Health Equity, and Camara Jones MD, PhD, MPH, thought leader in the fields of health equity and public health and former president of the American Public Health Association (APHA). We discuss policy, professional organizations, and history as they relate to advancing health equity, and imagine what the anti-racist health system of the future looks like.
Learning Objectives
After listening to this episode listeners will be able to…
Recognize that racism is both structural and interpersonal, and that both aspects must be addressed simultaneously.
Appreciate the importance of acknowledging history and sustaining institutional memory in advancing anti-racism efforts and achieving structural change.
Understand that collective action and a focus on community, rather than individualism, are most effective in combating racism and achieving health equity.
Credits
Written and produced by: Rohan Khazanchi, LaShyra Nolen, Naomi Fields, Dereck Paul, MS, Utibe R. Essien, MD, MPH, Michelle Ogunwole, MD, Chioma Onuoha, Jazzmin Williams, and Jennifer Tsai MD, M.Ed
Episode 5: Racism, Power, and Policy: Building the Antiracist Health Systems of the Future
Show Notes
Chioma Onuoha
Timestamps
00:00 Music/Intro
01:14 Guest Introductions
03:09 Framing Racism
05:15 Allegory: Cement Dust in Our Lungs
07:00 The AMA’s Declaration on Racism as a Public Health Threat
13:28 History and the AMA and APHA Movements
15:20 Barriers to Achieving Health Equity in Medicine
20:55 Documenting, Centering, and Institutionalizing “The Work”
23:30 The AMA’s Racist Past
31:00 How Do We Create Sustainable Work?
35:25 Creating and Maintaining Urgency
39:00 Racism Saps the Strength of the Whole Society
43:43 Building an Anti-Racism Health Care System from A Grassroots Level
52:15 Building an Anti-Racism Health Care System from A Governmental Level
53:45 Health is Not Created with the Health Sector
56:53 Why Must All Health Workers Practice Anti-racism?
1:05:57 Outtakes
Takeaways
Name Racism for What It Is
If we don’t explicitly say the word racism, and identify its historical context, then we are complicit in its denial. Racism denial is deeply ingrained in our society and it needs to be called out and recognized as a system in order to be addressed. Though the field of medicine often fails to think systematically, it is imperative that all healthcare workers learn to recognize racism, actively practice anti-racism, and acknowledge the many systems that impact people and community’s health.
Four Key Messages for Naming Racism:
Racism Exists
Racism is a System
Racism Saps the Strength of the Whole Society
We can Act to Dismantle Racism
History and Documentation are Key
Our country habitually denials racism by working to make its impacts invisible. Remembering history and collecting institutional memory avoids the danger of repeating work, wasting labor, and makes clear racism’s long standing effects. Part of this effort also includes learning the history of the organizations and institutions we are a part of.
Focus on the Community
While the health sector is where illness and ailments are often treated, a person’s health largely manifests outside of the health sector and is impacted by their community and environment. One of the biggest barriers to health equity is the narrow focus on the individual and a failure to see health as a widespread community issue. We must recognize that all policy is health policy and that which affects someone outside of the health sector may also affect their health. Our future should be grounded in our communities; our solutions cannot solely be declarative or institution-driven.
Pearls
Barriers to Achieving Health Equity
Narrow focus on the individual – makes systems and structures invisible or irrelevant
We as a nation are ahistorical – we need to bring history into the fold
Our endorsement of the myth of meritocracy – the uneven playing field
A movement can disappear as quickly as it arose if it is not institutionally ingrained. This means that anti-racism must be embedded into practice, performance standards and institutional culture. All policies, decisions, and behaviors should occur through the lens of anti-racism in order for its impact to be longstanding and effective.
The Power of Collective Action
“When we acknowledge each other’s work we acknowledge the power of collective action”
– Dr. Camara Jones
Addressing structural racism is a collective effort and is more effective when we shift from “what can I do” to “what can we do”. When we lift up our peers and validate/center the work of people on the margins, we recognize the power of collective action and ensure that efforts are not erased or lost. This includes recognizing the experts that have come before us and reaching out to younger generations.
Addressing Structures and Values
Racism is a system of structuring opportunity and assigning value based on the social interpretation of how one looks. In order to address racism, we must address both the structures and the values. Structures include the ways that racism is institutionalized and systematically reinforced, and values include the way that racism manifests in our shared consciousness. Addressing values will require us to make clear that “racism saps the strength of the whole society” and to highlight the urgency of anti-racism efforts. Additionally, we should equip educators, parents, and those who will guide the next generations with the tools to operate within the framework of anti-racism. Because structural racism often operates through inaction and complacency, the work to combat it must be persistent and collective. Racism hurts all people and achieving anti-racism will require active “fellows in the struggle” not just feeling allies.
Jones, C. Camara Jones, APHA executive director citation award acceptance speech. [Video]. YouTube. https://youtu.be/BGmIXV859YQ. Published December 2, 2020. Accessed December 9, 2020.
Berney, B., & Friedman, R. (Producers), & Burnett, C., Loewenthal, D. (Directors). (2018). Power to Heal: Medicare and the Civil Rights Revolution. Retrieved from https://www.blbfilmproductions.com/
28:55
Baker, RB., et al. Creating a segregated medical profession: African American physicians and organized medicine, 1846-1910. J Natl Med Assoc. 2009 Jun;101(6):501-12. doi: 10.1016/s0027-9684(15)30935-4. PMID: 19585918.
Washington, HA., et al. Segregation, civil rights, and health disparities: the legacy of African American physicians and organized medicine, 1910-1968. J Natl Med Assoc. 2009 Jun;101(6):513-27. doi: 10.1016/s0027-9684(15)30936-6. PMID: 19585919.
Additional References
Boyd RW, Krieger N, Jones CP. In the 2020 US election, we can choose a just future. Lancet. 2020;396(10260):1377-1380. doi:10.1016/S0140-6736(20)32140-1
Crear-Perry J, Maybank A, Keeys M, Mitchell N, Godbolt D. Moving towards anti-racist praxis in medicine. Lancet. 2020;396(10249):451-453. doi:10.1016/S0140-6736(20)31543-9
Ford CL, Airhihenbuwa CO. The public health critical race methodology: praxis for antiracism research. Soc Sci Med. 2010 Oct;71(8):1390-8. doi: 10.1016/j.socscimed.2010.07.030. Epub 2010 Aug 11. PMID: 20822840.
Jaffe S. Aletha Maybank: AMA’s Chief Health Equity Officer. The Lancet. 2020;395(10242):1963. doi:10.1016/S0140-6736(20)31408-2
Jones CP, Holden KB, Belton A. Strategies for Achieving Health Equity: Concern about the Whole Plus Concern about the Hole. Ethn Dis. 2019;29(Suppl 2):345-348. doi:10.18865/ed.29.S2.345
Jones CP, Jones CY, Perry GS, Barclay G, Jones CA. Addressing the social determinants of children’s health: a cliff analogy. J Health Care Poor Underserved. 2009;20(4 Suppl):1-12. doi:10.1353/hpu.0.0228
Jones CP. Confronting Institutionalized Racism. Phylon 2003;50(1-2):7-22.
Jones CP. Overcoming Helplessness, Overcoming Fear, Overcoming Inaction in the Face of Need. Am J Public Health. 2016;106(10):1717. doi:10.2105/AJPH.2016.303406
Jones CP. Systems of Power, Axes of Inequity: Parallels, Intersections, Braiding the Strands. Medical Care. 2014;52:S71. doi:10.1097/MLR.0000000000000216
Jones CP. Toward the Science and Practice of Anti-Racism: Launching a National Campaign Against Racism. Ethn Dis. 2018;28(Suppl 1):231-234. doi:10.18865/ed.28.S1.231
Jones, C. Camara Jones, APHA executive director citation award acceptance speech. [Video]. YouTube. https://youtu.be/BGmIXV859YQ. Published December 2, 2020. Accessed December 9, 2020.
Jones, CP [@CamaraJones]. (2020, Nov 28). My map with the 28 states (in red) with at least one city/county/state-level body declaring “Racism is a public health crisis.” Each state name is followed by the number of jurisdictions making these declarations. State name is in CAPS if there is a state-level declaration. [Tweet]. Twitter. https://twitter.com/CamaraJones/status/1332729107952627712?s=20
Metzl JM, Maybank A, De Maio F. Responding to the COVID-19 Pandemic: The Need for a Structurally Competent Health Care System. JAMA. 2020;324(3):231-232. doi:10.1001/jama.2020.9289
Dr. Maybank is the AMA’s Chief Health Equity Officer and director of the Center for Health Equity. Mr. Khazanchi is a member of the American Medical Association’s Council on Medical Education. The views presented herein represent their own and not necessarily those of the AMA. The hosts and guests report no other relevant financial disclosures.
Citation
Jones CP, Maybank A, Nolen L, Fields N, Ogunwole M, Onuoha C, Williams J, Tsai J, Paul D, Essien UR, Khazanchi, R. “Episode 5: Racism, Power, and Policy: Building the Antiracist Health Systems of the Future.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. January 19, 2021.
Episode 154: Clinical unknown with Dr. Armitage – Headache
Jan 15, 2021
Want to test your learning? Take our episode quiz here
Dr. Dayyan Adoor
Dayyan Adoor is a 2nd year internal medicine resident at Case Western Reserve/University Hospitals. Following residency, he hopes to pursue a fellowship in Gastroenterology! In his free time, he likes to spend his time outdoors, often exploring the beautiful parks in Cleveland, and lately, learning how to ski!
Dr. Keith Armitage
Dr. Keith Armitage is a professor of medicine in the division of infectious diseases at the Case Western Reserve University School of medicine. He is also the program director for the internal medicine residency at the Case Western Reserve/University hospitals internal medicine residency program where he is currently serving his 29th year as program director. In his free time Dr Armitage enjoys cheering on his beloved Arsenal Football Club and spending time with his wife and three daughters.
Dr. Keith Albrektson
Keith Albrektson is a current chief resident at the Case Western Reserve/University hospitals internal medicine residency where he completed his internship and residency in internal medicine. Following his chief year he will be continuing his training in pulmonary and critical care at the University of New Mexico Medical Center.
Kaitlyn Thomas is a 3rd year medical student at Lake Erie College of Osteopathic Medicine at their Seton Hill campus in Greensburg, Pennsylvania. She is interested in medical education, advocacy and assisting underserved populations. She has contributed to the CPSolvers on Virtual Morning Report on several occasions and produced a few videos for their illness scripts. In her free time, she enjoys hiking, spending time with family, and finding new recipes to cook.
Ninad Bhat
Ninad Bhat is a third-year medical student at UCSF. He has always been fascinated by communication and the brain, seeking to combine his interests by becoming a neurologist involved in medical education. In his free time, he writes poetry and works to keep his obligatory medical student plants alive.
Andrew Levy
Andrew Levy is a 4th-year medical student at the University of Colorado SOM applying to Family Medicine with interests in Primary Care, Global Health, and Population Health. After taking a year off to help implement a WHO educational community-based first aid response program, he is now pursuing further public health training through UCSF in Implementation Sciences. He has been a fan of CPSolvers since being turned onto it, as well as the general topic of diagnostic reasoning, through Juan Lessing, an IM attending at the University of Colorado Hospital. In his free time, he enjoys exploring the great outdoors with his wife, Emily a fourth-year medical student at RVU in Colorado, and their three dogs Layla, Jade, and Avalanche.
Patreon Exclusive: RLR 34 – LFT Abnormality
Jan 11, 2021
Rabih and Reza take us on a journey through liver function test abnormalities
Originally from Atlanta, Georgia, Amara spent time in Massachusetts, Vermont, British Columbia, Connecticut and Colorado before returning to the vibrant ATL for medical school. She is now an intern in the Med-Peds program at the University of Arizona in Phoenix. She is passionate about better understanding the relationship between early life exposures and lifelong health as a means to improve preventive medicine for kiddos, re-imagine our approach to adult disease, and disrupt intergenerational cycles of health inequity. Outside of the hospital you can find her hiking, biking, writing, and working on her collection of fermented foods including kimchi and hot sauce.
Kelly is a second-year internal medicine resident at Mercy Health in Muskegon, MI. I’m from Wisconsin and went to medical school at LMU-DCOM in Tennessee. I am looking forward to a career in hospitalist medicine once I finish residency. In my free time, I enjoy traveling (pre-COVID, anyway), cooking, reading fiction, and playing with my dog, Bubba.
Dr. Aaron Sabal
Aaron is currently a PGY-3 at Mercy Health Muskegon aspiring for a career in hospital medicine. He was born and raised in Westland, MI (Detroit metro area) and went to Wayne State University for his undergraduate studies thinking he would be a physical therapist, massage therapist, and dietitian (yes, all three of those). However, one week prior to starting a massage therapy program, he had an epiphany and decided to go to medical school instead. He was fortunate to be accepted at MSUCOM and fell in love with Internal Medicine. His passions include all things medical. In particular, he is passionate about medical education, how best to help physicians learn, diagnostic reasoning, and creating an environment of learning where no one is afraid to express what they’re thinking. When he is not pursuing his love of learning, he is spending time with his wife and their boys (2 cats and a dog), playing with his animals, preparing to be a father to his soon-to-be-born son, crossfitting, doing DIY home-improvement projects, exploring national parks, or reading good nonmedical fiction with a cat or dog in his lap begging for his love and attention.
Malika Gill
Malika Gill is a 4th-year medical student at Virginia Commonwealth University pursuing internal medicine with interests in gastroenterology and medical education. She completed her undergraduate studies in biology and psychology at Virginia Commonwealth University. In her free time, she loves to read, try new restaurants, and spend time with friends and family.
Episode 148: Antiracism in Medicine Series Episode 4 – Dismantling Race-Based Medicine Part 2: Clinical Perspectives
Dec 16, 2020
This is the second episode of a three-part series on understanding and dismantling race-based medicine. We invite Drs. Nwamaka Eneanya and Jennifer Tsai to discuss the limitations and harms of race-based medicine in clinical practice. Our guests explain how we can incorporate race-conscious medicine in clinical settings, medical education, and biomedical/epidemiological research to responsibly recognize and address the harms of racial inequality.
Learning Objectives
After listening to this episode learners will be able to…
Explain how race-based medicine harms our ability to provide equitable care for all
Understand the role of race in eGFR and other clinical calculators and the challenges of teasing out its role
Describe what clinicians can do to identify race-based medicine and how they can adapt their practices to mitigate the potential harms of race-based medicine
Explain the roles of medical education and biomedical/epidemiological research in accurately describing and justly addressing differences in clinical outcomes that stem from racial inequality
Understand why race-conscious medicine–not colorblindness–is how we should move forward and beyond race-based medicine
Credits
Written and produced by: Utibe R. Essien, MD, MPH, Naomi Fields, Rohan Khazanchi, LaShyra Nolen, Michelle Ogunwole, MD, Chioma Onuoha, Dereck Paul, MS, and Jazzmin Williams
Hosts: Utibe R. Essien, MD, MPH, Rohan Khazanchi, and Jazzmin Williams
Show Notes: Naomi Fields
Infographic: Creative Edge Design
Guests: Nwamaka Eneanya, MD, MPH, Assistant Professor of Medicine at the Hospital of the University of Pennsylvania (@AmakaEMD) and Jennifer Tsai, MD, MEd, Yale Emergency Medicine Class of 2023 (@tsaiduck77)
Episode 4 – Race-Based Medicine, Part 2: Clinical Perspectives
Show Notes
Naomi F. Fields
Time Stamps
00:00 Mission, vision, and introductions of hosts
01:30 Background on three-episode series
02:26 Introductions of guests
04:16 How Dr. Eneanya has seen race-based medicine play out in clinical practice
07:19 How Dr. Tsai has seen race-based medicine play out in clinical practice
10:45 What role should race play in making clinical decisions?
13:16 Status of the current conversation on removing race from eGFR calculators: why is it so contentious?
19:05 Clarifying the “ethics vs science” argument and critiquing research techniques
22:00 Resurgence of race-based speculation in COVID-19-related research
25:57 Implantation of ideas about innate racial inferiority within medicine
28:32 Will removal of race from algorithms potentially harm our patients?
33:19 Danger of normalizing immutable, innate racial difference within clinical algorithms
38:10 What role should race hold as we move toward health equity?
45:50 Key takeaways for trainees
47:45 Key takeaways for faculty
49:17 Pointers to those interested in health equity research
50:17 One thing you can employ in your practice today
54:14 Bloopers!
Episode Takeaways:
Trainees
Asking thoughtful questions that challenge the “status quo” can prove an effective means of sparking discussions while minimizing the potential for negative retaliation. Dr. Tsai describes previously asking her attendings, “Why is there a race correction for adults in nephrology, but not for children? What happens at age 18 [to provoke the need for correction]?” Questions such as these can stimulate thoughtful inquiry and remind all of us of the responsibility to be critical practitioners.
Faculty
If you feel your cause is important, keep going — even when you are challenged by others. Attending physicians have tremendous power in dictating culture, and are so valuable in extending this work, especially given how the hierarchical nature of medicine can make it difficult for trainees to advocate firmly. Moreover, center patients not only in discussions about individual decision-making but in constructing and drawing meaning from the research.
All
If you are interested in health equity, recognize that there is a breadth of research established in the fields of health equity, disparities, and structural racism. Be sure to do the work to educate yourself about the foundations of this work, and collaborate with those who have been studying and establishing it if you have the opportunity.
Poet Marge Piercy has written, “The work of the world is as common as mud.” While there indubitably exists a need to advance scholarship and theory, we must also ground ourselves in the day-to-day actions that can bring comfort and kindness to our patients. Where can you give an extra inch to those for whom you are caring?
Pearls
Role of Race in Clinical Reasoning
Harnessing the idea that “race is a social construct” to exclude consideration of race from medicine altogether does a disservice to our patients. Race, racism, and racial inequality have tangible impacts on people’s livelihoods, much less their experiences in the healthcare system. For instance, there is well-established research on how the stress of racism and racial inequality become “embodied” by modifying people’s cortisol levels to exert end-organ effects. Thinking about race is not racist in and of itself: It is the usage of race in the service of white supremacy or oppression that makes that transformation. Being race-conscious, or critically curious about the ways in which racism and racial inequality may affect our patients, can actually offer a starting point for advancing health justice. Much is akin to how naming the “battered child syndrome” catalyzed changes in our frameworks for addressing child abuse, critical curiosity in the space of racism can help us to develop thoughtful plans for tracking, discussing, and monitoring racism within in healthcare settings and beyond.
Race in eGFR Calculations — Why So Contentious?
eGFR equation-building is a complex science. Returning to the early literature that informs the equations reminds us that this research demonstrated racially stratified differences between Black and white cohorts. However, these studies did not account for many of the factors that can impact creatinine, the main biomarker used in eGFR calculations. These factors include a high-protein diet, muscle mass, creatinine generation, and certain medications. Many of the Black participants in the CKD epi study came from an African-American cohort (ASK trial) in which 50% of participants hadn’t graduated high school and over 50% made less than $50,000/year. These factors may have impacted their diet, physical activity, and medications, thus impacting their creatinine levels and the inputs that we use for GFR. This reminds us that using race as a catch-all can shroud other factors (ex. structural racism) that more rigorously account for differences observed between groups. And, as we think about revamping eGFR calculators, we must also ensure that there are standardized means of doing so across institutions.
Ethics-Plus: Reforming our Approaches to Clinical Research
Without question, there exists a strong ethical imperative to eradicate racism from biomedical science and to better use biomedical science in the service of health justice. There also exists an imperative to refine how we use race in research, given the scientific evidence that it is a social construct. Critiquing the cursory usage of race in studies illuminates the need to clearly define and standardize race as an operational variable, explain that to which racial differences are attributed, and describe how we interpolate meaning from these differences. Failing to do so may obfuscate the realities of social-structural racism, and obscure opportunities for improving understanding or intervention. Rigorous usage of race is not only ethically sound: it’s also better science.
In this vein, our researchers can take advantage of the technology that we have to ask more sophisticated questions that generate true accuracy, rather than those that simply accept race as a surrogate. We might critically think about why we might use race in a regression model, and proactively consider how we will interpret and responsibly discuss findings that may result. We might group people across socio-demographic categories (ex. education, income, number of previous hospitalizations) that also lead to clinical outcomes, not only race-based stratification. When racial differences are observed, we might further examine contributors to outcomes within a group. Our journals can help lead the charge by more diligently enforcing fastidious usage of race within papers they choose to publish. Rather than accepting racially-stratified differences in outcomes as inexorable and without further inquiry, we can seek to understand and address what underpins these phenomena. Consensus standards that guide authors on ethical use of race in scientific research exist. Our esteemed publications should ensure that investigations that utilize racial variables follow these guidelines before being published.
Addressing Potential Harms of Removal of Race from Clinical Calculators
Some have expressed fear that removing race from eGFR calculators will result in inaccurate therapeutic changes (ex. premature dialysis initiation, premature renal transplants, or inappropriate medication administration) that will primarily affect Black patients. However, the diagnostic approach used to determine changes in clinical management of renal disease (i.e. dialysis, transplant) is multifactorial; it is not based on eGFR alone. Additionally, research has shown that using symptom-prompted modifications to management, in the context of shared decision-making, can improve outcomes. Using the eGFR calculators as a sole determinant offers a limited metric with a ~30% margin of error. We can and should be incorporating other methods of evaluating kidney function (ex. 24-h Cr clearance, cystatin C) within a body of data. This can contribute to a more holistic understanding of disease progression and management.
How Bearing the Burden of Change Reinforces Racism
Some responses to the prospect of eliminating race corrections have asked proponents of these changes to prove that removing race corrections will not do harm to patients. In juxtaposition, research that established the corrections was not necessarily asked to prove that corrections are harmless. The additional evidence and surveillance needed to demonstrate the limited relevance of race belies a collective investment in the immutability of biological racial difference. However, race corrections do in fact cause both ideological and tangible harm in that they reify essential biological racial differences. Social psychology research demonstrates that when race is given this genetic basis, trainees display more apathy toward racial outgroups and a tendency to consider their physiology as innately dysfunctional. As a result, they demonstrate lower levels of accountability to creatively problem-solve for patients of color. It is also the case that many of these race corrections (eGFR, ASCVD, UTI, VBAC) about which people have been protective have not actually shown benefit to people of color.
Tsai J, Ucik L, Baldwin N, Hasslinger C, George P. Race Matters? Examining and Rethinking Race Portrayal in Preclinical Medical Education. Acad Med. 2016 Jul;91(7):916-20. doi: 10.1097/ACM.0000000000001232.
Ahmed S, Nutt CT, Eneanya ND, et al. Examining the Potential Impact of Race Multiplier Utilization in Estimated Glomerular Filtration Rate Calculation on African-American Care Outcomes. J Gen Intern Med. 2020. doi: 10.1007/s11606-020-06280-5.
Additional references and papers as mentioned in the episode
Essien UR, Eneanya ND, Crews DC. Prioritizing Equity in a Time of Scarcity: The COVID-19 Pandemic. J Gen Intern Med. 2020;35(9):2760-2762. doi:10.1007/s11606-020-05976-y
Krieger N. Embodiment: a conceptual glossary for epidemiology. J Epidemiol Community Health. 2005;59(5):350-355. doi:10.1136/jech.2004.024562
Gravlee CC. How race becomes biology: embodiment of social inequality. Am J Phys Anthropol. 2009 May;139(1):47-57. doi: 10.1002/ajpa.20983. PMID: 19226645.
Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate [published correction appears in Ann Intern Med. 2011 Sep 20;155(6):408]. Ann Intern Med. 2009;150(9):604-612. doi:10.7326/0003-4819-150-9-200905050-00006
African American Study of Kidney Disease and Hypertension (AASK):
Lewis J, Agodoa L, Cheek D, et al. Comparison of cross-sectional renal function measurements in African Americans with hypertensive nephrosclerosis and of primary formulas to estimate glomerular filtration rate [published correction appears in Am J Kidney Dis 2002 Feb;39(2):444]. Am J Kidney Dis. 2001;38(4):744-753. doi:10.1053/ajkd.2001.27691
Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619. doi:10.1056/NEJMoa1000552
Lloyd-Jones DM, Braun LT, Ndumele CE, et al. Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease: A Special Report From the American Heart Association and American College of Cardiology [published correction appears in J Am Coll Cardiol. 2019 Jun 25;73(24):3234]. J Am Coll Cardiol. 2019;73(24):3153-3167. doi:10.1016/j.jacc.2018.11.005
Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci U S A. 2016;113(16):4296-4301. doi:10.1073/pnas.1516047113
Micheletti SJ, Bryc K, Ancona Esselmann SG, et al. Genetic Consequences of the Transatlantic Slave Trade in the Americas. Am J Hum Genet. 2020;107(2):265-277. doi:10.1016/j.ajhg.2020.06.012
Krieger N. Does racism harm health? Did child abuse exist before 1962? On explicit questions, critical science, and current controversies: an ecosocial perspective. Am J Public Health. 2003;93(2):194-199. doi:10.2105/ajph.93.2.194
Mr. Khazanchi is a member of the American Medical Association’s Council on Medical Education, but the views presented herein represent his own and not necessarily those of the AMA or the Council. Dr. Eneanya is a member of the National Kidney Foundation and the American Society of Nephrology Task Force; the views herein represent her own and not necessarily those of the NKF or the Task Force. The hosts and guests report no other relevant financial disclosures.
Citation
Eneanya A, Tsai J, Williams J, Essien UR, Paul D, Fields NF, Nolen L, Ogunwole M, Onuoha C, Khazanchi R. “Episode 4: Dismantling Race-Based Medicine, Part 2: Clinical Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes December 17, 2020.
Episode 147: BeaST sized Schema – Meningoencephalitis
Dec 14, 2020
Want to test your learning? Take our Episode Quiz here
Dhruv Srinivasachar
Dhruv Srinivasachar is a 4th year medical student at Virginia Commonwealth University School of Medicine (the Medical College of Virginia for all the veteran attendings out there). Introduced to medicine through research, Dhruv has shifted his passions to empathetic clinical care and medical education, as a contributor to the CPSolvers (especially through VMR as a case presenter, discussant, and compiler of cases) and team member for the Not Just Little Adults podcast (CPedsSolvers, if you will). When he’s not interviewing for Med-Peds residency, he can be found biking around Richmond, VA, gardening, and cooking.
Tahir Malik
Tahir Malik is a 4th-year medical student at Baylor College of Medicine interested in artificial intelligence, cardiology, and global health. He is interested in performing healthcare disparities research, in capacity-building in low-resource settings, and in understanding the role AI might play in global health solutions. In his free time, Tahir is an avid runner and biker and is trying to become a reasonable cook.
Travis Smith
Dr. Smith is a student educator and community EM physician currently practicing in Jacksonville, Florida. He currently is an Associate Professor of Emergency Medicine, Assistant Dean of Clinical Education, and the Director of the Clinical Clerkship Curriculum for LECOM. He attended undergrad at FSU where he received his bachelor’s degree in Biological Science. He then attended Lake Erie College of Osteopathic Medicine in Bradenton for his medical degree and then completed his residency in emergency medicine at the University of Florida Jacksonville campus. He has been board-certified in emergency medicine through ABEM since 2013. In his free time, he serves as the lead section editor for the Human dx project as well as a frequent contributor to the Clinical Problem Solvers and is heavily involved in #Medtwitter running the @medtweetorials account as well as his own @RosenelliEM
In this episode of Clinical Problem Solvers: Anti-Racism in Medicine, we sit down with Ed Yong, an award-winning journalist and science writer with The Atlantic, to discuss the structural inequities amplified by COVID-19 as well as the social concerns associated with the impending/present second wave of the pandemic.
Learning Objectives
After listening to this episode listeners will be able to…
Understand the trajectory of the COVID-19 pandemic’s unique impact on communities of color in the United States and its tie to historical discrimination and structural inequities
Describe the racialized and politicized national response to COVID-19
Recognize the crucial role that social interventions can and could have played in decreasing the burden of COVID-19
Credits
Written and produced by: Dereck Paul, MS, Utibe R. Essien, MD, MPH, Rohan Khazanchi, LaShyra Nolen, Michelle Ogunwole, MD, Naomi Fields, Chioma Onuoha, and Jazzmin Williams
Hosts: Dereck Paul, MS, Utibe R. Essien, MD, MPH
Infographic: Creative Edge Design
Guests: Ed Yong staff writer at The Atlantic (@edyong209)
Clinical Problem Solvers: Anti-Racism in Medicine
Show Notes – Episode 3: Structural Inequities and the Pandemic’s Winter Surge
December 3rd, 2020
By: Chioma Onuoha
Timestamps
00:00 Music/Intro
00:20 Mission and Vision
00:32 Introduction of Ed Yong
02:00 Disproportionate impact of COVID-19 on minority communities
04:00 Racism in the national/policy response to COVID-19
07:00 Health Care Worker Fatigue
09:30 Grief and the Unique Frustrations of Health Care Workers of Color
11:30 The “Chinese” Virus and the history of the pandemic
14:00 Administrative Blame Shifting
17:00 How Could This Have Been Prevented?
20:00 COVID-19 and indigenous populations
Takeaways
Social Interventions are Valuable
Currently in the COVID-19 pandemic, social interventions are the only interventions available to us. When it comes to pandemics more broadly, the role of non-pharmaceutical interventions, like mask wearing, social distancing, and stay at home orders, must be recognized for their robust potential to reduce disease spread and burden. (Reflection Question: How can I best communicate the importance of social interventions to my extended family, community, and patients?)
The Racial Disparities Exposed by COVID-19 are Not a Result of Biological Difference
It is dangerous to look at the racial and ethnic health disparities highlighted by COVID-19 and attribute them to biological differences*. Many of the populations who suffer from these disparities also suffer from structural inequity and historical discrimination which impact their quality of life and health outcomes. Marginalized communities have historically received the brunt of the blame when it comes to widespread pandemics without recognition of the role that structural factors play in creating and maintaining health inequity.
*To learn more about the danger of biological explanations for health disparities see the CPS Anti-Racism in Medicine three-part episode series Dismantling Race-Based Medicine. Part 1: Historical & Ethical Perspectives featuring Professor Edwin Lindo is available now.
Health Policy Must Target Structural Inequities
Inequities worsen if they are not specifically addressed in policy. Without intentional effort put into addressing the root cause of structural inequities, it is possible that interventions will cause more harm than good. (Reflection Question: How should the concept of equity vs. equity be applied in creation of health policy?)
Pearls
The disparities amplified by COVID-19 are not new or unsurprising
The narrative of COVID-19 being a “ great equalizer” is largely untrue. If anything, COVID-19 has removed “the veil” and made the extent of the inequities in this country very clear. Marginalized communities are especially vulnerable to COVID-19 due to structural factors like segregation, lack of access to clean water, poor air quality, and limited availability of health care. These structural inequities are longstanding and will require long-lasting and intentional rectification.
Frontline Workers Pushed to their Limits
Touching accounts from frontline workers, in particular, nurses, who are uniquely positioned to face the devastating impacts of the disease, have clarified the toll that COVID-19 has placed on care workers. The emotional and physical fatigue associated with such immense loss of human life is leading to burnout among the very group that is required to address this disease. For many health care workers of color, their struggles are compounded by personal grief and increased expectations to lead anti-racism efforts within institutional walls.
Blame shifting
During COVID-19, we have seen marginalized communities be positioned as scapegoats to explain the prevalence and persistence of the disease. This is not a new phenomenon. Ed Yong cites anti-Blackness during the Ebola outbreak; homophobia, transphobia, and condemnation of sex workers and people who use drugs during the HIV epidemic; and current anti-asian rhetoric during COVID-19 and the original SARS as examples. Blame is deflected to populations on the outskirts of society and used as justification to delay or fail to provide aid. Throughout the duration of the pandemic, we have seen the nature of this blame evolve. While it started with accusations that Black people and POC do not take the virus seriously and/or have chronic diseases and unhealthy habits, most presently it manifests through discourse around black people’s weariness of taking the forthcoming COVID-19 vaccine. Rather than placing blame on marginalized populations, it is crucial that we first analyze history and external influences that may explain the behaviors and outcomes being observed.
Overreliance on Biomedical Measures
“[Rudolf Virchow] specifically writes ‘Medicine is a social science’ and we have lost that understanding” – Ed Yong
For much of the COVID-19 pandemic, rhetoric in the United States has centered around waiting for biochemical and pharmaceutical interventions to be developed rather than fully taking advantage of the social interventions currently available. Social interventions are powerful, and as we can see from the COVID-19 responses of countries like South Korea and Taiwan, they are effective at managing this disease. This reality highlights the importance of sociological and anthropological expertise in medicine and the need to expand interdisciplinary exchange in health care more broadly.
Gross, C. P., Essien, U. R., Pasha, S., Gross, J. R., Wang, S., & Nunez-Smith, M. (2020). Racial and Ethnic Disparities in Population-Level Covid-19 Mortality. Journal of General Internal Medicine, 35(10), 3097–3099. https://doi.org/10.1007/s11606-020-06081-w
Krishnan, L., Ogunwole, S. M., & Cooper, L. A. (2020). Historical Insights on Coronavirus Disease 2019 (COVID-19), the 1918 Influenza Pandemic, and Racial Disparities: Illuminating a Path Forward. Annals of Internal Medicine, 173(6), 474–481. https://www.acpjournals.org/doi/full/10.7326/M20-2223
The hosts and guests report no relevant financial disclosures.
Citation
Yong E, Essien UR, Nolen L, Khazanchi, R, Ogunwole M, Fields N, Onuoha C, Williams J, , Paul D. “Episode 4: Structural Inequalities and a Second Wave.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes. December 3, 2020.
Want to test your learning? Take our Episode Quiz here
Kushal Vaishani
Kushal is a hospitalist and contributing editor for the Adult Medicine section at Human Dx. After finishing his medical school in India, he completed his residency training at Brandon Regional Hospital and LSUHSC – University Hospital and Clinics. His academic interests include clinical reasoning, medical education, high-value care, and infectious diseases.
Gabe Siegel
Gabe Siegel is currently a PGY-1 Emergency Medicine Resident at Denver Health. Gabe completed medical school at Rush Medical College in Chicago, IL. When not working, he is busy enjoying the outdoors in Colorado and hunting for good food in Denver. His academic interests include health policy, critical care, and social EM.
Jake Hershey
Jake is currently a PGY-1 in the IM hospital training track at the University of Colorado and graduated from Rush Medical College alongside his friend and co-discussant Gabe. His passions in medicine include medical education, clinical reasoning, and after-work commiseration with his co-residents. In his free time, he loves exploring the Colorado wilderness to experience the amazing hiking, kayaking, and snowboarding that the state has to offer.
Episode 143: Human Dx Unknown with Dan and UAB residents- headache in the time of COVID
Nov 23, 2020
Want to test your learning? Take our Episode Quiz here
Courtney Wagner
Courtney Wagner is PGY-2 in Internal Medicine resident at the University of Alabama at Birmingham. She is a Florida native and grew up in and around the water either swimming competitively, SCUBA diving, or fishing. She initially graduated from the University of Central Florida with a biological sciences degree and taught high school science before going back to school for nursing at the University of South Florida. After gaining experience at the bedside as an ICU nurse, she pursued a career in medicine by returning to UCF for medical school. Currently interested in academic medicine with a heart for hospice and palliative and the geriatric population. She loves cooking, hiking, and triathlons, having completed over 60 races, including Ironman Cozumel.
John Alexander
John Alexander is a PGY-2 internal medicine resident at the University of Tennessee Health Science Center in Memphis. He got his undergraduate degree in history from Rhodes College and graduated from William Carey University College of Osteopathic Medicine. His research interests include clinical and diagnostic reasoning and cardiology. He hopes to pursue a career in academic medicine. Outside of the hospital he enjoys playing tennis, traveling, and spending time with family and friends.
Ryan Goetz
Ryan Goetz is a second-year internal medicine resident at the University of Alabama Birmingham. He attended medical school at the Medical College of Georgia. He wants to pursue a career in pulmonary/critical care medicine after completing his residency. His clinical/research interests include ventilator physiology/teaching, clinical reasoning, bronchiectasis, and ARDS. In his spare time, Ryan enjoys Orange Theory Fitness workouts, craft beer, and history podcasts.
Episode 142: WDx # 5 – Clinical Unknown with Dr. Natasha Chida – Altered Mental Status
Nov 18, 2020
Sharmin, Lindsey, and Alex discuss a clinical unknown with Dr. Natasha Chida from Johns Hopkins
Want to test your learning? Take our Episode Quiz here
Dr. Natasha Chida
Dr. Chida is an Assistant Professor in the Division of Infectious Diseases at Johns Hopkins University School of Medicine. She serves as the Associate Program Director for the infectious diseases fellowship training program. She is also the Co-director of the Osler and Bayview Internal Medicine Residency Programs Medical Education Pathway, and firm faculty in the Osler Program, where she serves as a resident coach. Her research interests include career development for early-career professionals, women in medicine, and HIV education for fellows.
Episode 141: Antiracism in Medicine Series Episode 2 – Dismantling Race-Based Medicine Part 1: Historical and Ethical Perspectives with Edwin Lindo
Nov 17, 2020
This is the first episode of a three-part series on understanding and dismantling race-based medicine by unearthing its origin and exposing the paucity of rigorous evidence in support of it. In this episode, we invite Critical Race Theory scholar Edwin Lindo, JD to discuss the invention of race, how its definition has changed over time, and how the fields of science and medicine contributed to its legitimacy as a tool for political and social oppression.
Episode Learning Objectives
After listening to this episode learners will be able to…
Define race and what is meant by “race is a social construct”
Describe the influential role of science and medicine in creating race
Understand why race is a poor proxy for genetics or ancestry
Credits
Written and produced by: Rohan Khazanchi, LaShyra Nolen, Michelle Ogunwole, MD, Naomi Fields, Chioma Onuoha, Jazzmin Williams, Dereck Paul, MS, and Utibe R. Essien, MD, MPH
Guests: Prof. Edwin Lindo, Assistant Dean for Social & Health Justice, University of Washington School of Medicine (@EdwinLindo)
Time Stamps
00:00 Music/intro 00:11 Our mission and vision 00:38 Introduction to the Antiracism in Medicine team 02:08 Introduction of this episode and the Dismantling Race-Based Medicine series 02:49 Introduction of Prof. Edwin Lindo 03:28 What is race? How is race a social construct? Why was it constructed in the first place? 16:10 Why color-blindness is not a solution to dismantling race-based medicine 20:00 How has medicine played a key role in defining race throughout history? 37:50 Race vs. ancestry vs genetics–implications for research and clinical practice 52:02 What can we start doing tomorrow? 57:35 Conclusion and outro
Episode Takeaways:
History matters. Medicine has never been an apolitical field, and understanding the specific ways the medical field contributed to socio-political definitions of race through practices rooted in medical racism can help us avoid repeating the same harms of the past (e.g. racial essentialism). This education needs to span the whole MedEd continuum.
Definitions matter. In research, clinical practice, and MedEd, we need to be explicit in our understanding and discussion of race vs. ethnicity vs. ancestry, and how each of these categorizations does or does not impact biological or genetic traits.
Bias is everywhere. Objectivity is a top priority in medicine and research; however, history shows us how initial assumptions have tainted both study design and interpretation of results.
Conversation Starters and Reflection Questions for Trainees & Faculty
What teachings lie at the root of your belief that race has a biological basis? – Dismantling race-based medicine starts at home by asking yourself, colleagues, and
classmates this question. Much of the data promoting biological difference amongst races comes from poorly-designed studies where race as a variable is ill-defined or confounding variables are inadequately controlled. This reflexive acceptance that race is rooted in biology comes from stereotypes created by Carl Linnaeus and other racial taxonomists.
How is racism causing the outcomes that I am seeing in my patient? – Recognizing that racism, not race, is the root cause of racial health disparities is the first step to improving health outcomes for Black, Indigenouls People of Color (BIPOC) patients. Acknowledging this truth highlights the necessity of mitigating the harms of racism as part of any comprehensive treatment plan. This is done on an individual level, by offering existing support and resources, as well as on a systemic level through advocacy.
Pearls
Defining Race
Race is a socio-politically constructed taxonomy that was invented based on factors such as perceived skin color and culture, not science or biology. The concept of race emerged for the purpose of allocating and/or extracting resources. In the United States, the concept of race was key to extracting resources from Black and Indigenous peoples during the formation and expansion of the country.
The Role of Science and Medicine in Defining Race and Racism
Scientists and physicians legitimized race as a category by positing “objective” proof that white persons were biologically superior to other races. In 1735, Carl Linnaeus, often known as the the “father of taxonomy,” classified four “varieties” of human species and ascribed stereotypical characteristics to each race: “Native Americans as reddish, stubborn, and easily angered; Africans as Black, relaxed, and negligent; Asians as sallow, avaricious, and easily distracted; while Europeans were depicted as white, gentle, and inventive.”
In 1839, Dr. Samuel Morton asserted that White people were the most intelligent of all races and Black people were the least so based on head circumference and cranial capacity. In an 1850 report commissioned by the Louisiana legislature, Dr. Samuel Cartwright argued that Black people were lazier, less intelligent, and more susceptible to infectious diseases than White people because they had less lung capacity. Cartwright’s study influenced the equations that medical professionals still use to calculate the impact of various diseases on lung function. This baseless race correction impacts treatment decisions, which contributes to racial health inequities. In the early 1900s, eugenicists and social anthropologists claimed that Black people were predisposed to violent crime, which justified institutionalization and sterilization of Black people. Despite their claims being based on unproven assumptions, their research was praised for scientific rigor and used to justify subjugation based on race.
“The scientific method is only as strong as the variables you input into it and if you are not critical of the questions you are asking, who you are researching, how you are doing that research then the biases, the history, the legacy, they seep in.” – Edwin Lindo, JD
Why is color-blindness not a solution to dismantling race-based medicine?
Ignoring race and racism does not negate the profound impact that race and racism have on our BIPOC patients’ health. Colorblindness inflicts harm through erasure. Instead, researchers and clinicians must be aware of the impact of racism in order to explore ways of mitigating its damage. For more on this concept, stay tuned for the next episode!
Is race a good proxy for ancestry? For genetics?
Since race is a socio-political construct, its definition has changed over time and space. For example, racial categories in the US Census have changed numerous times, with new categories being created and others disappearing or returning depending on the political atmosphere at the time. In another example, a person who is considered Latinx in the US could be considered Mulatto in Brazil or Coloured in South Africa. Given that there is no standard definition of race, its imprecision does not meet the standards of clinical medicine. As Prof. Lindo states, “our eyes see race” when we study disease disparities, but the true risk factor may actually be racism, geographic ancestry, or a specific genetic variant. However, assuming a genetic difference based on a perceived association with race is poor science.
Links
References discussed throughout episode
“The Praxis” Podcast: https://clime.washington.edu/praxis
Boyd RW, Lindo EG, Weeks LD, McLemore MR. On Racism: A New Standard For
Publishing On Racial Health Inequities. Health Aff Blog. Published online July 2, 2020.
Tsai J, Cerdeña JP, Khazanchi R, Lindo E, et al. There is no “African American physiology”: The fallacy of racial essentialism. J Intern Med. 2020;288(3):368-370. doi:10.1111/joim.13153
Wilkerson, I. (2020). Caste: The Origins of Our Discontents. Random House.
Additional references and papers as mentioned in episode
Roberts, D. (2012). Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-first Century (50852nd ed.). The New Press.
Braun, L. (2014). Breathing Race into the Machine: The Surprising Career of the Spirometer from Plantation to Genetics (1st ed.). Univ Of Minnesota Press.
Harris, C. (1993). Whiteness as Property. Harvard Law Review, 106(8), 1707-1791. doi:10.2307/1341787
Williams DR. Miles to go before we sleep: racial inequities in health. J Health Soc Behav. 2012 Sep;53(3):279-95. doi: 10.1177/0022146512455804.
Disclosures
Mr. Khazanchi is a member of the American Medical Association’s Council on Medical Education, but the views presented herein represent his own and not necessarily those of the AMA or the Council. The hosts and guests report no other relevant financial disclosures.
Citation
Lindo E, Nolen L, Paul D, Ogunwole M, Fields N, Onuoha C, Williams J, Essien UR, Khazanchi R. “Episode 140: Dismantling Race-Based Medicine, Part 1: Historical & Ethical Perspectives.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes November 17, 2020.
Show Transcript
Music
Introduction
Introduction to the Antiracism in Medicine team
Introduction of this episode and the Dismantling Race-Based Medicine series
Introduction of Prof. Edwin Lindo
What is race? How is race a social construct? Why was it constructed in the first place?
Why color-blindness is not a solution to dismantling race-based medicine
How has medicine played a key role in defining race throughout history?
Race vs. ancestry vs genetics–implications for research and clinical practice
Jan Ramesh is the Hospital Medicine Fellow in Quality and Safety at Dell Medical School at The University of Texas at Austin. Outside of the hospital, she enjoys writing poetry, drawing, and spending time with her husband and her two cats.
Dr. Chris Moriates
Chris Moriates is a practicing hospitalist, Assistant Dean for Healthcare Value, and Associate Chair for Quality and Safety at Dell Medical School at The University of Texas at Austin, where he also directs the Distinction Track in Care Transformation for internal medicine residents and the Hospital Medicine fellowship. When not in the hospital, he most enjoys running around the lakes in Austin accompanied by his 9-year-old son on his bike, or hanging out with his 5-year-old daughter.
Dr. Steph Le shares a story of gender discrimination and Emma and Annette discuss gender biases and stereotypes with UCSF’s Department of Surgery Chair, Dr. Julie Ann Sosa
Dr. Julie Ann Sosa
Julie Ann Sosa, MD MA FACS is the Leon Goldman MD Distinguished Professor of Surgery and Chair of the Department of Surgery at the University of California San Francisco (UCSF), where she is also a Professor in the Department of Medicine and affiliated faculty for the Philip R. Lee Institute for Health Policy Studies. Dr Sosa came to UCSF in 2018 from Duke. Her clinical interest is in endocrine surgery, with a focus in thyroid cancer. She is an NIH-funded investigator and author of more than 325 peer-reviewed publications and 78 book chapters and reviews, all largely focused on outcomes research, health care delivery, hyperparathyroidism, and thyroid cancer, with a focus on clinical trials. She has authored or edited 7 books. Dr Sosa is Treasurer of the American Thyroid Association (ATA) and serves on the Board of Directors/Executive Council of the ATA and International Thyroid Oncology Group, as well as practice guidelines committees for the ATA, NCCN, and the American Association of Endocrine Surgeons; for the ATA, she is chairing the committee responsible for writing the next iteration of differentiated thyroid cancer guidelines. She is the Editor-in-Chief of the World Journal of Surgery and is an editor of Greenfield’s Surgery: Scientific Principles and Practice. She has mentored more than 90 students, residents, and fellows, for which she was recognized with induction as a full member to the American College of Surgeons Academy of Master Educators in 2020, and with the Lewis E. Braverman Distinguished Lectureship Award from the ATA in 2017. Dr Sosa was born in Montreal and raised in upstate New York. She received her AB at Princeton, MA at Oxford, and MD at Johns Hopkins, where she completed the Halsted residency and a fellowship.
Want to learn more about Women in Diagnosis (WDx) series?
Gizem Reyhanoglu is a 4th-year medical student at LECOM-Bradenton, applying to Internal Medicine this application cycle. She completed her undergraduate degree in biology at the University of Florida and completed a Master’s degree in Medical Sciences at the University of South Florida. In her spare time, Gizem enjoys watching The Office, training for half-marathon races, baking for her family/friends, and playing with her puppy, Leo.
Lily Tranchito
Lily Tranchito is a PGY-3 at Case Western Reserve University/University Hospitals Internal Medicine program. She was born and raised in Cleveland, Ohio, earned her undergraduate degree from The Ohio State University, and graduated from Ohio University Heritage College of Osteopathic Medicine. She has a passion for medical education, cooking, gardening, daily walks around her neighborhood, and spending time with her family and friends.
Patrick Kramer
Patrick Kramer is a PGY-3 in Internal Medicine at the Case Western Reserve University / University Hospitals Internal Medicine Residency Program in Cleveland, Ohio. Although he is originally just a kid from Akron, he took his talents to the University of Notre Dame and Loyola University Chicago – Stritch School of Medicine for his education. Career interests include pulmonary and critical care medicine as well as diagnostic reasoning and medical education. Outside of the hospital, Patrick has recently taken up disc golf in addition to his passions for coffee brewing, photography, and watching classic movies.
Episode 131: Human Dx Unknown with Sharmin & Ohio State residents – headache & myalgias
Oct 19, 2020
David Jessee is an assistant professor of medicine and academic hospitalist at Virginia Commonwealth University School of Medicine. He was born and raised in Southwest Virginia and completed his premedical and undergraduate education at the University of Virginia. After graduating from VCU School of Medicine, he remained in Richmond to complete his internal medicine residency training and subsequently joined the faculty in the division of hospital medicine. His interests include medical student and resident education with a focus on diagnostic reasoning and simulation-based experiences and assessment. Additionally, he is involved in efforts which recognize early signs of clinical decline and enhance inpatient emergency and code response. Outside the hospital, he enjoys running with his dog, biking, playing racquetball, watching UVA sports, and traveling to state and national parks.
Antionette Pusaterri
Antoinette Pusateri is a PGY-3 in Internal Medicine at The Ohio State University Medical Center. Born and raised in Columbus, Ohio she attended the University of Notre Dame for undergraduate majoring in Biology & Theology then returned to Columbus for medical school and Internal Medicine Residency at The Ohio State University College of Medicine and Wexner Medical Center. She is currently interviewing for Gastroenterology & Transplant Hepatology Fellowship and has a passion for research and quality improvement, medical education and community engagement. She is also a strong advocate for trainee wellness, and herself finds wellness in CrossFit and horseback riding.
David Deng
David Deng is a PGY-3 in Internal Medicine at The Ohio State University Medical Center. He spent most of his life around Atlanta, GA, went to medical school at Medical College of Georgia, but is feels right at home in the Midwest. He’s currently pursuing a career in academic hospital medicine and is passionate about clinical reasoning and medical education. In his spare time, he loves cheering on Liverpool FC, trying hole-in-the-wall restaurants, and staying active lifting weights and running.
Episode 130: Spaced Learning Series – Lactic acidosis
Oct 14, 2020
Melanie Fellay is the CEO and Co-Founder of Spekit, the leading in-app learning and digital enablement companion that helps employees learn their tools and navigate process changes by accessing training resources in real-time, everywhere they work. Founded in 2018, Melanie and co-founder and former colleague, Zari Zahra, created Spekit to address the pain points they felt around driving adoption and continuous training that many Enablement and Operations leaders feel as well by bringing the sophistication of a modern digital adoption platform with the simplicity of a contextual knowledge base.
She’s a Salesforce and BizOps enthusiast with expertise in leading operations and success teams, thinking at scale and architecting Salesforce solutions. In her role, Melanie oversees the sales, marketing, customer success, and corporate development teams at Spekit. Melanie graduated from the University of Colorado, Boulder with a degree in Accounting & Finance. In her free time, Mel enjoys seeing Odesza at Red Rocks, exploring less-traveled corners of the earth and escaping it all through meditation.
Zari Zahra
Zari is a Pakistani-American Harvard MBA, an experienced Product Manager and builder of web and mobile apps for Pandora, SquareTrade, RealtyShares and Rakuten. Today, she is the Chief Product and Technology Officer and Co-founder of Spekit, the leading Salesforce adoption and contextual learning platform for growing orgs. Zari oversees all product and engineering departments, including a team office located in Karachi, Pakistan.
In her free time, Zari spends time listening to audio books and spending time with her husband and mini-goldendoodle Rumi.
Episode 126: Human Dx Unknown with Arsalan & medical students, Alec and Fran – vision loss
Sep 24, 2020
Francesca Siegel is a third year medical student at The Ohio State University College of Medicine. She received her masters in Nutritional Sciences from the University of Cincinnati. She’s passionate about preventive medicine, effective science communion, public health, and serving her community. Outside of her school work, she enjoys volunteering with Clinica Latina, OSU’s Hispanic free clinic, running with her husband, travel, and cooking.
Alec Yu
Alec is medical student at the University of British Columbia in Vancouver, Canada. Prior to med school, he’s worked as an innovation officer at one of Vancouver’s tertiary care hospitals, and has served as a director and co-founder of a non-profit organization supporting youth engagement with humanitarian issues. A passionate problem-solver, Alec loves combining his interests with his lived experiences to start grassroots initiatives in his community. His current projects include investigating improvements to medical respite care for patients facing homelessness, and designing solid waste reduction strategies for improved hospital sustainability. On his down time, he loves cooking, running, and trying not to kill his plants.
Varun Phadke
Varun Phadke is an Assistant Professor in the Division of Infectious Diseases at the Emory University School of Medicine. He is involved in microbiology and infectious diseases education for medical students, residents, and fellows, and his scholarly interests include subspecialty clinical reasoning and diagnostic error. He loves cooking, reading mystery novels, and spending time with his wife and son.
Episode 125: Human Dx Unknown with Sharmin and & medical students, Vivek and Joshua – Diarrhea
Sep 22, 2020
Josh is a proud cat dad to four kitties and a fourth year student at Dell Medical School applying Medicine-Pediatrics. He spent his third year doing an MA in design that cemented his passion for using creativity and innovation to better deliver care and information to patients and providers. In his spare time, he is active on MedTwitter (#MP4L), loves to run and be outside, and is obsessed with podcasts and audiobooks.
Vivek Nair
Vivek Nair is a second-year medical student at the University of Chicago Pritzker School of Medicine. He spent his undergraduate years at the University of Michigan. He is an avid runner and has been recently practicing his culinary skills (just in case medicine doesn’t work out).
Joshua Inglis
Dr Josh Inglis is an aspiring General Physician training at the Royal Adelaide Hospital. He obtained his medical degree from the University of Adelaide and is studying towards a Masters of Clinical Education. His academic interests include clinical reasoning, drug allergy and the electronic health record. Outside of work he enjoys playing tennis, brewing specialty coffee and walking his golden retriever.
Dr. Stephanie Sherman is a hospitalist and residency associate program director at Baylor College of Medicine (BCM) who rounds at Ben Taub General Hospital and Houston’s VA hospital. She went to medical school at the University of Michigan and did internal medicine residency at Massachusetts General Hospital. She spends her free time with her husband, fellow clinical problem solver Zaven Sargsyan, and their ever-more-mobile 8-month-old son.
Problem Representation A 35-year-old man with advanced HIV/AIDS complicated by a recent diagnosis of Pneumocystis pneumonia and cytomegalovirus esophagitis presented with progressive fevers, dyspnea, and worsening pulmonary infiltrates in the weeks after starting antiretroviral therapy.
Schemas The CPSolvers’ schema for dyspnea highlights the relative importance of the pulmonary and cardiovascular systems before considering other etiologies.
Diagnosis The patient was found to have extensive bilateral consolidations on computed tomography of the chest. Laboratory evaluation demonstrated an elevated alkaline phosphatase, an increase in his CD4 count from 22 to 43 per cubic millimeter, and a reduction in his HIV viral load from > 1 million to 3000 copies. Ultimately, a respiratory culture from his prior admission grew Mycobacterium avium complex, raising the question of whether direct infection with this pathogen or an inflammatory reaction to it in the setting of immune reconstitution could account for his clinical deterioration.
Teaching points
Mycobacterium avium complex (MAC) is the most common of the nontuberculous mycobacteria (NTM) that acts as a human pathogen. Clinical manifestations are varied, most typically presenting as a chronic pulmonary infection in immunocompetent individuals and either localized (e.g., affecting the lymph nodes or other focal sites) or disseminated infection in immunocompromised patients (especially those with HIV infection). In the early HIV epidemic, disseminated MAC was the most common bacterial opportunistic infection and conferred significant morbidity and mortality even with treatment.
The immune reconstitution inflammatory syndrome (IRIS) is a potential complication of antiretroviral therapy (ART), wherein patients with advanced immunosuppression related to HIV develop an inflammatory response (generally to microbial antigens) as their immune system recovers. The two main types of IRIS are (1) paradoxical IRIS, in which a patient with a known opportunistic infection on appropriate therapy appears to deteriorate clinically after starting ART, and (2) unmasking IRIS, in which a previously silent opportunistic infection becomes clinically apparent due to the newly present immune response. IRIS to MAC most commonly presents with peripheral lymphadenitis, pulmonary-thoracic manifestations, or intra-abdominal findings.
Female physicians face many challenges in the clinical environment. Among the most frequently experienced microaggressions is “role misidentification,” or incorrect identification of an individual’s contribution to the health care team (e.g., assuming a female physician is a nurse). It has been suggested that frequent role misidentification (both on the part of patients as well as other healthcare team members) can lead to anxiety and a loss of sense of professional credibility among female trainees.
A pilot study recently demonstrated that distribution of new staff badges with the occupational title prominently displayed (i.e., reading “Doctor”) led to a significant improvement in role identification.
Additionally, others have suggested that a more deliberate use of professional titles (i.e., introducing female physicians as “Dr. X”) may also serve to combat stereotype threat and role misidentification.
Episode 120: Antiracism in Medicine Series Episode 1 – Racism, Police Violence, and Health
Aug 25, 2020
We invite scholars and antiracism activists, Drs. Rhea Boyd and Rachel Hardeman, to discuss the meaning of structural racism, the health impacts of police violence, the “say her name” movement, and the ways we can ensure our country’s current antiracist movement grows beyond a moment.
Learning Objectives
After listening to this episode learners will be able to…
Define structural racism
Understand how police violence is a social determinant of health
Explore the relationship between policing and healthcare
Explore and employ strategies to dismantle structural racism in clinical practice
Credits
Written and produced by: Naomi Fields, Rohan Khazanchi, LaShyra Nolen, Michelle Ogunwole, MD, Chioma Onuoha, Dereck Paul, MS, and Utibe R. Essien, MD, MPH
“First do no harm and while you’re doing no harm, learn as much as you can.” -Dr. Rhea Boyd.
Practitioners who benefit from the racist power structures existent in America must examine the waysthey benefit from or ignore racism in their workspaces and beyond. Then we must all commit to dismantling racism with tangible policy change.
Trainees
We encourage trainees to reflect on the ways they have been socialized to learn and think about racism in our country. Trainees may use this foundation to question how this might impact their medical education and think about this educational legacy may be reformed through curricular and structural changes at their institutions.
Faculty
Regardless of specialty or field, it is important all educators and clinicians do the work of understanding how racism is pervasive within their respective areas of expertise. This starts with self-education and a commitment to speak up when blatant examples of racism come up in the work space and beyond.
Pearls
Defining Structural Racism
Structural racism is a term that acknowledges that racism is perpetuated beyond individual interactions and interpersonal racism, but is present in the systems and policies that govern our everyday lives. These policies and decisions are often rooted in a historical legacy of white supremacy that have led to the systematic disadvantage of racial minorities in our society. Public health advocate, leader, and scholar, Dr. Camara Phyllis Jones, is credited for creating the framework many healthcare professionals and researchers use to think about systemic racism’s impacts on Black health. Her definition centers the idea that Black individuals did not inherit the diseases they disparately suffer from, but they inherited a disadvantaged system that creates the stark health disparities we see today. It is important to understand this unequal system negatively impacts everyone and every aspect of our society.
Policing and health outcomes
Evidence has shown that excessive policing not only impacts the individual health of Black and brown people who’ve interacted with the police, but it also impacts the health of their communities at large. Heightened police presence in communities of color can be perceived as a threat by community members which can result in sustained increases in stress and cortisol levels. This pathologic process can lead to adverse health outcomes affecting the cardiovascular, neurological, and endocrine systems.
Police brutality
Police brutality should be thought of as the ways state-sanctioned violence leads to the physical, psychological, and emotional harm of its victims. It is important to understand that police brutality not only impacts individuals with direct relationships to those afflicted by this violence but also has widespread effects on the entire Black community. It impacts the health of our colleagues who constantly have to witness this injustice play on television, often without consequence. It also leads to decreased productivity in Black communities as they deal with the aftermath and ongoing challenges of police brutality.
#SayHerName Campaign
As we continue conversations around police brutality, antiracism, and health equity, we must remember to not exclude women, children, the LGBTQ community, and the disabled community, among other communities of intersecting marginalized identities who continue to be impacted by police brutality. Social media and public response to police brutality traditionally center cis-gendered men, but people like Breonna Taylor, Tony McDade, and Tamir Rice, along with so many others, need our voices too.
Policing in Schools and Hospitals
Health care systems must actively advocate and protect their patients and that means we have to also reevaluate the presence of police in our spaces. This includes thinking about our roles as mandated reporters and police presence in emergency departments. Police presence in medical spaces can add to Black patients’ feelings of not having a “safe space” and we must consider our roles in potentially perpetuating violence in this way.
The hosts and guests report no relevant financial disclosures.
Episode Citation
Boyd R, Hardeman R, Ogunwole M, Fields N, Khazanachi R, Nolen L, Onuoha C, Paul D, Essien UR. “#120 Racism, Police Violence, and Health.” The Clinical Problem Solvers Podcast. https://clinicalproblemsolving.com/episodes/ August 26, 2020.
Episode 117: Human dx unknown with Sharmin and Baylor residents – Leg weakness and difficulty swallowing
Aug 18, 2020
Cyrus is a PGY-3 internal medicine resident at Baylor College of Medicine. He loves sports, hip-hop, exploring new restaurants and coffee shops, and writing. He’s an aspiring hematologist/oncologist with a passion for medical education.
Ruchit Rana
Ruchit Rana is currently a third-year internal medicine resident at Baylor College of Medicine. Ruchit completed medical school at Baylor College of Medicine. He has a passion for practicing and improving medical education at all levels. In his free time, he enjoys cooking and baking dishes across all ethnicities and maintaining his multiple freshwater aquariums at home. He is a proud co-founder of the Schema Squad alongside his co-resident, Cyrus Iqbal.
Krishan Sharma
Krishan Sharma is currently an internal medicine resident at Massachusetts General Hospital. He earned his medical degree at Harvard Medical School, where he also pursued a Masters in Medical Sciences in medical education. His academic interests include cardiology, critical care, and clinical reasoning. His hobbies include basketball, drumming, and entering spice eating competitions.
Episode 116: Human dx unknown with Arsalan and Wake Forest residents – Nasal congestion and rigors
Aug 17, 2020
Dr. Meredith Lash-Dardia is an internist at Weill Cornell Medical Associates in NYC. She graduated with a BA from Rutgers University and an MD from Rutgers Medical School (formerly UMDNJ). She did her training at Mount Sinai in NYC. Her areas of interest include preventative wellness, medical student teaching, as well as quality and patient safety initiatives. In her spare time, she works on local political campaigns and is involved in grassroots activism
Dr. Taylor Brooks
Taylor Brooks is in his third year of residency at Wake Forest School of Medicine’s Internal Medicine Residency (let’s go Deacs!). Originally from Ohio, Taylor spent his college years at The Ohio State University (let’s go Bucks!). He then completed medical school at the University of Cincinnati College of Medicine (let’s go Bearcats!). Aside from loving all of his alma maters equally, Taylor’s professional goals are to become a physician scientist, researching blood cancers and treating the patients who have them. He also hopes to one day teach the joys of academic hematology to internal medicine residents. In his free time, Taylor enjoys traveling the world with his amazing wife Cassandra, and throwing a ball around with his awesome Bernedoodle, Winston
Dr. Sarah Maus
Sarah Maus is currently a third year Internal Medicine resident at Wake Forest School of Medicine. She grew up in Springfield, IL before heading to Lexington, KY to complete undergraduate and medical school. She will be staying at Wake Forest next year as a Chief Resident, and hopes to pursue Hematology Oncology fellowship after her chief year. Outside of medicine, Sarah enjoys hiking in the mountains of North Carolina, playing tennis with friends, and spending quality time with family and her dog, Mila.
Episode 115: Spaced Learning Series – Abdominal pain and jaundice
Aug 13, 2020
An elderly woman with a history of progressive weakness, falls, and recently diagnosed ascites presented with weight loss and functional decline. Her workup was notable for ascites with a low serum-ascites albumin gradient (SAAG), thrombocytosis, and imaging evidence of peritoneal enhancement with omental nodularity and multiple pancreatic lesions. Biopsies of the peritoneal nodules were initially unrevealing for infections or solid malignancies. Ultimately, further tissue examination revealed primary peritoneal mesothelioma. The patient was not started on treatment and passed away one month later.
Teaching Points
The most common causes of low SAAG ascites include malignancy and infection. Malignancy can cause low SAAG ascites via peritoneal carcinomatosis (seen most commonly ovarian, bladder, or gastric cancer) as well as peritoneal mesothelioma. Tuberculosis is an important and difficult to diagnose infectious cause of low SAAG ascites. Ascitic fluid often reveals a lymphocytic predominance with elevated protein. Additionally, an elevated ascitic adenosine deaminase level (ADA) can suggest peritoneal tuberculosis
Asbestos exposure can lead to an array of benign and malignant diseases. Manifestations within the pulmonary parenchyma include asbestosis (a form of diffuse pulmonary fibrosis resulting in interstitial lung disease) and lung cancer (both small cell and non-small cell lung cancers). Pleural complications of asbestos exposure can include pleural effusions, pleural plaques, and malignant mesothelioma. Rarely, asbestos-related complications can occur in extra-pulmonary sites and present as peritoneal mesothelioma, with diffuse peritoneal nodules and low-SAAG ascites.
Episode 112: Virtual Morning Report #100 with Rabih, Reza, and Dr. Rezigh – Rash and lactic acidosis
Aug 03, 2020
A 75-year-old-woman with multiple chronic medical problems presented with right arm pain, anorexia, and diffuse erythematous nodular plaques. Her work up was notable for an elevated serum lactate and S1Q3T3 pattern on ECG. Computed tomography of the chest, abdomen, and pelvis demonstrated a right pleural effusion as well as nodular soft tissue thickening surrounding the right atrium extending to the interatrial septum with local mass effect and narrowing of the superior vena cava. Biopsy of her rash revealed abnormal lymphoid proliferation. Further studies led to a diagnosis of diffuse large B-cell lymphoma (DLBCL) with prominent cutaneous manifestations.
Teaching Point
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin’s lymphoma and can have a diverse range of manifestations. Most often, patients present with a rapidly enlarging mass and/or systemic “B-symptoms” (e.g., fever, night sweats, weight loss). Laboratory abnormalities classically include elevated lactate dehydrogenase levels, which occur in >50% of patients. In a minority of patients (about 40%), DLBCL presents in extramedullary and extranodal locations, including the soft tissues, lung, endocrine organs, and central nervous system. Diagnosis requires histologic examination and immunophenotyping (flow cytometry, immunohistochemical staining).
Bryce Montane is a Floridian born and raised! He went to University of South Florida as part of the 7-year medical program for undergraduate and medical school. He is now a PGY-3 Internal Medicine resident at the Cleveland Clinic. He is part of the inaugural Clinician Educator Track. He will be staying at the Cleveland Clinic next year as a Chief Resident and will then be pursuing a career in academic medicine.
Dr. Saja Almaaitah
Saja Almaaitah was born and raised in Jordan and graduated from the University of Jordan school of medicine. She then moved to the United States and joined Cleveland clinic for her internal medicine residency. During which, she was part of the clinical research scholar track. She has recently graduated residency and joined the rheumatology department at Cleveland Clinic. She hopes to pursue a career in academic medicine and research. In her free time, she enjoys hiking, reading and cooking.
Dr. Elizabeth Hastie
Elizabeth (Lizzy) Hastie is currently a third year internal medicine resident at UCSD. She completed her undergraduate education at the University of Colorado Boulder, and she attended Emory University for medical school. Lizzy is a member of the Resident as Clinician Educator (RACE) track at UCSD and will be a Chief Medical Resident for the 2021-2022 academic year. She is interested in pursuing an infectious disease fellowship following her chief year.
Episode 106: Human dx unknown with Arsalan and Duke residents – cough, dyspnea, & AMS
Jul 20, 2020
Alexandra Rojek is currently an internal medicine resident at the University of Chicago, interested in pursuing hematology/oncology with an interest in translational research. She attended Harvard University for her undergraduate education in chemical and physical biology, and then medical school at UCSF. During medical school, she developed an interest in medical education, particularly in her research on implicit bias in medical student evaluations. She has always had an interest in diagnostic reasoning and loves being a contributing editor at the Human Dx Project, and is excited to work with CPSolvers on sharing this case!
Dr. Micah Schub
Micah Schub is a third year internal medicine resident at Duke. He grew up in Los Angeles, CA and got his undergraduate degree in (slapping the) Double bass performance at the Juilliard School and a masters at the Manhattan school of music. He returned to LA to play in Cirque du Soleil’s “Iris” for a couple years before making a sharp turn and attending University of Pittsburgh School of Medicine. He is interested in nephrology, clinical reasoning and medical education. Outside of work, you can find him playing sweet tunes with his residency Weezer cover band “Wheezer.”
Dr. Stacy Bagrova
Stacy grew up in Donetsk, Ukraine and was lucky enough to move to the US just in time for college. She completed medical school at the University of Florida (Go Gators!). Currently, she is trying to learn as much as possible and provide lots of (mostly unsolicited) teaching to junior learners as a third-year medicine resident at Duke University Medical Center. Her ideal career combines clinical rheumatology and medical education focused on diagnostic reasoning. In her free time, she loves to get lost in a good mystery novel, cook or bake while tuning in to one of her favorite podcasts, or go for a run, listening to a 70s-80s classic rock mix.
Anna Costello is a Pediatric Hospitalist at the Children’s Hospital of Philadelphia, where she completed her residency and chief residency. Her interests within Medical Education include clinical reasoning and linguistically and culturally competent care. Outside of the hospital, she is an avid reader, painter, and soccer player.
Dr. Gurpreet Dhaliwal
Dr. Dhaliwal is a clinician-educator and Professor of Medicine at the University of California, San Francisco. He is the site director of the internal medicine clerkship at the San Francisco VA Medical Center, where he teaches medical students and residents in the emergency department, urgent care clinic, inpatient wards, outpatient clinic, and morning report. His academic interests are the cognitive processes underlying diagnostic reasoning and clinical problem-solving and the study of diagnostic expertise. Dr. Dhaliwal enjoys playing pickup basketball with his two sons … even though both can handily defeat him
Episode 103: RLR #9 – Abdominal Pain
Jul 02, 2020
Episode description
Reza and Rabih tackle a case of abdominal pain.
These additional episodes will be available on Patreon only.
Jenny was born and raised on Bainbridge Island in Seattle, Washington. She attended Haverford College where she studied religion and theoretical chemistry; ultimately staying in the Philadelphia area to attend the University of Pennsylvania School of Medicine. There, she developed an interest in behavioral economics and decision making, particularly in the critical care setting. She completed her internal medicine training at NYU and is staying on as a Chief Resident.
Dr. Greg Rubinfeld
Greg is currently a chief resident at NYU Grossman School of Medicine.He aspires towards a career in academic cardiology where he hopes to find a marriage of his interests in thrombosis and coronary artery disease.When he is not in the hospital or at home with his wife and son, you might find him scuba diving wrecks along the east coast, nose deep in classic literature, or playing pick-up street hockey and collecting more bruises than he cares to admit.
Dr. Ryan Haran
Ryan grew up in Oregon and after attending Oregon State University went to medical school at Virginia Commonwealth University in Richmond, Virginia.He completed an internal medicine internship then spent a year as a radiology resident at Northwestern University in Chicago, Illinois before deciding that while radiology is cool and all he had learned too much medicine to just go and forget everything. As such, he decided to return to medicine and has now completed an internal medicine residency at his home institution of VCU where he will be staying on faculty as a hospitalist.
Case Recap
A 55-year-old previously healthy woman presented with subacute abdominal distension and acute emesis. On examination, she was found to be hypotensive and hypoxemic with evidence of ascites. Laboratory evaluation was notable for severe transaminase elevation (AST 2500, ALT 1300), leukocytosis to 53,000 per cubic millimeter, hemoglobin of 20 mg/dL, and a mildly elevated erythropoietin level. Imaging demonstrated an acute portal vein thrombus as well as a right-to-left intracardiac shunt. A bone marrow biopsy revealed trilineage hypercellularity with an erythroid predominance and JAK-2 positivity. The ultimate diagnosis was polycythemia vera with a secondary EPO-dependent polycythemia (likely secondary to her intracardiac shunt).
Teaching points
An absolute erythrocytosis refers to elevation in the red blood cell (RBC) mass and can be due to primary bone marrow, secondary (e.g., hypoxia, erythropoietin secreting tumors), and congenital etiologies. A key branch point is evaluation of the erythropoietin level (the primary stimulus for RBC synthesis), with normal/suppressed levels suggesting the presence of a primary or congenital disorder. Polycythemia vera (PV) is the most common primary erythrocytosis and lies on the spectrum of myeloproliferative neoplasms. Thrombosis and bleeding are life-threatening complications.
Episode 101: Human Dx unknown with Sharmin & BMC/Brigham residents – Abdominal pain, dyspnea & confusion
Jun 29, 2020
Amir Gilad is a PGY-1 (very soon to be PGY-2!) at Boston Medical Center. Born and raised in Toronto, he attended Boston University for medical school and loved it so much that he stayed on for his internal medicine residency. He’s an aspiring cardiologist who is passionate about medical education. Outside of medicine he enjoys cheering on his beloved Toronto sport teams, jogging along the Charles River, and exploring the beautiful city of Boston.
Hannah Chen
Hannah Chen is a second year internal medicine resident at the Brigham & Women’s Hospital. She graduated from the University of North Carolina School of Medicine. She has an interest in hospital medicine, nephrology, and health equity. In her spare time, she enjoys eating/cooking and hiking.
Leela Chockalingam
Leela Chockalingam grew up in Rochester, NY. She studied Chemistry at Carnegie Mellon University and then attended medical school at the Icahn School of Medicine at Mount Sinai in New York City. During medical school, she spent a year in Vietnam doing tobacco use treatment research. She is currently an Internal Medicine resident at the University of Colorado in Denver, CO. She is interested in pursuing pulmonary critical care fellowship, and would ultimately love to be a clinician educator focused on clinical reasoning and evidence based medicine. Her hobbies include reading fiction, being outside, and cooking for family and friends.
Case recap
A 47-year-old man with alcohol and meth use presented with acute dyspnea, abdominal pain, and encephalopathy, and was found to be in acute congestive heart failure with atrial fibrillation and rapid ventricular rate. While in the emergency department, his oxygen requirement rapidly increased and he required intubation for hypoxemia and airway protection. Further evaluation revealed a suppressed thyroid stimulating hormone with an elevated free T3 and free T4, confirming a diagnosis of thyrotoxicosis meeting criteria for thyroid storm.
Teaching points
Hyperthyroidism refers to increased synthesis and release of thyroid hormones from the thyroid gland, whereas the term “thyrotoxicosis” represents the clinical syndrome produced by excess circulating thyroid hormone. The most common causes of hyperthyroidism include Grave’s disease, toxic nodular goiter/adenoma, and drug induced thyroid dysfunction. Thyrotoxic states can also occur when thyroid hormones are released from an injured thyroid gland in thyroiditis (autoimmune, viral, suppurative) or ingestion of exogenous thyroid hormone.
The clinical manifestations of hyperthyroidism can result from the thyrotoxic state itself (e.g., palpitations, fatigue, tremor, weight loss) or be related to the underlying cause of hyperthyroidism (e.g., grave’s ophthalmopathy, globus sensation/dysphagia from enlarged goiter). Complications of thyrotoxicosis include atrial fibrillation (with possible heart failure), thyrotoxic periodic paralysis, osteoporosis, and reproductive issues. Thyroid storm represents life-threatening thyrotoxicosis and its diagnosis is supported by the Burch & Wartofsky Score, which takes into account temperature, central nervous system effects, gastrointestinal/hepatic dysfunction, cardiovascular dysfunction, and the presence/absence of a precipitating trigger.
Episode 100 – Juneteenth The H&P – History and Perspective – Stories and Conversations with Dr. Kimberly Manning and her Dad, Mr. William Draper, Sr
Jun 19, 2020
Dr. Kimberly Manning and her father, Mr. William Draper, commemorate Juneteenth, the holiday that celebrates the day when all remaining enslaved Black Americas were freed in Galveston Texas, on June 19th, 1865, with this hour-long storytelling event.
Brady is a PGY 3 at Mercy Health in Muskegon, MI. Next year, he will be doing a fellowship in pulmonary & critical care in Colorado. His favorite thing about internal medicine is is the profound sense of accomplishment he feels when replacing electrolytes that are just slightly below the normal range.
Dr. Aaron Sabal
Aaron was born and raised in Westland, MI (Detroit metro area). He went to Wayne State University for my undergraduate studies thinking he would be a physical therapist, massage therapist, and dietitian (yes, all three of those). However, about one week prior to starting my massage therapy program, he had an epiphany and decided to go to medical school instead. He was fortunate to be accepted to MSUCOM and fell in love with Internal Medicine. His passions include all things medical. In particular, he is passionate about medical education, how best to help physicians learn, diagnostic reasoning, and creating an environment of learning where no one is afraid to express what they’re thinking. When he is not pursuing his love of learning, He is spending time with his wife and their boys (2 cats and a dog), playing with his animals, doing DIY home-improvement projects, exploring national parks, or reading a good non-medical book with a cat or dog in his lap begging for his love and attention.
Dr. Julia Burns
Julia is currently a geriatrics fellow at Mount Sinai Hospital in Manhattan. She earned her undergraduate degree from Fairfield University. She then went on to obtain a master of science in biomedical sciences from New York Medical College followed by her medical degree at Albany Medical College. She completed her internal medicine residency at NYU Winthrop Hospital on Long Island. Her academic interests include medical student and resident education.
Episode 94: Human Dx unknown with Arsalan & Utah residents – ankle and hand pain with swelling
May 25, 2020
Marja is a chief medical resident at the University of Utah. She is originally from Chicago, IL and received her undergraduate degree from the University of Wisconsin-Madison (go Badgers!). She then moved back to Chicago for medical school at Loyola University Stritch School of Medicine. In her free time, you can find her traveling with her husband in their camper van, rock climbing with friends, tending to her garden or listening to the Clinical Problem Solvers! Next year she is excited to stay on at the University of Utah as an academic hospitalist.
Dr. Guinn Dunn
Guinn is a first year Internal Medicine resident at the University of Utah. She was born and raised in Salt Lake City, received her undergraduate degree at the University of Puget Sound, then headed back to Utah for medical school and residency. She is interested in academic hospital medicine and quality improvement. She enjoys skiing, backpacking, and is looking forward to the birth of her first kiddo in a few weeks.
Dr. Kavea Panneerselvam
Kavea Panneerselvam is about to complete her intern year at Baylor College of medicine in Houston, TX. She grew up in the Houston area and completed her undergraduate at the University of Texas at Austin and is a proud Longhorn, and obtained her medical degree at UT Houston. After residency she hopes to pursue a career in gastroenterology. Specifically, she has an interest in IBD. In her free time she enjoys playing board games, discovering new movies, and making art for her friends and family. 
Marc Heincelman is an assistant professor within the Department of Medicine at the Medical University of South Carolina, where he also serves as director of the Medicine Clerkship and Acting Internship. He received his undergraduate degree from the University of Pittsburgh, medical degree from Loyola University of Chicago, and completed his combined internal medicine/pediatrics residency at the Medical University of South Carolina in 2014. His passion for medical education stems from his mission to motivate and inspire learners to become the best physicians possible for their future patients.
Case Summary
A middle-aged woman with a history of treated breast cancer and unspecified uveitis presented with subacute fever, arthralgias, and headache. She was found to have elevated inflammatory markers, extensive lymphadenopathy, and a cholestatic pattern of liver injury with an unrevealing evaluation for infectious and autoimmune pathologies. She remained febrile despite broad-spectrum antibiotics. She was then started on empiric doxycycline, which resulted in prompt resolution of her fevers. A serologic test for Rickettsia rickettsii returned positive, confirming the diagnosis of “spotless” Rocky Mountain Spotted Fever.
Teaching Points:
Rocky mountain spotted fever(RMSF) is an acute, life-threatening febrile illness caused by the intracellular pathogen,Rickettsia rickettsii. Endemic to the southeastern and south central regions of the United States, it is transmitted by ticks (esp Dermacentor ). The classic triad of symptoms includes fever, headache, and rash (often beginning on the wrists and ankles, progressing from maculopapular to petechial). Roughly 10-12% of cases may present without rash (i.e., “spotless” RMSF), more commonly reported in elderly and/or African American patients. Given its high mortality rate, prompt initiation of empiric doxycycline is important for improving outcomes.
Episode – 89 – Virtual Morning Report #50 with Drs. Kimberly Manning and Gurpreet Dhaliwal – Foot Drop
May 19, 2020
Click here to learn more about joining VMR and learn together, live.
Dr. Kimberly Manning
Kimberly D. Manning, MD is a general internist/hospitalist who serves as Associate Vice Chair of Diversity, Equity, and Inclusion for the Department of Medicine at Emory University School of Medicine. Manning was recently promoted to Professor of Medicine and additionally serves as residency program director for the Transitional Year Residency Program at Emory. She has a strong commitment to supporting underrepresented minorities in medicine, serving underserved populations, and creating better understanding of our patients and each other through storytelling and narrative medicine. A huge fan of the CP Solvers, Dr Manning is as enthusiastic about being a teacher as she is being a lifelong learner.
Dr. Gurpreet Dhaliwal
Dr. Dhaliwal is a clinician-educator and Professor of Medicine at the University of California, San Francisco. He is the site director of the internal medicine clerkship at the San Francisco VA Medical Center, where he teaches medical students and residents in the emergency department, urgent care clinic, inpatient wards, outpatient clinic, and morning report. His academic interests are the cognitive processes underlying diagnostic reasoning and clinical problem-solving and the study of diagnostic expertise. Dr. Dhaliwal enjoys playing pickup basketball with his two sons … even though both can handily defeat him
Case Summary
A 69-year-old man with a history of prior cerebrovascular accident (CVA) presented with acute onset right leg weakness and paresthesias. Laboratory analysis was notable for elevated inflammatory markers. A magnetic resonance image of the brain showed a ring-enhancing lesion in the left parietal lobe, with fine needle aspiration revealing gram positive cocci in chains. Cultures grew Streptococcus intermedius (a member of the S. anginosusgroup), and the patient was diagnosed with a bacterial brain abscess.
Teaching Points:
Brain abscesses can be caused by bacteria, fungi, and parasites. Bacterial brain abscesses can arise via contiguous spread of bacteria from head and neck sources or by hematogenous routes. The causative organism often varies with the underlying immune status of the host. Among immunocompetent hosts, the most common organisms are Staphylococcusand Streptococcus spp (e.g., S anginosus). Neurosurgical sampling may be required to identify the pathogen and achieve source control.
Lacunar infarctions are an important form of ischemic strokes (representing ~20%) caused by cerebral small vessel disease. Pathophysiologically, the most important risk factor is uncontrolled hypertension, which can lead to small vessel injury and subsequent occlusion. Most lacunar strokes involve the basal ganglia, pons, and subcortical white matter structures (e.g., internal capsule). While many clinical syndromes have been described, the 5 most common include pure motor, pure sensory, mixed sensorimotor, ataxic hemiparesis, and dysarthria-clumsy hand syndrome.
Episode 88 – RLR – Transient Loss of Consciousness
May 14, 2020
RLR #4 – Transient loss of consciousness A 43-year-old man with a history of epilepsy, coronary artery disease, and pulmonary sarcoidosis presented after experiencing an unheralded transient loss of consciousness. His initial evaluation revealed no abnormalities. Ambulatory cardiac event monitoring demonstrated an episode of complete heart block, and myocardial perfusion imaging showed a focal perfusion defect in the left ventricle (thought to represent a prior myocardial infarction versus sarcoidosis). He underwent pacemaker and implanted cardiac defibrillator (ICD) placement and was discharged home.
Teaching Point:
Small-cell lung cancer(SCLC) is a primary pulmonary malignancy of epithelial origin that most commonly occurs in older patients with long-standing smoking histories. Clinically, it typically presents aggressively with pulmonary symptoms (e.g., cough, dyspnea, hemoptysis), manifestations related to intra- or extra-thoracic spread, or with a variety of paraneoplastic syndromes (e.g., endocrine, dermatologic, neurologic). Prognosis is poor, with median survival without treatment being 2-4 months.
Sarcoidosis is a multisystem granulomatous disease that most often affects the lungs, skin, and eyes.Cardiac manifestationsof sarcoidosis include arrhythmias, cardiomyopathy, sudden cardiac death, and, rarely, coronary artery vasculitis. Diagnosis can be made by endomyocardial biopsy or with compatible imaging findings (e.g., delayed gadolinium enhancement on cardiac MRI) or cardiac manifestations (e.g., complete heart block, ventricular arrhythmias, or otherwise unexplained heart failure) in a patient with known extra-cardiac sarcoidosis.
RLR #3 – Scrotal pain A 75-year-old man with a history of Alzheimers dementia presented with 2 weeks of bilateral scrotal pain. Genital exam was unremarkable. Chest radiography revealed a right lower lobe opacity and computed tomography of the abdomen was notable for diffuse retroperitoneal lymphadenopathy. Biopsy was performed of a mediastinal lymph node which revealed findings consistent with metastatic small-cell lung cancer.
Teaching Points:
Acute scrotal pain is a common complaint encountered in the emergency department and can be caused by pathology within the scrotum, abdomen (i.e., inguinal hernia), or referred from the retroperitoneum. The most common causes of acute scrotal pain include torsion of the testicular appendage, epididymitis, and testicular torsion. The initial evaluation is focused on excluding the presence of testicular torsion (a surgical emergency) by exam and, often times, doppler ultrasonography.
Episode 86: Racial Disparities in COVID – Student Dr. Paul, Dr. Essien & Dr. Manning
May 10, 2020
Student Dr. Dereck Paul, Dr. Utibe Essien and Dr. Kimberly Manning join the CPSolvers to discuss racial disparities. This all-star crew discusses the role of race and inequality in the current COVID-19 pandemic and medicine more broadly. Don’t miss out on this truly powerful episode.
Student Dr. Dereck Paul
Dereck Paul is a 4th-year medical student at the University of California, San Francisco School of Medicine and applying into residency this fall. He studies the relationships between homelessness and health under Dr. Margot Kushel at the UCSF Center for Vulnerable Populations. He was a 2018 Student National Medical Association David E. Satcher MD, PhD Health Disparities Research Fellow for his work mapping the role of structural racism in susceptibility to housing insecurity and homelessness. Outside of his studies and research, he writes about health policy, medical education, and the underrepresented medical trainee experience.
Dr. Utibe Essien
Utibe Essien is an Assistant Professor of Medicine at the University of Pittsburgh and a health disparities researcher in the VA Center for Health Equity Research and Promotion. He completed Primary Care residency and General Internal Medicine fellowship at the Massachusetts General Hospital and Harvard Medical School. Dr. Essien’s research focuses on developing interventions to advance equity in the management of cardiovascular diseases.
Dr. Kimberly Manning
Kimberly D. Manning, MD is a general internist/hospitalist who serves as Associate Vice Chair of Diversity, Equity, and Inclusion for the Department of Medicine at Emory University School of Medicine. Manning was recently promoted to Professor of Medicine and additionally serves as residency program director for the Transitional Year Residency Program at Emory. She has a strong commitment to supporting underrepresented minorities in medicine, serving underserved populations, and creating better understanding of our patients and each other through storytelling and narrative medicine. A huge fan of the CP Solvers, Dr Manning is as enthusiastic about being a teacher as she is being a lifelong learner.
Episode 85: Virtual Morning Report unknown with Dr. Avital O’Glasser & CPSolvers, Jack and Reza – fever, joint pain & rash
May 07, 2020
Avital O’Glasser is an Associate Professor of Medicine at Oregon Health & Science University (OHSU) in the Division of Hospital Medicine. She is the medical director of OHSU’s hospitalist-led Pre-Operative Medicine Clinic, as well as The Curbsiders Kashlek Memorial Hospital Chief of Perioperative Medicine. She is also the Assistant Program Director for Social Media and Scholarship for OHSU’s Internal Medicine Residency Program. She has been a member of the OHSU faculty since completing her internal medicine residency training there, and she is a graduate of Jefferson Medical College. She enjoys spending time with her husband, two young boys, and labradoodle Matilda.
Case Summary
A 31-year-old man with no prior medical problems presented with subacute abdominal pain, recurrent fevers, and weight loss. His work-up was notable for stigmata of endocarditis, although bacterial blood cultures were persistently negative. Ultimately, he underwent aortic valve replacement, and pathologic examination of the valve tissue demonstrated coliform bacteria with molecular testing confirming a diagnosis of Streptobacillus moniliformis. Further history confirmed that he owned a pet rat and had experienced repeated bites prior to his illness.
Teaching Points
Streptobacillus moniliformisis a pleomorphic, gram-negative rod that is the predominant cause ofrat bite fever (RBF). This pathogen is found across the United States and is most commonly transmitted by rat bites, with numerous cases being acquired from pets or laboratory animals. Clinical manifestations include fever (potentially relapsing), arthralgias, and rash. Serious complications include infective endocarditis, meningitis, systemic vasculitis, and other organ involvement.
RLR #2 – Hoarseness A 54-year-old man with a history of PTSD, depression, and a recent diarrheal illness presented with acute dysphagia to liquids and solids. Neurologic exam was initially unremarkable, but the patient returned the next day with diplopia and ataxia. Exam was notable for new bilateral cranial nerve III palsies and areflexia. Laryngoscopy revealed unilateral vocal cord paralysis. Cerebrospinal fluid analysis was notable for elevated protein and positive GQ1b antibody testing. He was diagnosed with Miller Fisher’s syndrome, a variant of Guillain-Barre Syndrome.
Teaching Points:
Miller Fisher’s Syndrome(MFS) is a rare variant of Guillain-Barre syndrome (acute inflammatory demyelinating polyneuropathy) that primarily affects the bulbar nerves. MFS is suggested by the classic triad of acute-onset ophthalmoplegia, ataxia, and areflexia and often occurs following a prodromal illness (upper respiratory infection or gastroenteritis). Diagnosis is supported by elevated cerebrospinal fluid protein as well as demonstration of GQ1b ganglioside autoantibodies (which are positive in 85% of cases). Prognosis is typically favorable, and most cases are self-limited.
RLR #1 – Lymphadenopathy A woman in her 20’s with a history of prior possible thrombotic thrombocytopenic purpura (TTP) and recently treated secondary syphilis was transferred to a tertiary referral center for evaluation of generalized lymphadenopathy, new anemia, and thrombocytopenia. Laboratory workup was concerning for a Coombs-positive autoimmune hemolytic anemia, possible immune thrombocytopenia, and polyclonal gammopathy. Core and excisional lymph node biopsies were unrevealing for either infection or malignancy. Ultimately, anti-nuclear, anti-dsDNA, and anti-Sm autoantibodies were grossly positive and the patient was diagnosed with systemic lupus erythematosus.
Teaching Points:
Systemic Lupus Erythematosus(SLE) is a complex autoimmune disease that most frequently presents with inflammatory arthritis, malar rash, and nephropathy.Hematologic abnormalities are common in SLE and are components of both the American College of Rheumatology (ACR) and Systemic Lupus International Collaborating Clinics (SLICC) diagnostic criteria. Common features include leukopenia (both neutropenia and lymphopenia), autoimmune hemolytic anemias (generally Coombs-positive, warm-type), and thrombocytopenia. SLE is a recognized cause of secondary thrombotic thrombocytopenic purpura (TTP), which may present concurrently with or, in some instances, precede the diagnosis of SLE.
Episode 82: Virtual Morning Report unknown with student Dr. Jean-Claude Guidi and Drs. Kushal Vaishnani & Ramya Ramachandran – hypoxemia
Apr 29, 2020
Problem Representation A 53-year-old woman with a history of rheumatoid arthritis and amiodarone-induced lung injury on immunosuppression presented with acutely progressive hypoxic respiratory failure and hypotension, found to have a serpiginous truncal rash, acute anemia, and elevated beta-d-glucan. Schemas In this episode, we revisit the schemas for fever and rash (which highlights first addressing the life-threatening causes) and diffuse alveolar hemorrhage (which focuses on differentiating vasculitis from other etiologies). Diagnosis The patient underwent bronchoscopy with bronchoalveolar lavage fluid demonstrating elevated leukocytes with a neutrophilic predominance as well as progressively bloody fluid, consistent with diffuse alveolar hemorrhage. Silver stain was diagnostic for Pneumocystis jiroveci, and pathology revealed helminthic larvae consistent with Strongyloides stercoralis. The patient was diagnosed with both Pneumocystis pneumonia and Strongyloides hyperinfection syndrome!
Teaching Points:
Beta-D-glucan(BDG) is a cell wall polysaccharide found in many fungal organisms (with notable exceptions including Cryptococcus, the zygomycetes, and Blastomyces dermatitidis) and is frequently used as a laboratory marker for invasive fungal infections. Caution is advised when interpreting this test, as it is imperfectly sensitive and false positives have been reported in association with certain hemodialysis filters, immunoglobulins (e.g., IVIG), albumin, and beta-lactam antimicrobials (thought to be more of an issue with older formulations).
Strongyloides stercoralisis an important human pathogen in tropical and subtropical areas throughout the world. While many cases of chronic strongyloidiasis are mild and may go unrecognized, severe manifestations can include the strongyloides hyperinfection syndrome and disseminated strongyloidiasis. Hyperinfection occurs when there is accelerated autoinfection (i.e., the ability to complete the parasitic life cycle entirely within the host – a trait relatively unique to Strongyloides among human helminthiases) and most commonly occurs in the setting of immune dysregulation or exogenous immunosuppression.
Pneumocystis jiroveciis an important opportunistic infection in immunosuppressed patients. Originally identified by Carlos Chagasin 1909, who believed it to represent a pulmonary manifestation of the parasite Trypanosoma cruzi, it was later reclassified as a fungus in 1988. The most frequent symptoms include subacute dyspnea, nonproductive cough, and low-grade fever, with hypoxemic respiratory failure being the most common manifestation of severe decompensation.
Episode 81: Human Dx unknown with Dr. André Mansoor & OHSU residents – dyspnea and weight loss
Apr 23, 2020
“Logan” Jones is a PGY-3 at OHSU in Portland, and will be joining the faculty as an assistant professor in the Division of Hospital Medicine with an academic focus on student assessment, curricular innovation, learner scholarship, clinical reasoning, and EMR proficiency. He is active in organized medicine with the American Medical Association and the American College of Physicians. Outside of medicine, he enjoys cooking with his sig fig Samantha, spending time on his yoga mat, and hiking throughout the Pacific Northwest.
Dr. Patricia Liu
Pat is currently one of the IM chief residents at Oregon Health & Science University. She will be a hospitalist next year and is interested in medical education, empowering women in medicine and improving care for inpatients with substance use disorders. In her free time, you can find her running, snowboarding and teaching tricks to her cat, Pekoe.
Dr. Ruchit Rana
Ruchit Rana is currently a second-year internal medicine resident at Baylor College of Medicine. He completed medical school at Baylor College of Medicine. He has a passion for practicing and improving medical education at all levels. In his free time, he enjoys cooking and baking dishes across all ethnicities and maintaining his multiple freshwater aquariums at home.
Dr. André Mansoor
André Mansoor is an Assistant Professor of Medicine at Oregon Health and Science University in Portland, Oregon. His favorite book is the Count of Monte Cristo and his favorite band is Stone Temple Pilots. He is the author of an internal medicine textbook called Frameworks for Internal Medicine. https://www.amazon.com/Frameworks-Internal-Medicine-Andre-Mansoor/dp/1496359305.
Case Summary
A 70-year-old man presented with six months of dyspnea on exertion, night sweats, and weight loss. He was found to be febrile and in distributive shock, with laboratory analysis demonstrating cytopenias, coagulopathy, and lactic acidosis. Computed tomography of the abdomen and pelvis was notable for hepatosplenomegaly, and a bone marrow biopsy revealed a monoclonal B-cell population with hemophagocytosis. The patient was diagnosed with diffuse large B-cell lymphoma complicated by hemophagocytic lymphohistiocytosis (HLH).
Teaching Points:
Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening, immune-mediated disease caused by impaired NK and cytotoxic T-cell function. While genetic defects play a prominent role in triggering HLH in children, most cases of HLH in adults are secondary to another disorder, such as infections (e.g., EBV, histoplasmosis), hematologic malignancies (e.g., NK, T, or B-cell lymphomas), or autoimmune disease (e.g., systemic lupus erythematosis).
Episode 80: Human Dx unknown with Rabih & Indiana residents – fatigue and weight loss
Apr 21, 2020
Devika Gandhi is a second-year internal medicine resident at Indiana University. She is originally from Dayton, Ohio and received her undergraduate degree from the University of Akron. She earned her medics degree from Northeast Ohio Medical University in Rootstown, Ohio (Go Walking Whales!). After residency, she plans to pursue a career in gastroenterology/hepatology. During her free time, she enjoys reading, cooking, and going out to trivia with friends.
Dr. Cody Hill
Cody Hill is a second-year Med-Peds resident at Indiana University. He attended Clemson University for his undergraduate/graduate studies and the University of South Carolina School of Medicine Greenville for medical school. Although he loves taking care of patients, his true passion lies in medical education, especially when it relates to clinical reasoning and evidence-based medicine. He is also very invested in resident wellness and mentorship, which led him and a fellow classmate to start their own podcast called The Resident Lounge (@resident_lounge). After residency, he plans to pursue a career as a Med-Peds hospitalist and a medical educator with the ultimate goal of one day becoming a program director. Cody also just became a father, so in addition to taking care of his newborn daughter, he and his wife enjoy walking their dog, gardening, cooking and exploring Indianapolis for new craft beers.
Dr. Anand Patel
Dr. Anand Patel is a hematology-oncology fellow at the University of Chicago and the Medical Education Lead at the Human Diagnosis Project. He attended University of Missouri-Columbia for medical school and completed both his internal medicine residency and chief residency at Northwestern. Anand’s academic interests include medical education and clinical reasoning. Specifically within hematology-oncology, he is interested in clinical trial design using targeted therapies for patients with leukemias and myeloid neoplasms.
Case Summary
An 83-year-old woman with acute myeloid leukemia and psoriasis (on immunosuppression) presented with six weeks of fatigue, weight loss, and a dry cough. Her medical history was notable for two indeterminate interferon-gamma release assays. Computed tomography of the chest demonstrated a 3 x 3 cm right lower lobe mass, with subsequent biopsy revealing necrotizing granulomas and acid-fast bacilli. Cultures ultimately grew Mycobacterium avium complex (MAC).
Teaching Points:
Mycobacterium avium complex (MAC) is a ubiquitous water and soil-based organism. Clinical manifestations include pulmonary infections, lymphadenitis, and disseminated disease in severely immunocompromised patients (e.g., those with HIV and CD4 counts < 50 cells/µL). Pulmonary manifestations of MAC include cavitary upper lobe disease similar to tuberculosis, fibronodular bronchiectasis that often develops in the right middle lobe or lingula, solitary pulmonary nodules, and hypersensitivity pneumonitis.
Episode 79: Human Dx unknown with Reza & U of C residents – abdominal pain
Apr 19, 2020
Alec Rezigh is a third-year internal medicine resident at The University of Colorado. He is originally from Houston, TX and received his undergraduate degree at the University of Texas at Austin. He then went back to Houston for medical school at the University of Texas at Houston (McGovern) Medical School. In his free time, he loves all things basketball, traveling with his wife, and napping on the couch with his dog. Following completion of his training, he will return to Houston to be an academic hospitalist. He wishes to thank Dr. Juan Lessing for his amazing mentorship and inspiring his interest in clinical reasoning – and introducing him to Rabih and Reza!
Dr. Austin Rezigh
Austin Rezigh is a third-year internal medicine, primary care track resident at the University of Colorado. He completed medical school at UT Southwestern and is excited to pursue a career in academic general internal medicine. In his free time, he enjoys trying new cuisines, exercising, and spending time with his fur-niece, Kensie.
Dr. Anand Jagannath
Dr. Anand Jagannath is a clinician-educator at the University of California, San Diego (UCSD) and hospitalist at the VA San Diego. He completed medical school at the Tufts University School of Medicine and internal medicine residency and chief residency at Albert Einstein College of Medicine/Montefiore Medical Center. At UCSD, Anand’s interests include bedside team rounding, teaching clinical reasoning to medical students and residents, learning from his learners, and promoting a safe and inclusive learning environment. He is also a Section Editor for adult medicine cases at the Human Diagnosis Project. When he’s not getting excited about medicine, you’ll probably find Anand cooking food, watching shows about food on Netflix, running, or playing basketball or his violin.
Human Dx Case Summary
A 66-year-old man with alcohol use disorder and chronic NSAID use presented with one day of abdominal pain and nausea. Laboratory analysis was notable for hypercalcemia to 16 mg/dL (with low parathyroid hormone and vitamin-D levels), metabolic alkalosis, and an acute kidney injury. The patient disclosed that he had recently consumed large amounts of calcium carbonate for his abdominal pain, and he was diagnosed with the milk alkali syndrome. His serum calcium normalized after receiving intravenous fluids and withholding further calcium supplementation.
Teaching Points:
The milk alkali syndrome, the third most common cause of hospital admission for hypercalcemia, develops from excess consumption of calcium supplements (e.g., calcium carbonate). Patients classically present with hypercalcemia, metabolic alkalosis, and renal insufficiency. The metabolic alkalosis is thought to be due to hypercalcemia-induced nephrogenic diabetes insipidus, while renal insufficiency develops as a result of calcium-induced renal tubular damage and vasoconstriction of the renal afferent arteriole. Treatment includes intravenous fluid resuscitation and cessation of calcium supplementation.
Episode 78: Spaced Learning Series – Hyponatremia and AKI
Apr 15, 2020
Ellie Garbade is a current chief resident at the University of Rochester Medical Center, where she completed her internship and residency in Internal Medicine. Following chief year, she plans to continue her career at the University of Rochester as an academic hospitalist.
Dr. Aimee Zaas
Aimee Zaas is an Associate Professor of Medicine at Duke University School of Medicine in the Division of Infectious Diseases and International Health. She serves at the Program Director for the Duke Internal Medicine Residency Program and spends her clinical time on the general medicine service with residents and students as well as on the Transplant Infectious Diseases consultative service at Duke Hospital. After completing her medical school at the Feinberg School of Medicine at Northwestern University, she completed her residency and Assistant Chief of Service (Thayer!) at The Johns Hopkins Hospital and her Infectious Diseases fellowship at Duke. She enjoys spending time with her husband, two boys (but, let’s face it, they are teenagers so are never home) and two dogs, cheering on her kids’sports, the Duke Blue Devils and St. Louis Cardinals as well as trying out new restaurants and excellent coffee.
Episode 76: Human Dx unknown with Reza, Sal, and student Dr. Boateng – Fever
Mar 26, 2020
Boateng Kubi is a third-year medical student at Johns Hopkins University School of Medicine and will be applying to residency programs this fall. He is excited to pursue a career in academic surgery and has developed an early interest in cardiothoracic surgery. He is interested in outcomes research, medical education, and clinical reasoning. His clinical interests include cardiovascular infections, thoracic malignancies, and heart & lung transplantation. A Maryland native, he enjoys spending his free time with family, working out, or exploring restaurants in Baltimore with friends.
Dr. Sneha Thatipelli
Sneha Thatipelli is a third year internal medicine resident at Northwestern Memorial Hospital. She completed her medical school at UCSF, and is excited to pursue a career in Infectious Disease with a focus on HIV medicine. She is passionate about medical education and understanding barriers to provide equitable care for vulnerable populations. She will be a graduate of the Health Equity and Advocacy Clinical Scholars (HEACS) program at McGaw and hopes to use this training for clinical care and also medical education of trainees.
Episode 75: Human Dx unknown with Rabih and Einstein residents, Dr. Gandhi and Dr. Bressman – fever and headache
Mar 24, 2020
I graduated from NYU medical school and am now finishing my PGY-3 year at Montefiore Medical Center in the Bronx, NY. My clinical interests include preventative cardiology and medical education and I am excited to be starting my cardiology fellowship at Northshore University Hospital- Northwell in Long Island. When I am not in the hospital I love hiking, running, cooking, and exploring different styles of dance.
Dr. Max Bressman
I went to Swarthmore College where I played tennis for the college team (ranked top 25), went to NYU Medical School (switched to golf, now attempt to qualify for the US Open every year and came 1 stroke from making the US national amateur championship last year). Finishing PGY-3 year at Montefiore in the Bronx, NY. Was originally planning on cardiology, but changed my mind and am going to stay as a Hospitalist at Montefiore and get involved in education. While at Montefiore, published abstracts, posters, and just got a manuscript into AJM. Anand Jagannath was my chief as an intern and we wrote and abstract/poster (along with Firm-1 leader Matt Shaines) that won the top prize at SHM in 2018.
Alex Hajduczok
Alex Hajduczok is a second-year internal medicine resident at Penn State Hershey Medical Center. He is originally from Buffalo, New York and completed is undergraduate degree in biochemistry at the University of Rochester and stayed at the University of Rochester School of Medicine & Dentistry for medical school. After residency, he plans to pursue a career as a clinician-investigator in cardiology. He is currently engaged in heart failure remote monitoring research at Penn State Hershey. In his free time, he enjoys working out, coaching CrossFit, and playing hockey.
Episode 74: On COVID-19 – A case-based discussion with Drs. Block, Thakur, and Chin-Hong
Mar 22, 2020
Peter Chin-Hong is Associate Dean for Regional Campuses at UCSF School of Medicine. He is a medical educator who specializes in treating infectious diseases, particularly infections that develop in patients who have suppressed immune systems, such as as solid organ and hematopoietic stem cell transplant recipients and HIV+ organ transplant recipients. He directs the immunocompromised host infectious diseases program at UCSF. He has been involved in the COVID19 clinical consultation and treatment team.
Dr. Neeta Thakur
Neeta Thakur is a Pulmonary Critical Care Physician and health disparities researcher at UCSF. Her main research interests are in understanding how the social environment contributes to disease and modifies disease course in low-income communities and communities of color. Dr. Thakur’s experience as a clinician and Medical Director of the Zuckerberg San Francisco General Hospital Chest Clinic, gives her first-hand insight on how social and environmental stress negatively affect asthma and other health outcomes, and practical knowledge of the existing barriers to adoption of evidence-based interventions into practice. With the evolving COVID-19 epidemic, her research focus has shifted to better understand the fears, needs, and socioeconomic impact in low-income, diverse communities.
Dr. Brian Block
Brian Block is an Instructor of Medicine and Research Fellow in the Division of Pulmonary and Critical Care Medicine at UCSF. He has interests in medical ethics and critical illness communication. He graduated from Harvard Medical School and completed Internal Medicine training at Columbia University where he was also a Chief Resident. He then came to UCSF to complete fellowship training in Pulmonary and Critical Care medicine. His UCSF bio also describes him as a “mediocre golfer” and now he can’t figure out how to have that removed.
Episode 73: Clinical unknown with Dr. Joel Topf – Polyuria
Mar 21, 2020
Joel Topf went to medical school at Wayne state University School of Medicine and did Med-Peds at Indiana University. He completed an adult fellowship in nephrology at the University of Chicago. He is currently a clinical nephrologist in Detroit at Oakland University William Beaumont School of Medicine. Joel’s passion is using social media and new media to teach nephrology. He started his blog, PBFluids in 2008. He developed NephMadness and NephJC to leverage the power of community, digital scholarship and creativity to teach nephrology. He is the founder and program director of the Nephrology Social Media Collective internship which trains medical professionals to use social media for medical education. Joel is a pioneer in bringing visual abstracts to nephrology and is a visual abstract editor for CJASN and the American Journal of Nephrology. He is creator and host of the nephrology podcast, Freely Filtered. He was recognized by the American Society of Nephrology with the Robert Narins award for innovations in Teaching in 2017.
Dr. Madeline McCrary
Madeline McCrary is a third year Internal Medicine resident at Christiana Care in Delaware. She is originally from Annapolis, MD but moved down south to North Carolina for the next 10 years. She went to Duke for undergrad then switched sides and went to UNC for medical school. She will be starting Infectious Diseases fellowship at UNC in July. In her spare time, she enjoys exploring with her dog Sammie, spending time with family and friends, and playing board games.
Dr. Bob Centor
Dr. Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama.
Episode 72 – On COVID-19 – A conversation with Colleagues from Italy Part 2
Mar 19, 2020
Marco Ripa is a Researcher and Infectious Disease physician working at IRCCS San Raffaele Hospital in Milan. His main research topics are sepsis, bloodstream infections and infective endocarditis. During his specialty training, he worked for one year at the Hospital Clinic in Barcelona with professor Alex Soriano and professor José Maria Miró in the Nosocomial Infections and Cardiovascular Infection Units. He is a member of the ESCMID Study Group for Bloodstream Infections, Endocarditis and Sepsis (ESGBIES). Currently, he is working in the COVID-19 dedicated ward of San Raffaele Hospital.
Dr. Giacomo Monti
Giacomo Monti is a consultant in Anesthesia and Intensive Care working in the general ICU, medical emergency team and emergency operating room of one the most important University Hospital in Italy. He’s actively involved in scientific research on sepsis, invasive and non-invasive ventilation, outcome after surgery, sedation in ICU, and kidney failure. He has been the Principal Investigator for many international collaborative studies. Currently, he’s leading different research projects, thanks to different grants from public and private founders. He’s active in teaching as adjunct professor on different topics both for medical and post graduates students.
Episode 71 – On COVID-19 – A conversation with Colleagues from Italy Part 1
Mar 18, 2020
Marco Ripa is a Researcher and Infectious Disease physician working at IRCCS San Raffaele Hospital in Milan. His main research topics are sepsis, bloodstream infections and infective endocarditis. During his specialty training, he worked for one year at the Hospital Clinic in Barcelona with professor Alex Soriano and professor José Maria Miró in the Nosocomial Infections and Cardiovascular Infection Units. He is a member of the ESCMID Study Group for Bloodstream Infections, Endocarditis and Sepsis (ESGBIES). Currently, he is working in the COVID-19 dedicated ward of San Raffaele Hospital.
Dr. Giacomo Monti
Giacomo Monti is a consultant in Anesthesia and Intensive Care working in the general ICU, medical emergency team and emergency operating room of one the most important University Hospital in Italy. He’s actively involved in scientific research on sepsis, invasive and non-invasive ventilation, outcome after surgery, sedation in ICU, and kidney failure. He has been the Principal Investigator for many international collaborative studies. Currently, he’s leading different research projects, thanks to different grants from public and private founders. He’s active in teaching as adjunct professor on different topics both for medical and post graduates students.
Episode 70 – On COVID-19 w/ Dr. Carlos Del Rio & App Announcement
Mar 15, 2020
Carlos del Rio, MD is Distinguished Professor of Medicine at Emory University School of Medicine and Professor of Global Health and Epidemiology at the Rollins School of Public Health of Emory University. He is co-Director of the Emory CFAR and co-PI of the Emory-CDC HIV Clinical Trails Unit and the Emory Vaccine Treatment and Evaluation Unit. Dr. del Rio is a native of Mexico where he was Executive Director of the National AIDS Council of Mexico (CONASIDA, the Federal agency of the Mexican Government responsible for AIDS Policy throughout Mexico), from 1992 through 1996. He was also a member of the National Academy of Medicine.
Dr. Kumfer is a third year resident at the University of North Carolina Internal Medicine Residency. She completed medical school at Texas Tech University Health Science Center. She is pursuing a career in hospital medicine and is interested in medical education and diagnostic clinical reasoning. In her time away from work, she enjoys traveling, running, and spending time with her husband and dog.
Dr. Maxwell Diddams
Dr. Maxwell Diddams is a 3rd year resident in Internal Medicine at the University of North Carolina at Chapel Hill where he will be staying for his fellowship in pulmonary and critical care. Max can be easily identified by the portable ultrasound he always carries, and is interested in point-of-care ultrasound for the internist and intensivist. Outside of medicine he enjoys rock climbing, good jokes, Chinese language learning, and pants with pockets large enough for the whole bottle of ultrasound gel.
Dr. Travis Smith
Travis Smith is an attending EM doc and clinical preceptor at St. Vincent’s Southside in Jacksonville, Florida. He also currently serves as a Regional Dean for the Lake Erie College of Osteopathic Medicine where he helps mentor 50 wonderful and bright third and fourth year medical students. He is a graduate from the University of Florida Emergency Residency-Jacksonville campus in 2012 and Lake Erie College of Osteopathic Medicine-Bradenton in 2009. He received a degree in Biological Science from The Florida State University in 2005 (go Noles). In his spare time, he enjoys being a father of 3 young kids, golfing as much as possible, FSU football, and bedside ultrasound with his new Butterfly IQ.
Episode 67: Human Dx unknown with Reza & Pitt residents – altered mental status
Feb 23, 2020
Christina Mallarino-Haeger is a third year Internal Medicine resident at UPMC/University of Pittsburgh. Originally from Bogota, Colombia; Christina completed her medical school at the Pontificia Universidad Javeriana, followed by a postdoctoral research fellowship at Brigham and Women’s hospital in Boston. Christina will be moving to Atlanta to continue her training in infectious diseases at Emory and is interested in pursuing a career as a physician-scientist and HIV researcher. When not in the hospital, Christina enjoys riding her bike, going to the symphony and watching movies.
Dr. Ryan Augustin
Ryan Augustin is a second-year internal medicine resident at the University of Pittsburgh Medical Center. He is originally from Minnesota (Twin Cities) and received his undergraduate degree in biochemistry from the University of St. Thomas. He graduated from Case Western Reserve University School of Medicine where his love for all things med-ed took root. After residency, he plans to pursue a career in medical oncology. During his free time, he enjoys playing piano and cooking with his wife.
Dr. Janna Raphelson
Janna Raphelson is a PGY-1 in Internal Medicine at UC San Diego. She is a born Midwesterner who moved to Montreal to complete her medical degree at McGill University and learn some French. Her clinical interests include physical exam teaching, clinical anatomy for internists, and point of care ultrasound. Since moving to California, she spends her free time running outside all year round and reading books on the beach.
Episode 66: Clinical unknown with Dr. Lekshmi Santhosh – joint pain and rash
Feb 20, 2020
Dr. Santhosh is Assistant Professor at UCSF in the Divisions of Pulmonary/Critical Care Medicine and Hospital Medicine. She cares for patients at UCSF in the medical and neurological ICUs, the general pulmonary outpatient clinic, and on the general medicine teaching service. She serves as the Associate Program Director of the UCSF Pulmonary/Critical Care Fellowship Program and is the Co-Director of the UCSF Women in Leadership Development program. She is involved in medical education at the medical student, resident, and fellow levels and is passionate about clinical reasoning, medical education, and leadership development.
Episode 65 – Spaced Learning Series – Hemolysis and Infection
Feb 12, 2020
Dr. Heldman is currently an infectious diseases fellow at the University of Washington. Originally from Cincinnati, OH, she completed her undergraduate education at Brown University in Providence, RI. She then began making her way west across the country, completing both medical school and internal medicine residency at Northwestern in Chicago, before heading out to the Pacific Northwest. Her academic interests include transplant ID, immunocompromised hosts, and medical education. In her spare time, she enjoys running, hiking, and exploring new restaurants.
Ryan Augustin is a second-year internal medicine resident at the University of Pittsburgh Medical Center. He is originally from Minnesota (Twin Cities) and received his undergraduate degree in biochemistry from the University of St. Thomas. He graduated from Case Western Reserve University School of Medicine where his love for all things med-ed took root. After residency, he plans to pursue a career in medical oncology. During his free time, he enjoys playing piano and cooking with his wife.
Dr. Christina Mallarino-Haeger
Christina Mallarino-Haeger is a third year Internal Medicine resident at UPMC/University of Pittsburgh. Originally from Bogota, Colombia; Christina completed her medical school at the Pontificia Universidad Javeriana, followed by a postdoctoral research fellowship at Brigham and Women’s hospital in Boston. Christina will be moving to Atlanta to continue her training in infectious diseases at Emory and is interested in pursuing a career as a physician-scientist and HIV researcher. When not in the hospital, Christina enjoys riding her bike, going to the symphony and watching movies.
Dr. Nick Duca
Dr. Nick Duca is an assistant professor of medicine in the division of general internal medicine at Penn State College of Medicine. He completed his internal medicine residency and chief residency at the University of Pittsburgh Medical Center- Presbyterian. He joined as faculty at Penn State College of Medicine in July of 2017. His clinical roles include outpatient medicine as well as attending on the inpatient teaching services at Hershey Medical Center. He has a strong interest in mentoring and clinical reasoning. He currently serves as clerkship director for the internal medicine clerkship. In his free time he loves spending time with his wife, Lauren, 3-month-old daughter Natalie, and their Beagle, Simon. He also enjoys fishing the beautiful trout streams of central Pennsylvania, hiking, and practicing mindfulness meditation.
Episode 62: Clinical unknown w/ Rabih & Reza at DEM – bloating and abdominal distension
Jan 22, 2020
Andrew Olson is an Associate Professor of Medicine and Pediatrics at the University of Minnesota Medical School. He grew up on a farm in Iowa and then attended medical school at the University of California, Davis, did an internship in medicine at UCSF, and then residency in Medicine and Pediatrics at the University of Minnesota. A hospitalist, his work focuses on improving diagnostic performance through education as well as educational approaches to teach clinical reasoning. He is the co-chair of the Education Section of the Society to Improve Diagnosis in Medicine.
Dr. Gurpreet Dhaliwal
Dr. Dhaliwal is a clinician-educator and Professor of Medicine at the University of California, San Francisco. He is the site director of the internal medicine clerkship at the San Francisco VA Medical Center, where he teaches medical students and residents in the emergency department, urgent care clinic, inpatient wards, outpatient clinic, and morning report. His academic interests are the cognitive processes underlying diagnostic reasoning and clinical problem-solving and the study of diagnostic expertise. Dr. Dhaliwal enjoys playing pickup basketball with his two sons … even though both can handily defeat him.
Mary Ann Hernando is a 5th-year medical student at the University of Pennsylvania in the process of applying in Internal Medicine. She is originally from Miami, Florida and received her undergraduate degree in neuroscience from the University of Miami. During medical school, she took a year out to pursue a Master of Public Health at Johns Hopkins University with a concentration in health systems and policy. In her spare time, Mary Ann enjoys cooking with friends, live music, and working her way through every escape room in Philadelphia.
H. Moses Murdock
H. Moses Murdock is a 5th year medical student at the University of Pennsylvania applying in Internal Medicine. He is originally from Orlando, Florida, and received his undergraduate degree at the University of Central Florida in molecular biology and microbiology. In his free time, Moses enjoys running, reading, and discovering new vegetarian restaurants.
Dr. Travis Smith
Travis Smith is an attending EM doc and clinical preceptor at St. Vincent’s Southside in Jacksonville, Florida. He also currently serves as a Regional Dean for the Lake Erie College of Osteopathic Medicine where he helps mentor 50 wonderful and bright third and fourth year medical students. He is a graduate from the University of Florida Emergency Residency-Jacksonville campus in 2012 and Lake Erie College of Osteopathic Medicine-Bradenton in 2009. He received a degree in Biological Science from The Florida State University in 2005 (go Noles). In his spare time, he enjoys being a father of 3 young kids, golfing as much as possible, FSU football, and bedside ultrasound with his new Butterfly IQ.
Episode 59 – Human Dx unknown w/ UCSD team – subacute abdominal pain
Dec 23, 2019
Rima Deshpande is a fourth year medical student at the University of California San Diego (UCSD) School of Medicine. She is originally from Thousand Oaks, California and completed her undergraduate biology degree from UCSD. She is interested in pursuing residency in Internal Medicine. In her free time she enjoys cooking, hiking, and going to the dog beach with her dog Rajah.
Dr. Elizabeth Hastie
Elizabeth (Lizzy) Hastie is a second year Internal Medicine resident at the University of California San Diego. She is originally from Cincinnati and graduated from Emory University School of Medicine. She is currently a part of the RACE (Resident as Clinical Educator) Track at UCSD and is interested in pursuing a career in medical education. During her free time, she enjoys hiking, running, and watching scary movies.
Dr. Anand Jagannath
Dr. Anand Jagannath is a clinician-educator at the University of California, San Diego (UCSD) and hospitalist at the VA San Diego. He completed medical school at the Tufts University School of Medicine and internal medicine residency and chief residency at Albert Einstein College of Medicine/Montefiore Medical Center. At UCSD, Anand’s interests include bedside team rounding, teaching clinical reasoning to medical students and residents, learning from his learners, and promoting a safe and inclusive learning environment. He is also a Section Editor for adult medicine cases at the Human Diagnosis Project. When he’s not getting excited about medicine, you’ll probably find Anand cooking food, watching shows about food on Netflix, running, or playing basketball or his violin.
Dr. Patrick Murphy
Pat is currently a 2nd year fellow in an acute care surgery and trauma fellowship in Indianapolis, Indiana. Originally from Nova Scotia, Canada he completed his General Surgery training at Western University in London, Ontario. During his training he successfully completed with MPH from Johns Hopkins University and his MSc from Western University. His main areas of interests are outcomes and health services research in emergency general surgery and trauma, with a focus on quality of care. Outside of medicine he enjoys competing in triathlons and playing soccer.
Martin Rofael graduated from the University of Washington School of Medicine and subsequently completed his residency at Highland Hospital in Oakland, California. He is currently a first year pulmonary and critical care fellow at UCSF. His clinical interests include global health, ultrasound, and health disparities in pulmonary and critical care. When away from the hospital, he enjoys being outdoors, playing sports, and traveling.
Dr. Meshell Johnson
Meshell Johnson is a Professor of Medicine at UCSF in the Division of Pulmonary, Critical Care, and Sleep Medicine. Her clinical home is the San Francisco VA Medical Center, where she attends mostly in the ICU. Her research lab is also located at the VA, where she focuses on better understanding the role of alveolar type I cells in lung injury and repair. She is passionate about diversity, equity, and inclusion (DEI) and has roles both in the Department of Medicine and the School of Medicine to promote DEI efforts across multiple platforms. In her free time, she loves to travel and spend time with family and friends.
Dr. McGee graduated from Northwestern University Feinberg School of Medicine. She is a second year internal medicine resident at Northwestern. After residency she plans to pursue training in cardiology, and takes particular interest in transcatheter interventions and medical education. In her free time she enjoys swimming, cooking for friends, and listening to jazz.
Dr. Graham Peigh
Graham Peigh is a third year Internal Medicine resident at Northwestern. Originally from Chicago, Graham completed undergrad at Princeton and medical school at Jefferson before returning to the Windy City for residency. Next year, Graham will be staying at Northwestern as a Chief Medical Resident, and will be applying for fellowship in Cardiology with hopes to pursue a career in academic Cardiology. When outside the hospital, Graham enjoys golfing, hiking, and cheering for the Chicago Cubs.
Dr. David Kudlowitz
David Kudlowitz is an internist and Site Director for the Internal Medicine Residency Program at NYU Langone Health. He works as a hospitalist and primary care physician. He is also Content Director of Clinical Reasoning for 1st year medical students.
Episode 55 – Human Dx unknown with Rabih & Brigham & Women’s residents – Drs. Hayes & Mehta – ESRD + dyspnea
Nov 24, 2019
Dr. Hayes graduated from the School of Medicine at the Oregon Health and Science University in Portland, Oregon. She is a 2nd year resident of the Brigham and Women’s Internal Medicine Residency in Boston, Massachusetts. Her clinical interests include pulmonary and critical care, the care of geriatric patients in the ICU, ethics and communication, and medical education. When away from the hospital, she is either curled up with a cup of tea and good book, or exploring a new river, mountain bike trail, or ski slope.
Dr. Pooja Mehta
Dr. Mehta graduated from Harvard Medical School. She is an intern of the Brigham and Women’s Internal Medicine Residency/Division of General Internal Medicine Primary Care Program in Boston, Massachusetts. Her clinical interests include primary care,health equity and social justice, trauma-informed care, and medical education. When away from the hospital she loves to explore various styles of dance, hike in the mountains, go for long walks along the river,read and cook.
Dr. Stephanie Sherman
Dr. Stephanie Sherman is an academic hospitalist at Baylor College of Medicine (BCM) at Ben Taub General Hospital and the Houston VA Medical Center. She is also an associate program director for the internal medicine residency with a focus on resident-as-teacher training, clinical reasoning, and bedside rounding. If she’s being truthful about how she spends her spare time, she often finds herself re-watching The Office with her husband and fellow clinical problem solver, Zaven Sargsyan.
Episode 54 – Clinical unknown w/ Dr. Paul Sax – Fever and Headache
Nov 21, 2019
Dr. Paul E. Sax is Clinical Director of the Division of Infectious Diseases and the HIV Program at Brigham and Women’s Hospital (BWH), and Professor of Medicine at Harvard Medical School. Dr. Sax received his MD from Harvard Medical School, then did his residency in Internal Medicine at BWH, then fellowship in Infectious Diseases at Massachusetts General Hospital. He is Editor-in-Chief of Open Forum Infectious Diseases, is Section Editor of HIV/AIDS in UpToDate, on the Editorial Board of NEJMJournal Watch Infectious Diseases (where he writes the HIV and ID Observations blog), and on the editorial advisory board of Medscape HIV/AIDS. Dr. Sax is also on the core faculty of the International AIDS Society – USA and the New England AIDS Education and Training Center. In addition to his clinical practice and teaching, Dr. Sax’s ongoing areas of research include clinical trials of antiretroviral therapies, cost-effectiveness of management strategies for HIV, and toxicity of antiretroviral therapy. He is presently the principal investigator at the BWH AIDS Clinical Trials Unit, and is a member of the Cost-Effectiveness of Preventing AIDS Complications (CEPAC) Research Group.
Episode 53 – Clinical unknown Dr. Paul Sax – Cough & Rash
Nov 13, 2019
Dr. Paul E. Sax is Clinical Director of the Division of Infectious Diseases and the HIV Program at Brigham and Women’s Hospital (BWH), and Professor of Medicine at Harvard Medical School. Dr. Sax received his MD from Harvard Medical School, then did his residency in Internal Medicine at BWH, then fellowship in Infectious Diseases at Massachusetts General Hospital. He is Editor-in-Chief of Open Forum Infectious Diseases, is Section Editor of HIV/AIDS in UpToDate, on the Editorial Board of NEJMJournal Watch Infectious Diseases (where he writes the HIV and ID Observations blog), and on the editorial advisory board of Medscape HIV/AIDS. Dr. Sax is also on the core faculty of the International AIDS Society – USA and the New England AIDS Education and Training Center. In addition to his clinical practice and teaching, Dr. Sax’s ongoing areas of research include clinical trials of antiretroviral therapies, cost-effectiveness of management strategies for HIV, and toxicity of antiretroviral therapy. He is presently the principal investigator at the BWH AIDS Clinical Trials Unit, and is a member of the Cost-Effectiveness of Preventing AIDS Complications (CEPAC) Research Group.
Rash
Radiology
Episode 52 – Spaced Learning Series – Fever and Rash
Nov 06, 2019
Dr. Redfield is a third-year internal medicine resident at Thomas Jefferson University Hospital. She is a graduate of University of Maryland and received her MD from University of Texas Health Science Center in San Antonio. Her clinical interests include mental health disease, hepatology and functional gastroenterology. When not in the hospital she enjoys eating, traveling and most importantly spending quality time (her love language) with friends and family.
Dr. Sean Dikdan
Dr. Dikdan is a third-year internal medicine resident at Thomas Jefferson University Hospital. He is a graduate of Boston College and obtained his dual MD/MPH from Rutgers New Jersey Medical School. His clinical interests include atrial fibrillation and medical education. Outside of the hospital, he enjoys cooking, podcasting, and escape rooms. He is applying for cardiology fellowship and creating his own podcast (Med Lit Review), but his most challenging aspect of residency is surviving the streets of Philadelphia as an avid NY Giants fan. #DannyDimes
Dr. Rebecca Berger
Rebecca Berger is an Assistant Professor of Medicine at Weill Cornell Medicine and a Hospitalist at New York Presbyterian Hospital. She completed medical school at Columbia University College of Physicians and Surgeons in New York and residency in internal medicine at Massachusetts General Hospital in Boston. Rebecca worked as an editorial fellow at the New England Journal of Medicine and was on the faculty at MGH before moving back to New York in 2018. Her academic interests include patient safety, quality and process improvement, and medical education.
Dr. Birnbaum graduated from Boston University School of Medicine. She is a third year Internal Medicine resident at the Baylor College of Medicine, and will be staying in Houston next year for her chief residency. Her clinical interests include primary care and medical education. When not in the hospital and clinics, she enjoys exploring the Houston foodie scene, watching movies, enjoying all things true crime, and spending time with her husband, Tyler, and Olde English Bulldogge, Bella.
Dr. Bibin Varghese
Bibin was born in the United Arab Emirates and moved to Texas as a teenager. He graduated from Baylor College of Medicine and is currently a 2nd year Internal Medicine resident at the Johns Hopkins Hospital. Bibin’s interests include cooking, watching the Great British baking show, eating, and going to the gym. His clinical interests include cardiology and medical education.
Dr. Jad Al Danaf
Dr. Al Danaf is a third year Cardiovascular Medicine Chief Fellow at the University of Utah and is board certified in Internal Medicine. He graduated from the Lebanese American University School of Medicine and finished his Masters in Public Health in Biostatistics & Epidemiology with a certificate in Quality, Patient Safety and Outcomes Research from the Johns Hopkins Bloomberg SPH. He completed his Internal Medicine training at Thomas Jefferson University Hospital in Philadelphia. He is an aspiring Interventional Cardiologist with interests in cardiac critical care, mechanical support, medical education, provider wellness, and quality improvement projects. Outside of work he enjoys cooking, being a foodie, exploring the outdoors and learning about new cultures with his wife and friends.
Dr. Zaven Sargsyan
Dr. Zaven Sargsyan is a hospitalist and associate residency director at Baylor College of Medicine (BCM). He completed medical school at BCM and medicine residency at Massachusetts General Hospital, and now rounds at Ben Taub Hospital and the VA in Houston. His academic interests include clinical decision-making, physical diagnosis, point-of-care ultrasound, and the language of medicine. In his free time, he likes to play soccer and chess with his nephews and hang out with his wife and fellow clinical problem solver Steph Sherman.
Amit Goyal (@AmitGoyalMD) is a cardiology fellow at the Cleveland Clinic. He completed his medical school at the University of California, San Diego and went on to enjoy residency training in the Osler Program at Johns Hopkins, where he served as the Assistant Chief of Service of the Barker Firm (aka Firm of Choice!). As ACS he co-founded (with Reza Manesh!) Osler Grand Rounds, an interactive mystery case discussion guided by expert discussants, and helped establish a novel morning report structure integrating bedside skills education. Amit is looking forward to a career as an interventional cardiologist and clinician educator. He began the Osler Program’s twitter account (@OslerResidency) and now co-manages the CCF Cardiology fellowship twitter account (@CCFcards). He relishes time with friends and family including with his wife Riddhi and son Dhruv.
Episode 47 – Spaced Learning Series – Altered Mental Status and Hypercalcemia
Sep 25, 2019
Mariana Urquiaga is a second-year internal medicine resident at the University of Alabama at Birmingham. She is from Lima, Peru, where she graduated from Universidad Peruana Cayetano Heredia. She has an interest in disorders of gut immunology. Outside of the hospital, she enjoys reading, swimming, and spending time with her boyfriend, Mauricio, and her dog, Otis.
Dr. Lindsey Shipley
Lindsey Shipley is a second year internal medicine resident at the University of Alabama, Birmingham. She was raised in Jackson, TN and received her medical degree from East Tennessee State University, Quillen College of Medicine. After residency, she hopes to pursue a career in gastroenterology. In her free time she enjoys lifting weights and spending time with family, friends, and her Airedale Terriers, KC and Izzy.
Dr. Anand Jagannath
Dr. Anand Jagannath is a clinician-educator at the University of California, San Diego (UCSD) and hospitalist at the VA San Diego. He completed medical school at the Tufts University School of Medicine and internal medicine residency and chief residency at Albert Einstein College of Medicine/Montefiore Medical Center. At UCSD, Anand’s interests include bedside team rounding, teaching clinical reasoning to medical students and residents, learning from his learners, and promoting a safe and inclusive learning environment. He is also a Section Editor for adult medicine cases at the Human Diagnosis Project. When he’s not getting excited about medicine, you’ll probably find Anand cooking food, watching shows about food on Netflix, running, or playing basketball or his violin.
I am from the great state of Oklahoma (Ohhhhhh-klahoma if you say it like the musical). I attended medical school and stayed for residency at Saint Louis University where I am currently a second year resident. After residency I hope to pursue a fellowship in pulmonology and critical care. I’m a serial hobbyist with interests ranging from sewing, to college football (Boomer Sooner), to researching future projects to do around my house.
Dr. Fernand Bteich
I hail from Lebanon and went to Saint Joseph University School of Medicine in Beirut (learnt medicine in French). I am now a third year Internal Medicine Resident at the Saint Louis University Hospital. I am pursuing a fellowship in hematology and oncology after residency. In my free time, I enjoy attending concerts, trying new restaurants, working out, fiddling with computer hardware and binging on Youtube.
Dr. Andrew Smaggus
Dr. Andrew Smaggus is a general internist in Kingston, Ontario, Canada. He is currently pursuing a Ph.D. in Healthcare Quality & Safety at Queen’s University. His interests include complexity science and its applications to healthcare. He has served as a contributing editor at HumanDx since 2017
Dr. Casey McQuade is a current chief medical resident at the University of Pittsburgh Medical Center. He completed his undergraduate studies in bioengineering and subsequently medical school at the University of Pennsylvania in Philadelphia. After he finishes his chief year, he will pursue a career as an academic hospitalist and wants to continue developing his skills as a clinician-educator. His primary research interests include strategies for reducing heart failure readmission rates and the use of social media for education. With the help of his colleagues, he runs the popular Twitter feed @MedEdPGH, which hosts live case discussions focused on developing participants’ clinical reasoning skills. Outside of work, Casey enjoys running, hiking, and playing the piano.
Hannah Kaizer went to University of Maryland School of Medicine and is now a second year resident in the Osler Medical Training Program at the Johns Hopkins Hospital. After residency, she hopes to complete a fellowship in hematology and oncology. Outside of the hospital, she enjoys cooking for friends and family, trying new restaurants, and spending time with her husband, Alex, and French Bulldog, Bruno.
Dr. Eva Valilis
Eva Valilis is a second year internal medicine resident at Johns Hopkins. She is a native Texan from El Paso and received her undergraduate degree at the University of Texas at Austin in public health. She graduated from the University of Texas at Houston Medical School, where she also obtained her Masters in Public Health. In her free time Eva enjoys shopping and traveling, particularly visiting her extended family in Greece.
Emma Levine is currently a fourth-year medical student at the University of California, San Francisco, applying to Internal Medicine residency programs this fall. She is interested in clinical and epidemiological research, medical education, and clinical reasoning. Her clinical interests include gastroenterology, with a special interest on how we can use food to heal the gut and better understanding the gut microbiome, as well as palliative care.
When not in the hospital, Emma enjoys training and teaching as a barre instructor, traveling the world with her family, and exploring restaurants in San Francisco and abroad.
Dr. Brooke Rice
Brooke Rice is currently an internal medicine intern at Boston Medical Center. She is originally from Boston; she completed college at Harvard University and taught math in Morocco before attending medical school at the University of California, San Francisco, and then finally ending up back in Boston again. She is interested in medical education and clinical research, and outside the hospital she enjoys cooking (and eating) Italian food, reading true crime novels, and all the summertime activities.
Dr. Chris Jackson serves as Assistant Professor of Medicine and Assistant Program Director for Ambulatory Education at the University of Tennessee Health Science Center (UTHSC). A native of Augusta, GA, he graduated from Emory University with a degree in Biology and Sociology. He received his Doctor of Medicine degree at the Medical College of Georgia. He completed his internal medicine and chief residency year in patient safety and quality improvement at UTHSC before joining the faculty in the Division of General Internal Medicine and the Center for Health System Improvement in 2019. Outside of work, he enjoys playing piano and watching forensic shows.
Dr. Zaven Sargsyan is a hospitalist and associate residency director at Baylor College of Medicine (BCM). He completed medical school at BCM and medicine residency at Massachusetts General Hospital, and now rounds at Ben Taub Hospital and the VA in Houston. His academic interests include clinical decision-making, physical diagnosis, point-of-care ultrasound, and the language of medicine. In his free time, he likes to play soccer and chess with his nephews and hang out with his wife and fellow clinical problem solver Steph Sherman.
Harry Hollander attends on the general medicine and infectious diseases services at UCSF.
We at the CPSolvers will add that:
Dr. Hollander is a beloved clinical educator who led the UCSF Internal Medicine program for 23 years, helping train over 1,000 residents. He is a consummate educator and a master clinician, who we are delighted to have on the final episode of our inaugural season.
Dr. Luis Rubio
Luis Alberto Rubio graduated from Yale School of Medicine and is originally from the West Texas town of El Paso. He is currently a third-year internal medicine resident at UCSF and next year will be starting his infectious disease fellowship at UCSF. His clinical interests include health care disparities, HIV, and loves all things related to tuberculosis. He is an avid Dallas Cowboys fan, and enjoys swimming, rock climbing, and dirt biking when away from the hospital.
Episode 37 – Clinical Unknown with Dr. Kwan, Dan, and Rabih – Diplopia
May 30, 2019
Janice Kwan is a general internist and Assistant Professor of Medicine at the University of Toronto. After completing medical school and residency in her hometown at the University of Toronto, she pursued a Master of Public Health at Harvard University and a fellowship with the Veterans Affairs Quality Scholars program. In 2016, she was awarded the inaugural research fellowship in diagnostic excellence with the Society to Improve Diagnosis in Medicine. Her research focuses broadly on improving the quality of care of general medical patients, and includes the study of diagnostic safety, test result follow-up, computerized decision support systems, and medication reconciliation. Janice prides herself on being a passionate snack enthusiast, devoted family member, and loyal Toronto sports fan
Episode 36 – Clinical unknown with Drs. Desai, Zarin-Pass, and Olson – Neuropathy
May 23, 2019
Brinda Desai is a 4th year Med-Peds Resident at the University of Minnesota who will be the next Med-Peds chief. Her professional interests include: clinical medicine in the ICU, social determinants of health, congenital pediatric diseases surviving into adulthood, and advocating for women in medicine. In her free time, she is obsessed with Bollywood dance, bouldering, yoga with the intent to find ultimate zen, and exploring new places through local food and music!
Dr. Margot Zarin-Pass
Margot Zarin-Pass graduated from UCSF School of Medicine and is now a third year resident in Internal Medicine and Pediatrics at the University of Minnesota. Her career interests include transitions of care between pediatric and adult medicine as well as medical education. In her free time, she hangs out with her wife and toddler son, who is getting new skills and stronger opinions every day.
Dr. Andrew Olson
Andrew Olson is an Associate Professor of Medicine and Pediatrics at the University of Minnesota Medical School. He grew up on a farm in Iowa and then attended medical school at the University of California, Davis, did an internship in medicine at UCSF, and then residency in Medicine and Pediatrics at the University of Minnesota. A hospitalist, his work focuses on improving diagnostic performance through education as well as educational approaches to teach clinical reasoning. He is the co-chair of the Education Section of the Society to Improve Diagnosis in Medicine.
Episode 35 – Clinical Unknown with Sharmin, Arsalan, and Reza – Syncope
May 21, 2019
Stephenie Le grew up in a small town in Ohio and attending college at the University of California, Berkeley and medical school at Albany Medical College in the beautiful upstate New York. She is currently a second year internal medicine resident at the University of California, San Francisco. She is interested in medical and clinician education, as well as clinical reasoning. In the future she plans to pursue additional specialty training in infectious diseases.
In her spare time, she likes to explore the outdoors and loves various hiking and camping trips planned with friends and family.
Dr. Harry Han
Harry Han graduated from the Perelman School of Medicine at the University of Pennsylvania and is currently a second-year internal medicine resident at UCSF. His clinical interests include palliative care and oncology. When not in the hospital or clinic, Harry enjoys brunch, reliving his childhood through watching the original Magic School Bus on Netflix, and visiting museums
Emily Silverman, MD is an academic hospitalist at the Zuckerberg San Francisco General Hospital, where she seeks out projects that resurrect the narrative soul of medicine. She is the creator and host of the live show and podcast, The Nocturnists, where health professionals share stories from the world of medicine. She wrote a series of prose-poems based on her experiences as a resident, and is currently working on her first book, a memoir. Her writing is animated by a deep-seated curiosity about science, human nature, and what it means to live and die well. In her spare time she enjoys teaching herself how to play electric guitar, listening to podcasts, and traveling with her husband Boaz. She tweets @ESilvermanMD.
Episode 32 – Clinical Unknown with Drs. Malevanchik and Winston – Cirrhosis + Dyspnea – Part 2
May 08, 2019
Dr. Lev Malevanchik completed medical school at Thomas Jefferson University and is finishing his third year of internal medicine residency at the University of California, San Francisco. This summer, he will start a fellowship in academic hospital medicine at UCSF focusing on medical education, point of care ultrasound, and improving the care of hospitalized patients with limited English proficiency. In his spare time, he loves going indoor rock climbing, listening to This American Life, and playing with his little dog Paprika.
Dr. Lisa Winston
Lisa Winston, MD is Professor of Medicine, Divisions of HIV/ID/Global Medicine and Hospital Medicine, University of California, San Francisco (UCSF). She completed medical school at the Johns Hopkins University School of Medicine. She was a resident in Internal Medicine, a chief resident, and a fellow in Infectious Diseases and Clinical Pharmacology at UCSF. She currently serves as the Vice Chief, Inpatient Medical Services and Hospital Epidemiologist at Zuckerberg San Francisco General Hospital and Trauma Center.
Dr. Winston works with the California Emerging Infections Program as the California Principal Investigator for a multi-site Clostridium difficile surveillance supported by the Centers for Disease Control and Prevention (CDC). She is a member of the steering group for the CDC’s Healthcare-Associated Infections Community Interface.
Dr. Winston has a long-standing interest in graduate and undergraduate medical education and was inducted into UCSF’s Academy of Medical Educators. She was also selected as a member of the UCSF Department of Medicine Council of Master Clinicians.
Episode 31 – Clinical Unknown with Drs. Malevanchik and Winston – Cirrhosis + Dyspnea – Part 1
May 07, 2019
Dr. Lev Malevanchik completed medical school at Thomas Jefferson University and is finishing his third year of internal medicine residency at the University of California, San Francisco. This summer, he will start a fellowship in academic hospital medicine at UCSF focusing on medical education, point of care ultrasound, and improving the care of hospitalized patients with limited English proficiency. In his spare time, he loves going indoor rock climbing, listening to This American Life, and playing with his little dog Paprika.
Dr. Lisa Winston
Lisa Winston, MD is Professor of Medicine, Divisions of HIV/ID/Global Medicine and Hospital Medicine, University of California, San Francisco (UCSF). She completed medical school at the Johns Hopkins University School of Medicine. She was a resident in Internal Medicine, a chief resident, and a fellow in Infectious Diseases and Clinical Pharmacology at UCSF. She currently serves as the Vice Chief, Inpatient Medical Services and Hospital Epidemiologist at Zuckerberg San Francisco General Hospital and Trauma Center.
Dr. Winston works with the California Emerging Infections Program as the California Principal Investigator for a multi-site Clostridium difficile surveillance supported by the Centers for Disease Control and Prevention (CDC). She is a member of the steering group for the CDC’s Healthcare-Associated Infections Community Interface.
Dr. Winston has a long-standing interest in graduate and undergraduate medical education and was inducted into UCSF’s Academy of Medical Educators. She was also selected as a member of the UCSF Department of Medicine Council of Master Clinicians.
Episode 30 – Anion gap metabolic acidosis
May 01, 2019
Dan grew up in Gig Harbor, WA (a small town outside of Seattle). He studied neurobiology at the University of Washington and then spent a year in Argentina working in a basic science lab after graduation. He moved to San Francisco to attend medical school at UCSF. He stayed on for internal medicine residency and is currently in the middle of his intern year. He is considering fellowship in infectious diseases and ultimately wants to be a physician educator focusing on clinical reasoning. His hobbies include traveling, cooking, and jogging in golden gate park
Hannah Abrams
Hannah Abrams is a 3rd year medical student at Baylor College of Medicine, applying to Internal Medicine residency programs in the fall. In her spare time she rotates at Kashlak Memorial Hospital, home of the podcast The Curbsiders, where she is a social media editor and episode producer.
Madeline Eckenrode graduated from Wake Forest School of Medicine and is a fourth year med-peds resident at the University of Alabama at Birmingham. She is passionate about medical education and is excited to be staying at UAB next year doing both adult primary care and pediatric hospital medicine. In her spare time she enjoys reading (and is proud of the book club she started in Birmingham), doing calligraphy, and traveling.
Dr. Robert Centor
Dr. Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama.
Dr. Sullivan graduated from the Pritzker School of Medicine at the University of Chicago. She is a 3rd year resident of the UCSF Internal Medicine Residency Program in San Francisco. Next year, Dr. Sullivan will stay at UCSF to be a chief resident internal medicine at the Zuckerberg San Francisco General Hospital. Her clinical interests include health care disparities, pulmonary & critical care, nutrition and medical education. When away from the hospital, she loves to cook, spend time in the ocean and listen to music.
Dr. Sarah Goglin
Dr. Goglin is assistant professor at UCSF in the division of rheumatology. She cares for patients at UCSF in the lupus and vasculitis clinics and at ZSFG in the general rheumatology clinic. She is involved in many aspects of UCSF medical student, medicine resident, and rheumatology fellow education, including serving as an assistant program director for the Internal Medicine Residency and directing the Rheumatology elective for fourth year medical students.
Episode 23 – Clinical Unknown with Hannah Abrams + Human Dx Project – Edema + AKI
Mar 27, 2019
Hannah Abrams is a 3rd year medical student at Baylor College of Medicine, applying to Internal Medicine residency programs in the fall. In her spare time she rotates at Kashlak Memorial Hospital, home of the podcast The Curbsiders, where she is a social media editor and episode producer.
Hannah Abrams is a 3rd year medical student at Baylor College of Medicine, applying to Internal Medicine residency programs in the fall. In her spare time she rotates at Kashlak Memorial Hospital, home of the podcast The Curbsiders, where she is a social media editor and episode producer.
Dr. Daniel Restrepo is a Chief Resident at the Massachusetts General Hospital. He completed his undergraduate studies at the University of Florida before graduating from the University of South Florida College of Medicine and then pursuing a residency in Internal Medicine at MGH. Prior to rejoining the residency for a chief year, he served as an academic hospitalist in the MGH Hospital Medicine Unit attending on both teaching and non-teaching services. His primary interests include medical education, bedside teaching, physical diagnosis, POCUS and clinical reasoning. When not in the hospital he enjoys playing music, SCUBA diving and spending time with his wife and two dogs.
Episode 20 – Clinical unknown with Drs. Tom Goslinga and Bob Centor – Abdominal pain and weight loss
Mar 14, 2019
Dr. Tom Goslinga graduated from the University of Michigan Medical School, and is a current Internal Medicine intern at UCSF. He’s from up north in Minnesota, and is glad to not be covered in feet of snow now that he lives in San Francisco. He enjoys exploring the city while listening to audio books, rock climbing, and going on disastrous but memorable backpacking trips.
Dr. Bob Centor
Dr. Bob Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama. He is Chair of Medicine at Kashlak Memorial Hospital, home of the IM podcast – The Curbsiders. He is an expert diagnostician, teacher, and most importantly a kind and caring human being. Visit his popular blog http://medrants.com and twitter feed @medrants.
Dr. Broderick graduated from Rutgers New Jersey Medical School. He is a 2nd year resident of the Osler Internal Medicine Residency Training Program at Johns Hopkins Hospital. His career interests include Pulmonary & Critical Care Medicine and Medical Education. In his spare time, Dr. Broderick likes to work out, watch the New Jersey Devils, and binge watch Netflix series with his wife.
Dr. Zafia Anklesaria
Dr. Anklesaria graduated from the UCSF Internal Medicine Residency Program. She then completed Pulmonary and Critical care fellowship at UCLA. Her academic interests include clinical problem solving, diagnostic reasoning, resident education, and pulmonary hypertension. She is currently an intensivist at California Hospital, a level 1 trauma center in downtown LA. She is medical director of the pulmonary services at California hospital and is expanding her services into an outpatient pulmonary center. She works closely with family medicine residents on their ICU rotation and is involved in creating their curriculum and weekly didactic sessions on general internal medicine, pulmonary, and ICU topics. Outside the hospital her main passion is horses and horse riding. She also loves traveling around the world scuba diving, hiking with her dog (Dr Isaac Newton) and watching endless re reruns of friends.
Episode 17 – Clinical Unknown with Hannah Abrams + Human Dx Project – Chest Pain + Night sweats
Feb 21, 2019
Hannah Abrams is a 3rd year medical student at Baylor College of Medicine, applying to Internal Medicine residency programs in the fall. In her spare time she rotates at Kashlak Memorial Hospital, home of the podcast The Curbsiders, where she is a social media editor and episode producer.
Episode 15 – Clinical Unknown with Hannah Abrams + Human Dx Project – Chest Pain
Feb 18, 2019
Dr. Stephanie Sherman is a clinician-educator at Baylor College of Medicine (BCM) at Ben Taub General Hospital and the Houston VA Medical Center. She completed medical school at the University of Michigan and internal medicine residency at Massachusetts General Hospital. At BCM, Steph is an associate program director for the internal medicine residency with a focus on resident-as-teacher training, clinical reasoning, and bedside rounding. She is also a contributing editor to the Human Diagnosis Project, an online case-solving platform. If she’s being truthful about how she spends her spare time, she most often finds herself re-watching The Office.
Episode 11 – Clinical Unknown with Reza – Fever and rash
Jan 24, 2019
Dr. Arps graduated from Emory medical school. She is a 3rd year resident of the Osler Internal Medicine Residency Training Program at Johns Hopkins Hospital. She matched at Duke for cardiology fellowship next year. Her academic interests include cardiac critical care as well as research in primary and secondary cardiovascular prevention. In her spare time Dr. Arps likes to run, read biographies, and cook vegetarian dishes.
Dr. Dhaliwal is a clinician-educator and Professor of Medicine at the University of California, San Francisco. He is the site director of the internal medicine clerkship at the San Francisco VA Medical Center, where he teaches medical students and residents in the emergency department, urgent care clinic, inpatient wards, outpatient clinic, and morning report. His academic interests are the cognitive processes underlying diagnostic reasoning and clinical problem-solving and the study of diagnostic expertise. Dr. Dhaliwal enjoys playing pickup basketball with his two sons … even though both can handily defeat him
Episode 8 – Clinical Unknown with Dr. Bob Centor – Hypercalcemia
Jan 05, 2019
Dr. Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama.
Dr. Chew graduated from Baylor College of Medicine. She is an intern in the Internal Medicine Residency Training Program at Johns Hopkins Hospital. She is from Orlando, Florida and enjoys family vacations at the beach, watching British dramas, and hanging out with her co-interns.
 Stay Connected
Stay Connected








































































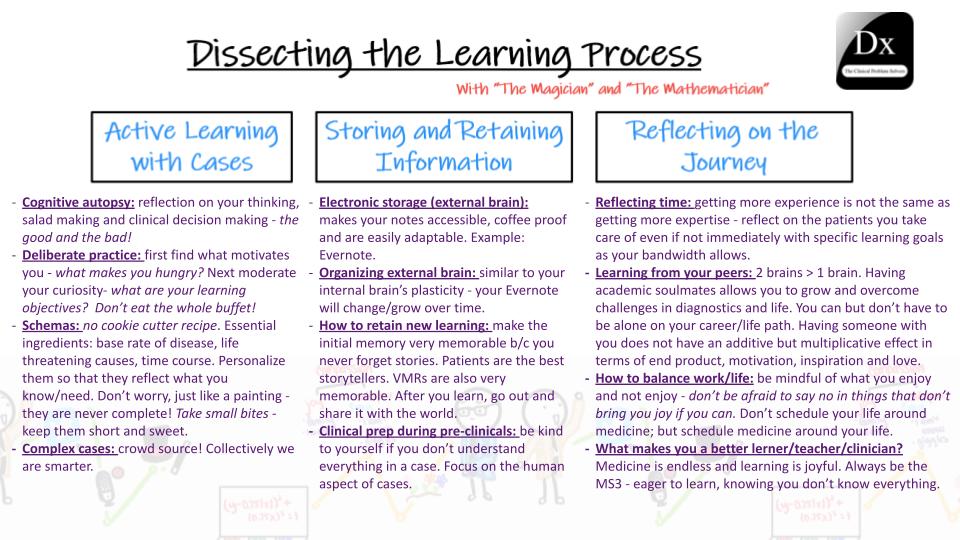






 Dr. Risheen Reejhsinghani is a Clinical Associate Professor in the Division of CardiovascularMedicine at Stanford. She was born in Mumbai, India, where she attended medical college, after spending her early school years in Sydney, Australia. Risheen moved to Boston for residency atSt. Elizabeth’s Medical Center and completed a cardiology fellowship at Baystate Medical Center, the western campus of Tufts University. She then completed an advanced echocardiography fellowship at the University of California, San Francisco.During fellowship, under combined cardiology and rheumatology mentorship, Risheen developed a clinical focus in cardio-rheumatology. This led to the creation of the StanfordCardio-Rheumatology Program, to provide specialized care to patients with cardiac pathology as a direct consequence of autoimmune disease. Risheen cares deeply about medical education and mentorship, and is an Associate Program Director for the CardiovascularMedicine Fellowship, where working closely with fellows is the absolute best part of her role. In the School of Medicine, she serves as an Associate Course Director for the pre-clerkshipPractice of Medicine Course, and is faculty co-lead for the cardiopulmonary block. Her scholarly work addresses curricular interventions and novel methods of teaching to improve education delivery, with the ultimate goal of increasing global access to education for medical trainees.Outside of medicine, Risheen enjoys writing and used to freelance for a newspaper in India.Along with her husband, she tries to travel as frequently as possible and loves learning about local cultures and traditions in the US and internationally. An ardent enthusiast of the alternative rock scene, Risheen has been an unwavering fan of the band Nirvana since well before she could read an EKG.
Dr. Risheen Reejhsinghani is a Clinical Associate Professor in the Division of CardiovascularMedicine at Stanford. She was born in Mumbai, India, where she attended medical college, after spending her early school years in Sydney, Australia. Risheen moved to Boston for residency atSt. Elizabeth’s Medical Center and completed a cardiology fellowship at Baystate Medical Center, the western campus of Tufts University. She then completed an advanced echocardiography fellowship at the University of California, San Francisco.During fellowship, under combined cardiology and rheumatology mentorship, Risheen developed a clinical focus in cardio-rheumatology. This led to the creation of the StanfordCardio-Rheumatology Program, to provide specialized care to patients with cardiac pathology as a direct consequence of autoimmune disease. Risheen cares deeply about medical education and mentorship, and is an Associate Program Director for the CardiovascularMedicine Fellowship, where working closely with fellows is the absolute best part of her role. In the School of Medicine, she serves as an Associate Course Director for the pre-clerkshipPractice of Medicine Course, and is faculty co-lead for the cardiopulmonary block. Her scholarly work addresses curricular interventions and novel methods of teaching to improve education delivery, with the ultimate goal of increasing global access to education for medical trainees.Outside of medicine, Risheen enjoys writing and used to freelance for a newspaper in India.Along with her husband, she tries to travel as frequently as possible and loves learning about local cultures and traditions in the US and internationally. An ardent enthusiast of the alternative rock scene, Risheen has been an unwavering fan of the band Nirvana since well before she could read an EKG. 













 Maria Jimena Aleman
Maria Jimena Aleman









 Dr. Ashita Tolwani, Professor of Medicine at the University of Alabama at Birmingham (UAB). She was the Nephrology Fellowship Training Program Director from 2004-2010 and is now the Associate Program Director. She is also the Director for ICU Nephrology at UAB. (Twitter: luck_urine)
Dr. Ashita Tolwani, Professor of Medicine at the University of Alabama at Birmingham (UAB). She was the Nephrology Fellowship Training Program Director from 2004-2010 and is now the Associate Program Director. She is also the Director for ICU Nephrology at UAB. (Twitter: luck_urine)



 Dr. Vipul Kumar MD PhD is a hematology-oncology fellow at UCSF. He is currently in his second year of fellowship and has a clinical interest in oncology of all forms as well as a passion for teaching.
Dr. Vipul Kumar MD PhD is a hematology-oncology fellow at UCSF. He is currently in his second year of fellowship and has a clinical interest in oncology of all forms as well as a passion for teaching.  Dr. Anand Patel is an assistant professor of medicine at University of Chicago where he treats patients with leukemia and myeloid malignancies. He also serves as medical director of the inpatient leukemia service. His research focuses on the development of clinical trials to help improve the standard of care for patients with high risk leukemias and myeloid malignancies.
Dr. Anand Patel is an assistant professor of medicine at University of Chicago where he treats patients with leukemia and myeloid malignancies. He also serves as medical director of the inpatient leukemia service. His research focuses on the development of clinical trials to help improve the standard of care for patients with high risk leukemias and myeloid malignancies.

























































































































































































































































































 Dr. Sullivan graduated from the Pritzker School of Medicine at the University of Chicago. She is a 3rd year resident of the UCSF Internal Medicine Residency Program in San Francisco. Next year, Dr. Sullivan will stay at UCSF to be a chief resident internal medicine at the Zuckerberg San Francisco General Hospital. Her clinical interests include health care disparities, pulmonary & critical care, nutrition and medical education. When away from the hospital, she loves to cook, spend time in the ocean and listen to music.
Dr. Sullivan graduated from the Pritzker School of Medicine at the University of Chicago. She is a 3rd year resident of the UCSF Internal Medicine Residency Program in San Francisco. Next year, Dr. Sullivan will stay at UCSF to be a chief resident internal medicine at the Zuckerberg San Francisco General Hospital. Her clinical interests include health care disparities, pulmonary & critical care, nutrition and medical education. When away from the hospital, she loves to cook, spend time in the ocean and listen to music.


 Dr. Bob Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama. He is Chair of Medicine at Kashlak Memorial Hospital, home of the IM podcast – The Curbsiders. He is an expert diagnostician, teacher, and most importantly a kind and caring human being. Visit his popular blog
Dr. Bob Centor is Professor Emeritus of Internal Medicine at the University of Alabama at Birmingham, Chair Emeritus for the Board of Regents for the American College of Physicians (ACP) and a retired Dean working part-time at Huntsville and the VA in Alabama. He is Chair of Medicine at Kashlak Memorial Hospital, home of the IM podcast – The Curbsiders. He is an expert diagnostician, teacher, and most importantly a kind and caring human being. Visit his popular blog