What Is the First-Line Treatment for This Patient’s Eye Pain?
Nov 05, 2019
Welcome to the next episode of The Reveal where we take you inside the mind of a test-taker to deconstruct and connect the dots of a board-style question so you can become a better student, transform how you learn, and excel not only on high-stakes exams, but also in your general medical knowledge. Let’s get started.
Episode 18 is limited to audio only, but video returns for episode 19.
A 21-year-old woman presents with pain, tearing, photophobia, and left eye redness. She has been wearing her contact lenses continuously for the last two weeks. A slit lamp examination reveals a white, hazy opacity on the cornea at the 3 o’clock position of the cornea with associated limbal flush. Which of the following is the most appropriate pharmacotherapy?
A. Topical acyclovir
B. Topical amphotericin B
C. Topical ciprofloxacin
D. Topical cyclopentolate
You can find other episodes of The Rosh Reveal podcast here. Remember to subscribe to the podcast and leave us feedback!
Ep 52 Roshcast Emergency Board Review
Feb 25, 2019
Welcome back to RoshCast for Episode 52!For those of you taking the upcoming in-training exam, an early congratulations! All of your hard work will surely pay off soon. Remember to listen to this episode and old episodes as you get closer to the end for more review. Good luck from us at the RoshCast team!
Begin to be now what you will be hereafter.
–William James
Question 1
A 64-year-old woman presents to the emergency department with a right-sided headache. Past medical history includes hypertension, migraines, and polymyalgia rheumatica. Her symptoms started three days ago and have progressively worsened. She states that this headache is different from her previous migraines. It is frontal and she describes it as an ache without radiation of symptoms. She does describe worsening of symptoms with eating as well as when she brushes her hair. She admits to feeling more tired the last couple of days as well as having partial vision loss in the right eye. She denies any nausea or vomiting. Vital signs demonstrate a temperature of 38°C but otherwise are within normal limits. Physical examination is remarkable for tenderness to palpation over the right temple and visual acuities of 20/40 OS and 20/80 OD. What is the most appropriate next step in this patient’s management?
A. Intravenous methylprednisolone
B. Obtain erythrocyte sedimentation rate and C-reactive protein to confirm the diagnosis
A 42-year-old man presents to the emergency department with lower back pain that started acutely while lifting a couch. He complains of pain radiating to the right posterolateral calf. He denies any bowel or bladder incontinence. On examination, he has decreased plantar flexion at the right ankle and numbness of the right lateral foot. Disk herniation at which level is most likely responsible for his findings?
A 27-year-old man presents to the ED with left-hand pain. He was at work as an auto mechanic when he accidentally injected his left index finger with a grease gun. On physical exam, the digit is swollen with a central pinhole wound. The remainder of the hand exam is unremarkable. Which of the following will best determine the amount of tissue damage a substance will cause?
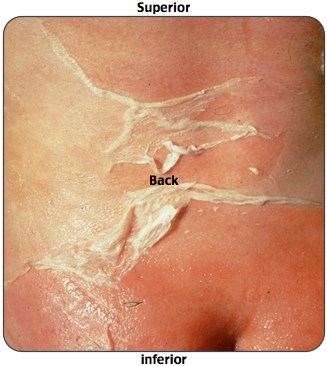
A 5-year-old girl presents to the ED with a rash that started on her face and spread to her neck, axillae, and groin. Mom states that the patient had an upper respiratory infection one week prior. On examination, the patient’s rash is tender to the touch. Which of the following statements regarding the diagnosis of this patient’s condition is correct?
A. Deep layers of the dermis are involved
B. It often leaves the patient disfigured from scarring
C. Mucous membrane involvement is common
D. The disease is caused by an exotoxin producing bacteria
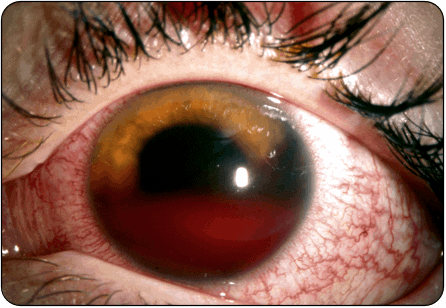
A 22-year-old man complains of pain, photophobia, and vision loss in his eye. He has a history of sickle cell anemia. His vision is 20/200 in the affected eye. Intraocular pressure is 30 mm Hg in the affected eye. You see the above finding on physical exam. Which of the following medications should be immediately administered to this patient?
Vision loss is the most concerning clinical feature in patients with temporal arteritis, whereas jaw claudication is the clinical feature that is most likely associated with a positive temporal artery biopsy.
S1 radiculopathy leads to decreased plantar flexion, numbness to the lateral foot, decreased sensation along the posterolateral calf, and decreased Achilles reflex.
Hepatorenal syndrome leads to arteriolar constriction and the kidneys here would appear normal histologically.
The chemical properties of the substance injected is the primary determinant of damage caused by high-pressure injection injury. While air and clean water have a benign course, paint solvents cause the most severe inflammation.
Staph scalded skin syndrome presents in children less than 5 years old and often follows a URI. The rash starts on the face, neck, axillae, and groin, and there will be a positive Nikolsky sign.
Patients with a spontaneous hyphema present with decreased visual acuity, elevated intraocular pressure, and an afferent pupillary defect. Immediate treatment is with agents that lower intraocular pressure including topical timolol.
That wraps up RoshCast Episode 52! Creating and producing RoshCast has been a ton of fun, but it also takes a ton of time. We are unfortunately halting production for the time being to focus on other projects. We thank you all for your long-time listenership. And don’t forget that there are 51 other episodes. Listen and re-listen on your commute to work, at the gym, or even just at a desk during dedicated study time.
A huge thanks also goes out to all of the folks at Rosh Review who have worked diligently to create high-quality clinical questions. If you need to reach us, please e-mail Nachi at nachig@gmail.com. Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images, and tables, as well as bonus teaching points.
Ep 51 Roshcast Emergency Board Review
Oct 30, 2018
A champion is defined not by their wins but by how they can recover when they fall.
–Serena Williams
Welcome back to RoshCast for Episode 51! For those of you taking the initial certification exam, you’re at the home stretch. Remember to listen to this episode and old episodes as you get closer to the end for more review. Good luck from us at the RoshCast team! We have a great episode for you to get you prepped in your final studies!
Question 1
A 46-year-old man presents with a progressive dull headache over the past 3 weeks. It is worse in the morning and with bending over or coughing. He denies any fever or congestion. For the last two days, he has had associated nausea and three episodes of vomiting. Which of the following characteristics seen on neuroimaging would be most consistent with a glioblastoma?
A. Heterogenous mass with central necrosis
B. Lack of enhancement with administration of contrast
A 16-year-old African American boy presents with a scalp rash. On examination, it is a 5 x 5 cm boggy and thickened area of the right parietal cap with an overlying scaly and crusty plaque and hair loss. The lesion appears yellowish-green under a Wood’s lamp. What is the treatment of choice for this lesion?
A 22-year-old man recently diagnosed with schizophrenia presents to the ED with altered mental status. His blood pressure is 160/80 mm Hg, pulse 130 beats per minute, and temperature is 39.5°C. He is noted to be confused and diaphoretic. He has muscle rigidity and a tremor in his hands. What is the most likely diagnosis?
A 21-year-old woman presents with painful urination. She has no vaginal discharge and is not sexually active. Which of the following is most sensitive for a urinary tract infection on urine dipstick testing?
A 73-year-old man presents with painless vision loss in the right eye. Which of the following on funduscopic examination is most characteristic of central retinal vein occlusion?
Glioblastoma is the most common primary malignant brain tumor in adults and presents as a heterogeneous mass with central necrosis.
A kerion is a boggy, pus-filled lesion caused by a fungalinfection on the scalp. It is treated with a 6 to 8-week course of oral griseofulvin.
New antipsychotic medication administration and a presentation of altered mental status, muscle rigidity, hyperthermia, and autonomic instability is classic for the diagnosis of neuroleptic malignant syndrome.
On urine dipstick, leukocyte esterase is sensitive while nitrites are specific for a urinary tract infection.
Tetralogy of Fallot is the most common cyanoticcongenital heart disease and is associated with a harsh systolic murmur that improves with squatting.
Central retinal vein occlusion presents with sudden, painless, monocularvision loss with the classic “blood and thunder” appearance and retinal hemorrhages.
That wraps up RoshCast Episode 51! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images, and tables, and bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
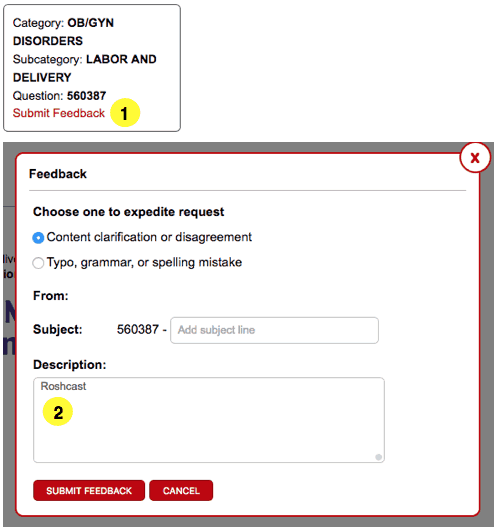
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 50 Roshcast Emergency Board Review
Oct 16, 2018
A hero is someone who has given his or her life to something bigger than oneself.
–Joseph Campbell
Welcome back to RoshCast for Episode 50! Wow!! We can’t believe we’re already at Episode 50. It’s been a real journey building this podcast from the original concept two years ago. And in the last year, we have seen some pretty big changes, including Megha joining the team. We are excited to see how RoshCast continues to evolve over the next fifty episodes and two years.
None of this would be possible without you, our listeners. Your listenership and feedback is what drives us to keep delivering high-quality content! We value every moment you give your attention to us, and we try our best to design the episode to maximize your learning. We have a pretty involved process for choosing questions to present to you and for how we manipulate and deliver the content before we get it to your ears.
With that, let’s kick off a great episode!
Question 1
A 70-year-old woman with history of coronary artery disease, hypertension, and diabetes presents to the emergency department with chest pressure and shortness of breath. Her exam is notable for a new holosystolic murmur best heard over the midaxillary line as well as diffuse bilateral rales. Which of the following is most likely to be seen on this patient’s ECG?
A. Biventricular tachycardia
B. S1Q3T3 pattern
C. ST-depressions in I, V6, and aVL without ST-elevations
A 26-year-old woman with no medical history presents with bleeding gums after brushing her teeth for the last three days. Her complaint was preceded two weeks ago by a URI. Her examination is unremarkable except for oozing from the gums. Labs show a platelet count of 23,000. Which of the following is the most appropriate next step in management?
A. IV immunoglobulin
B. Platelet transfusion
C. Steroids, IV immunoglobulin
D. Steroids, IV immunoglobulin, and platelet transfusion
Which of the following is most suggestive of measles infection?
A. A prodrome of fever, lymphadenopathy, and conjunctivitis followed by a maculopapular rash that starts on the face and spreads to the trunk and limbs
B. Diffuse maculopapular rash with white spots on the buccal mucosa
C. High fever for three days followed by the appearance of a pink maculopapular rash after defervescence
D. Presence of shallow ulcers on oral mucosa and vesicular lesions on the palms and soles
A 23-year-old man who has unprotected, receptive anal intercourse presents to the ED with two weeks of worsening rectal pain and dyschezia. On exam, he has numerous ulcers in the anorectal area and a crop of grouped vesicles containing clear fluid on an erythematous base. The surrounding skin shows no sign of cellulitis or abscess. Which of the following is the most appropriate next step?
A. Refer the patient to a surgeon for operative intervention
B. Send a serology test
C. Send a Tzanck smear
D. Treat with acyclovir
Question 5
A 5-year-old boy with von Willebrand disease presents with persistent bleeding after he lost a tooth 4 hours ago. Vital signs are unremarkable. Physical exam reveals oozing at the site of the tooth which persists despite pressure. Which of the following is the most appropriate treatment?
A 70-year-old man with a history of chronic neck pain presents after a fall. On physical examination, he has a laceration on his chin. Motor strength is 2/5 in his upper extremities and 4/5 in his lower extremities. He has decreased sensation to soft touch in both legs. Which of the following is the most likely diagnosis?
A new holosystolic murmur over the midaxillary line, with signs of heart failure, is consistent with acute mitral valve regurgitation. Think of inferior stemi as a possible cause here.
Immune thrombocytopenia presents with bleeding that is often preceded by a viral illness. It is treated with steroids and IVIG in most cases. For those with severe or life-threatening bleeding, platelet transfusion should be considered as well.
Measles presents with a prodrome of fever and three Cs (coryza, cough, and conjunctivitis) followed by a diffuse maculopapular rash and Koplik spots.
A painful vesicular rash on an erythematous base in the anorectal area is consistent with herpes simplex proctitis. Diagnosis is clinical. Treat with antivirals.
von Willebrand disease presents with mucosal bleeding, and the first-line treatment is desmopressin.
Central cord syndrome is often the result of a hyperextension injury to the cervical spine. It presents with bilateral motor dysfunction that is greater in the upper extremities than the lower extremities.
That wraps up RoshCast Episode 50! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, and bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 49 Roshcast Emergency Board Review
Oct 02, 2018
Life is like riding a bicycle. To keep your balance, you must keep moving.
–Albert Einstein
Welcome back to RoshCast for Episode 49! We have a lot of exciting material in this episode. Definitely don’t skip this one! For those taking the initial certification exam, it’s just around the corner. Go back and listen to old episodes and review.
Question 1
A 14-year-old boy developed an itchy, painful, erythematous rash on his hands, forearms, and face about a day after hiking in nearby woods with some friends. Your exam shows linear erythematous papules over his forearms with similar swelling and erythema around his eyes (including eyelids), cheeks, and forehead. You suspect poison ivy that he reports he has had in the past. Which of the following is most likely to improve the course of his illness?
Which of the following patients will benefit most from receiving tissue plasminogen activator for acute pulmonary embolism detected in the emergency department?
A. 55-year-old man with a history of hypertension with vital signs showing HR 100/min, BP 80/40 mm Hg, R 24/min, and oxygen saturation 92%
B. 55-year-old man with a history of hypertension with vital signs showing HR 145 bpm, BP 136/86 mm Hg, R 24/min, and oxygen saturation 92%
C. 55-year-old woman with a history of hypertension and systemic lupus erythematosus with vital signs showing HR 100 bpm, BP 116/86 mm Hg, R 24/min, and oxygen saturation 85%
D. 55-year-old woman with a history of hypertension with vital signs showing HR 110 bpm, BP 122/80 mm Hg, R 24/min, and oxygen saturation 92% with evidence of right ventricular dysfunction on echocardiogram
A 55-year-old woman presents to the emergency department unresponsive. She and her friend had finished eating 60 minutes earlier when the patient collapsed to the floor while talking. Which of the following foods is most likely the cause?
A 32-year-old woman with no past medical history presents to the emergency department with a four-day history of bloody diarrhea and abdominal cramping. She states that her boyfriend is having similar symptoms but did not want to come to the hospital. Their symptoms started two days after they shared a meal at their favorite fried chicken restaurant. The patient’s vital signs are 37.4℃, HR 89/min, BP 112/70 mm Hg, RR 17/min. Physical examination is significant for moist mucus membranes with brisk capillary refill and mild diffuse tenderness to palpation of the abdomen. Which of the following is the most appropriate management of this patient’s illness?
A. Admit for IV azithromycin and rehydration
B. Admit for IV rehydration and observation for resolution of diarrhea
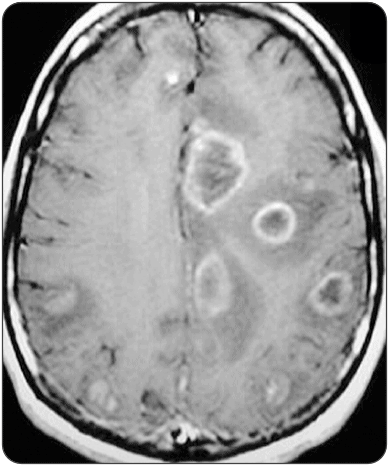
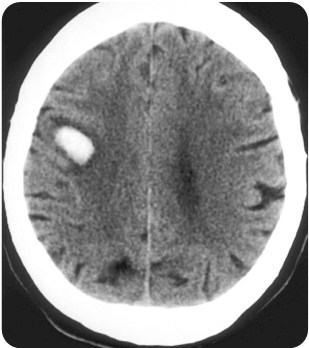
A 54-year-old man with a history of HIV and recent CD4 count of 85 presents with headache for 3 days. The patient’s sister says that he has been increasingly confused over the last 3 days. While in the emergency department, he has a seizure which resolves spontaneously. Electrolytes are within normal limits. A CT scan is performed and is shown above. Which of the following medication regimens should be given?
Localized reaction from poison ivy can be treated with topical high-potency corticosteroids. Extensive reactions or reactions involving the face or genitalia need a 2–3-week course of tapering systemic steroids.
Persistent hypotension or shock due to acute pulmonary embolism is the only widely accepted indication for systemic thrombolysis.
Severe metabolic acidosis is a hallmark feature of cyanide poisoning and treatment is with hydroxycobalamin.
Lightning strikes cause injuries via both acute thermal radiation and widespread electrical damage. Intense thermal radiation can cause tympanic membraneperforation.
Undercooked poultry is associated with infection from Campylobacter jejuni. This can present with bloody diarrhea, abdominal cramping, and vomiting. Treatment is with fluoroquinolones or azithromycin.
Subcortical, ring-enhancing lesions on a CT of the brain in an HIV patient with a CD4 < 100 is indicative of toxoplasmosis and treatment is with pyrimethamine, sulfadiazine, and leucovorin.
CNS lymphoma also causes ring-enhancing lesions in patients with AIDS but lesions in this case are usually solitary and located in the periventricular white matter. Symptoms are usually gradually progressive over months rather than days.
That wraps up RoshCast Episode 49! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 48 Roshcast Emergency Board Review
Sep 18, 2018
Success is not final, failure is not fatal: it is the courage to continue that counts.
–Winston Churchill
Welcome back to RoshCast for Episode 48! We’re going to jump right into questions this week. Remember to send us feedback for any changes you would like to see at roshcast@roshreview.com.
Question 1
An 8-year-old previously healthy boy presents with back pain and fever for 4 days. He complains of pain in the low back, which is increased with bending or twisting. The pain radiates down into his left leg. He denies trauma. Physical exam is remarkable only for tenderness to palpation over the lumbar spine. What management is indicated
A 40-year-old man is brought to the emergency department after being assaulted during a bar fight. He has proptosis of the right eye with a measured intraocular pressure of 50 mm Hg. A lateral canthotomy is started. Once the Kelly clamp is released from the lateral canthus, what is the appropriate next step?
A. Clamp the medial canthus
B. Cut the inferior crus of the lateral canthal tendon
C. Cut the superior crus of the lateral canthal tendon
A 25-year-old man presents to the emergency department after sustaining burns to the hands, legs, and chest after falling into a bonfire. On physical examination, there are partial-thickness burns on the upper half of the anterior torso along with the bilateral palms of the hands and bilateral anterior legs. He weighs 70 kg. You begin to initiate fluid resuscitation using the Parkland formula. How much fluid should this patient receive in the first eight hours?
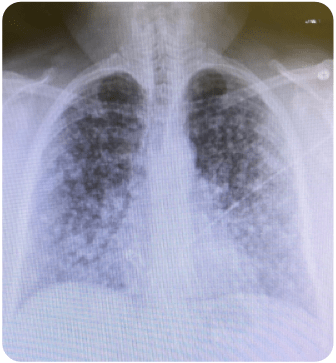
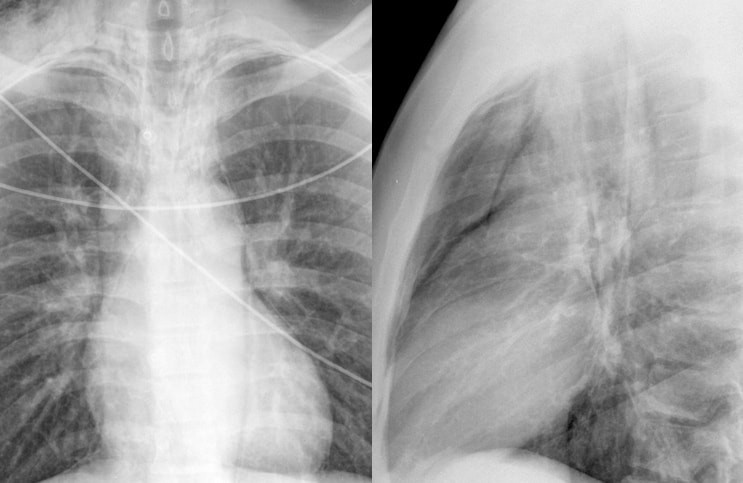
A 64-year-old man presents to the emergency department with cough and shortness of breath that has progressively been worsening over the last several weeks. He has also been more fatigued and is unable to get around the house anymore. He denies fever and night sweats. He has a past medical history of hypertension and takes lisinopril daily. He is an immigrant from Argentina where he used to work as a miner. He denies tobacco use. What is the most likely diagnosis based on this chest radiograph?
A 53-year-old man presents with numbness to his right hand for three to four months. He states that he has numbness with waking up in the morning, which gets better when he shakes his hands. The patient indicates numbness to his first, second, and third digits on the right hand. Which of the following tests is most sensitive for this diagnosis?
A young man is involved in a motor vehicle collision and sustains a severe head injury. In the ED, his GCS is 7. His blood pressure is 115/70 mm Hg and heart rate is 85 beats per minute. His pupils are 3 mm and equal and reactive to light. You intubate the patient and place him on a mechanical ventilator. The FAST ultrasound is negative and there are no other obvious injuries. Which of the following is the most important principle to follow in the management of this patient?
A. Administer mannitol
B. Avoid hypotension
C. Hyperventilation
D. Initiate induced hypothermia
Discitis presents with severe localized radiating pain. The lumbar spine is most commonly involved, and treatment is with IV antibiotics.
A lateral canthotomy is performed to relieve intraocular pressure from a retrobulbar hematoma or a postseptal hemorrhage. It is done by cutting the inferior crus of the lateral canthal tendon.
The Parkland Formula is used to determine the volume of fluid required for resuscitation of burn patients. It is 4 mL x body weight in kg x % total body surface area of the burn. Half of this fluid is given within the first 8 hours and then other half over the next 16 hours.
Pneumoconiosis is a restrictive lung disease that can be caused by inhalation of dust, often in mines. It presents with bilateral ground glass opacities on Chest X-ray.
The Median Nerve Compression Test is the most sensitive test for confirming carpal tunnel syndrome. It consists of direct pressure application to the median nerve at the carpal tunnel.
Hypotension and hypoxia have both been shown to have a devastating effect on the outcome of patients with traumatic brain injury.
That wraps up RoshCast Episode 48! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, and bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 47 Roshcast Emergency Board Review
Sep 04, 2018
If you fell down yesterday, stand up today.
–H. G. Wells
Welcome back to RoshCast for Episode 47! Let’s kick off this episode with a review of Neisseria meningitides, an important topic for clinical practice and personal safety.
Neisseria meningitides is highly contagious and antibiotic prophylaxis is indicated for close contacts of an infected patient, including those in contact with secretions as well as members of the same household or daycare center.
Healthcare workers with close contact with the patient’s secretions should also receive prophylaxis.
There are three options for prophylaxis:
Rifampin is administered at a dose of 10 mg/kg with a max dose of 600 mg every 12 hours for 4 doses, and this is 100% effective as far as we know.
Ceftriaxone 250 mg IM can be given for 1 dose, which is 97–100% effective.
The least effective option is Ciprofloxacin 500 mgPO for 1 dose, and that’s 90–95% effective.
Even though rifampin is the most effective, be wary of its side effects, which include turning secretions like tears and urineorange. Contact lens wearers should be warned of permanent staining.
A 33-year-old woman presents to the ED with agitation and severe respiratory distress. She has been taking a significant amount of “pain medication” for low back pain, according to her son. The patient is screaming about her “ears ringing.” Vital signs are BP 100/60 mm Hg, HR 140 beats per minute, RR 35 breaths per minute, and T 100.1°F. Which of the following complications is she at risk of developing?
A. Hemodynamically significant lower gastrointestinal bleeding
A 62-year-old woman presents to the emergency department with dizziness. She describes the events as a spinning sensation that is worse with position changes. The dizziness is associated with hearing loss as well as tinnitus and vomiting. She notes it started three days ago and that she has had multiple episodes all lasting less than a day since that time. On physical examination, horizontal nystagmus is present as is decreased hearing on the left. The remainder of the ear and neurologic examination is within normal limits. A head CT and brain MRI are performed and are negative. Which of the following is the most likely diagnosis?
A 28-year old woman presents with several painful ulcers she has developed in the vaginal area. Examination reveals multiple 0.5 cm to 1.5 cm oval ulcers with sharply defined borders and a yellowish-white membrane. She denies recent sexual activity. Except for recurring aphthous ulcers of her mouth, her past history is unremarkable. At this time, which of the following is the most likely diagnosis?
A 65-year-old man on peritoneal dialysis presents because his dialysis effluent is cloudy. You send it for culture and Gram staining, which returns with a preliminary result of gram-positive cocci in clusters. Vital signs are BP 125/70 mm Hg, HR 80 bpm, RR 14/min, and T 98.5°F. Other than abdominal ascites, the physical exam is unremarkable. Which of the following is the most appropriate management for this condition?
A. Inpatient management with antibiotics and temporary hemodialysis
B. Inpatient management with IV antibiotics
C. Outpatient management with intraperitoneal antibiotics
Salicylates, opioids, naloxone, phencyclidine, and meprobamate can cause noncardiogenic pulmonary edema.
Patients with acute salicylate toxicity with levels greater than 100 mg/dL and chronic toxicity with levels greater than 60 mg/dL require dialysis.
Neurologic sequelae from carbon monoxide poisoning can be identified radiographically within 12 hours of exposure as symmetric hypodense lesions in the basal ganglia.
Meniere disease is a set of episodic symptoms including vertigo, hearing loss, tinnitus, and a sense of fullness in the ear. Episodes last anywhere from 20 minutes to 4 hours.
Behcet syndrome presents as recurring genital and oral ulcerations and also relapsing uveitis.
Peritonitis is the most common complication of peritoneal dialysis, and it can often be treated with intraperitonealantibiotics as an outpatient.
Infantile spasms present before the age of one and EEG shows hypsarrhythmia. This is treated with corticotropin.
That wraps up RoshCast Episode 47! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, and bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the Submit Feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 46 Roshcast Emergency Board Review
Aug 21, 2018
Only those who dare to fail greatly can ever achieve greatly.
–Robert F. Kennedy
Welcome back to RoshCast for Episode 46! Let’s kick off this episode with a rapid review of molluscum contagiosum.
Molloscum contagiosum is caused by poxvirus. It is seen in children, sexually active adults, and immunocompromised patients like those with HIV.
The rash presents as painless, pearly, umbilicate papules, and it is spread by direct skin-to-skin contact.
Children present with lesions on the face, trunk, and extremities, whereas sexually active adults can present with lesions in the genital regions, lower abdomen, and thighs. The rash tends to spare the palms and soles.
Most patient will not require therapy with spontaneous resolution occurring in months. Those with extensive lesions may benefit from cryotherapy.
HIV positive patients with a CD4 count less than 100 are at greater risk for developing molluscum contagiosum.
A 26-year-old man presents to the ED after being hit in the head by a foul baseball. The patient was initially alert and talking to you. He is now becoming progressively more somnolent. Which of the following would you expect to see on a non-contrast computed tomography scan of the head?
A. A collection of blood layering in the basilar cisterns
B. A crescent-shaped frontal hematoma crossing suture lines
C. A lenticular-shaped hematoma in the temporal region
D. An intraparenchymal hemorrhage within the frontal lobe
A 55-year-old man who is taking several antihypertensive medications presents to the ED with nausea, vomiting, shortness of breath, and a rash after eating a home-cooked Thai meal at a friend’s house about one hour ago. The symptoms began within seconds of the first bite of his meal. Despite the patient being administered 2 doses of intramuscular epinephrine, diphenhydramine, dexamethasone, and crystalloid fluids, his blood pressure remains at 75/38 mm Hg. Which other medication should be considered in this patient?
A. Cimetidine
B. Glucagon
C. Norepinephrine
D. Octreotide
Question 4
A 36-year-old man presents to the ED after having a seizure. He has a folder full of medical records dating back 15 years. Several of the records are from other cities and states. It is now 11:00 pm on a Friday night. His primary care physician, neurologist, and psychiatrist are “out of town,” and he believes that he needs to be admitted for the duration of the weekend. He has another episode in the ED and immediately following this he returns to his baseline. He is now awake and alert. You immediately draw a serum lactate and it is normal. Which of the following diagnoses should be strongly considered in this patient?
A 4-year-old boy is brought to the emergency department by his parents after they found him in the backyard shed choking and gagging. Before this event, he was otherwise healthy. His temperature is 101°F, heart rate is 95 bpm, blood pressure is 100/60 mm Hg, and respiratory rate 40/min. On exam, he appears sleepy but continues to cough. Pulmonary findings include moderate retractions and diffuse wheezes. A chest X-ray shows patchy infiltrates. What is the most likely diagnosis?
A 12-year-old boy presents to the ED after his brother bumped into his elbow while he was using a cotton-tipped swab to clean out his ear. He denies dizziness, vertigo, nausea, or hearing loss. On exam, you note a tear of the tympanic membrane and a small amount of blood in the external canal. Which of the following is the most appropriate next step in management?
A. Begin antibiotics
B. Discharge with instructions to keep the ear canal dry
Anaerobes like Prevotella, Bacteroides, Fusobacterium, and Peptostreptococcus are the most common organisms found in a lung abscess.
On chest radiograph, lung abscesses present as a consolidation with an air fluid level inside a cavitary lesion.
An epidural hematoma presents as a hyperdense lenticular-shaped hematoma in the temporal region, and it is caused by a tear in the middle meningeal artery. A lucid interval is often associated with this bleed.
Patients taking beta-blockers for hypertension may exhibit persistent hypotension in the setting of anaphylactic shock. They should be treated with glucagon to free up the beta receptor and potentiate the circulating epinephrine to restore vasomotor tone.
In Munchausen syndrome, the individual feigns disease in an attempt to gain attention, sympathy, or reassurance.
Somatization disorder is characterized by unexplained physical symptoms that lead to significant social and occupational impairment.
Conversion disorder is characterized by an unexplained neurologic symptom triggered by a psychological stressor.
Hydrocarbon ingestion can cause pneumonitis, and the chest X-ray can show diffuse bilateral infiltrates.
Patients with asymptomatic ruptured tympanic membranes can be discharged home with instructions to keep the canal dry. Symptomatic patients require emergent ENT consultation.
That wraps up RoshCast Episode 46! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, and bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the Submit Feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 45 Roshcast Emergency Board Review
Aug 07, 2018
There is only one corner of the universe you can be certain of improving, and that’s your own self.
–Aldous Huxley
Welcome back to RoshCast for Episode 45! Let’s start out with a review of rabies before getting to core content Q&A.
The most common wild reservoirs of rabies are raccoons, skunks, bats, foxes, and coyotes. Domestic animals like cats, dogs, and cattle can also get rabies. Rodents, reptiles, and birds on the other hand are not carriers and cannot transmit rabies.
One important factor in deciding if you get rabies postexposure prophylaxis is whether the animalcan be foundand held for observation.
The rabies postexposure prophylaxis has two parts: the immunoglobulin and the vaccine.
When giving rabies postexposure prophylaxis, inject the immunoglobulininto the wound and start the rabies vaccine series which the patient will receive on days 1, 3, 7, 14, and 28.
Now onto this week’s podcast
Question 1
Which of the following is true regarding acute respiratory distress syndrome?
A. Define as PaO2:FiO2 > 300
B. Empiric corticosteroids should be given
C. Positive end-expiratory pressure should be increased with increases in FiO2
D. Tidal volume should be started at 10 mL/kg in intubated patients
A 35-year-old man presents to the ED after being assaulted in a bar fight. He has signs of significant facial trauma. On physical exam, you note a tooth fracture through the enamel and dentin but does not involve the pulp. Which of the following is the most appropriate next step in management of his dental injury?
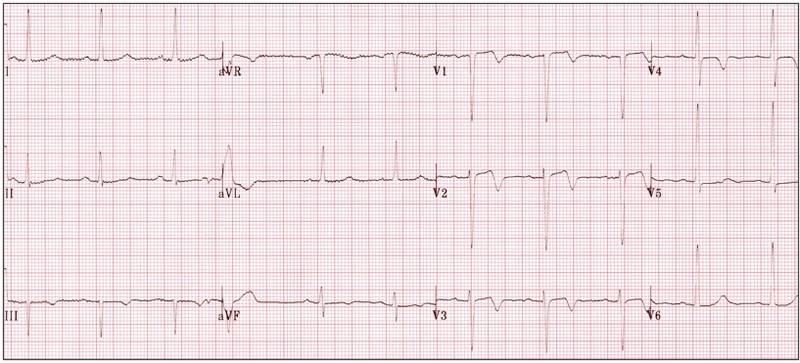
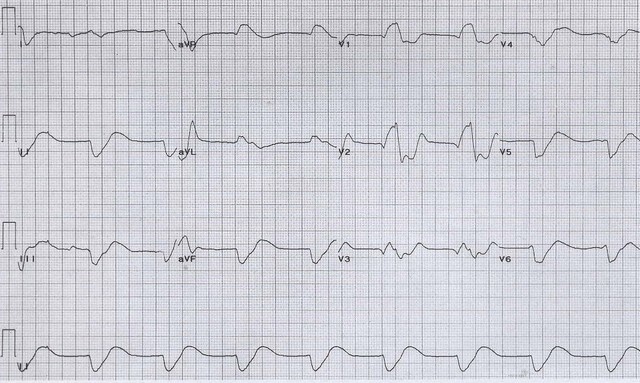
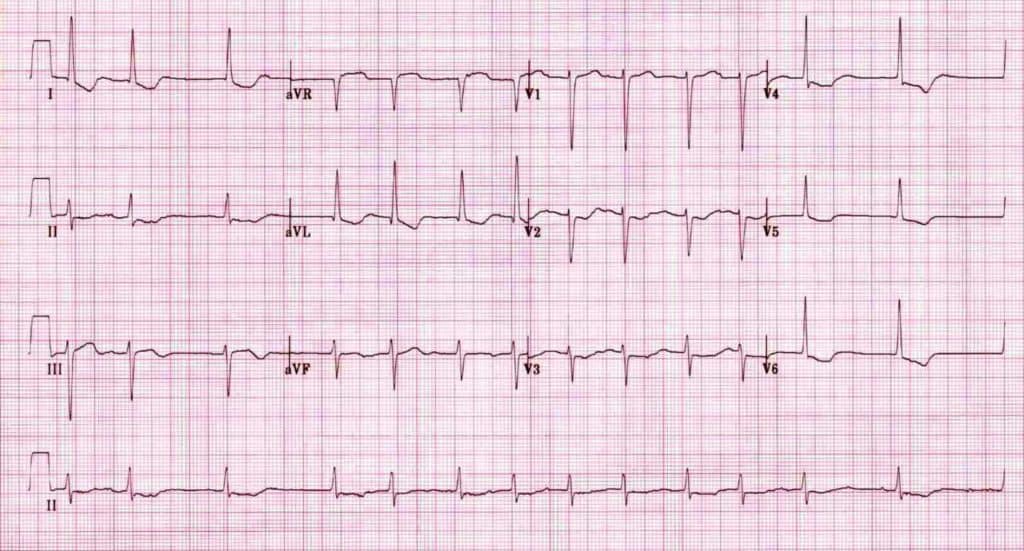
A 62-year-old man presents with acute onset of chest pain with radiation to the shoulders and nausea while walking his dog. On examination, he is diaphoretic with heart rate 94 bpm, respiratory rate 20 bpm, blood pressure 92/59 mm Hg, and oxygen saturation 96% on room air. His ECG reveals 2 mm elevation in aVR. Occlusion of which coronary artery is most likely responsible for this patient’s presentation?
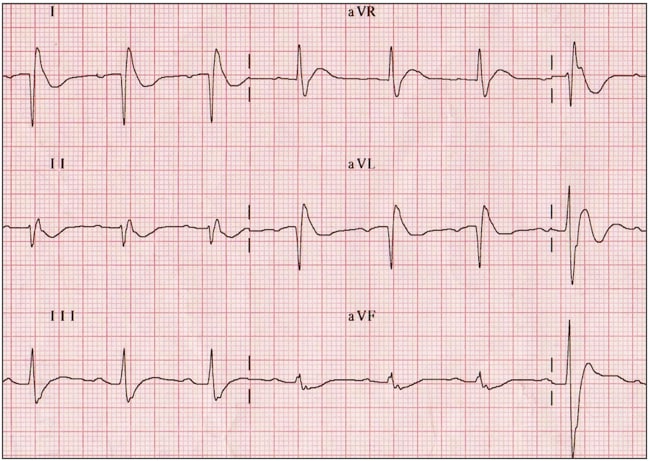
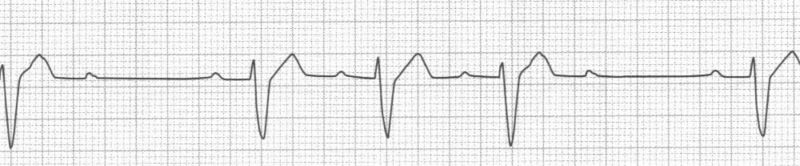
A 62-year-old man presents for evaluation of chest pain. Approximately three weeks ago the patient had a myocardial infarction with stent placement. Last evening he developed pleuritic chest pain and fever. He has no cough and does not feel short of breath. His ECG is shown above. Which of the following is the most likely diagnosis?
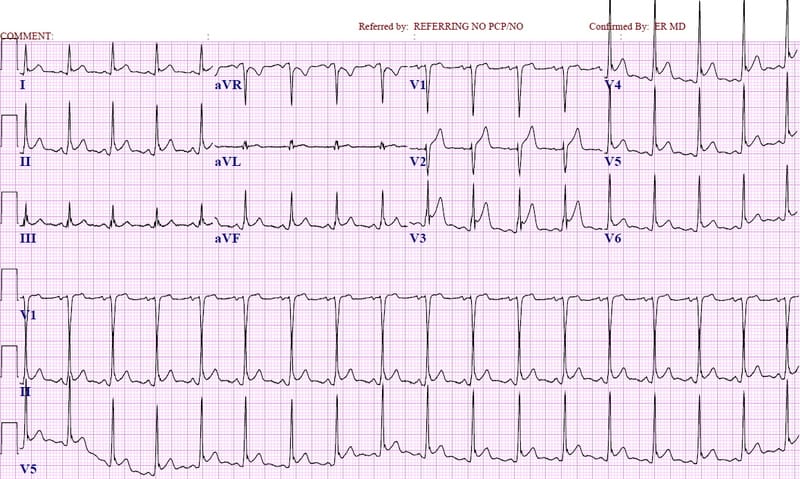
A 45-year-old man with a history of hypercholesterolemia presents with acute onset of anterior chest pain, nausea, and diaphoresis. His ECG is distinct for upsloping ST elevation in AVR (≥ 1 mm) with ST depressions and tall T waves in the precordial leads. What is the most likely diagnosis?
A. Occlusion of the left circumflex artery
B. Occlusion of the left main coronary artery
C. Occlusion of the proximal left anterior descending artery
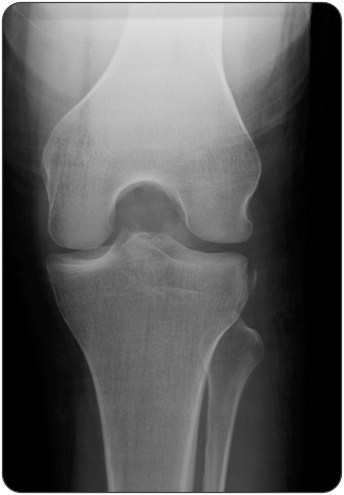
A 25-year-old man presents the emergency department with knee pain. This morning he slipped on the ice and felt a pop in his knee. On physical exam his left knee appears to have a moderate effusion with limited range of motion and medial joint line tenderness. An X-ray of the left knee is performed. A pedunculated, bony exostosis with well-defined margins is seen along the distal lateral femur on the AP view of the knee. What is the most likely diagnosis of the incidental bone lesion?
Intubated patients with ARDS should be started on low tidal volumes of 6–8 cc/kg of ideal body weight, and the PEEP and FiO2 should be titrated up together.
The PaO2 to FiO2 ratio in patients with ARDS is < 300. The lower the ratio, the worse the disease process.
There are three classes of dental fractures:
Ellis Class I involves injury to the enamel alone and is treated by smoothing any rough edges.
Ellis Class II involves injury to the dentin and enamel. This is treated by coveringexposed dentin with calcium hydroxide.
Ellis Class III involves the pulp along with the dentin and enamel. These usually require antibiotics and immediate dentalconsult.
ST segment elevation in aVRgreater than 1 mm or greater than the ST segment elevation in V1 is most concerning for occlusion of the left main coronary artery.
Dressler syndrome is pericarditis occuring one week to several months after an MI.
A left ventricular aneurysm is a complication of a large anterior wall MI. EKG shows ST segment elevations in the anterior leads.
De Winter ECG patterns presents with tall, prominent symmetric T waves in the precordial leads with upsloping ST segment depression greater than 1mm at the J point and ST segment elevation may be seen in aVR
De Winter EKG is a STEMI equivalent and represents acute LAD occlusion.
Aneurysmal bone cyst, osteochondroma, and osteoid osteoma are benign bone lesions.
Osteosarcoma is a malignant bone lesion seen on X-ray as a lytic lesion, a blastic lesion, or a heavily ossified mass.
That wraps up RoshCast Episode 45! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast and @RoshReview. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast. We’re also launching on Google Play in the near future.
Ep 44 Roshcast Emergency Board Review
Jul 24, 2018
By failing to prepare, you are preparing to fail.
–Benjamin Franklin
Welcome back to RoshCast for Episode 44! We are back to an every other week schedule covering core content. Let’s start out with a rapid review of neonatal conjunctivitis.
The three dangerous causes of neonatal conjunctivitis that you need to consider in the ED are gonorrhea, chlamydia, and herpes.
Gonorrhea is the most aggressive bacteria associated with neonatal conjunctivitis. It presents in the first week of life with purulent drainage and ulcerations, and it can disseminate to cause gonococcal sepsis. Culture the drainage for confirmation, and treat the baby with cefotaxime.
Chlamydianeonatal conjunctivitis, which presents in the first month of life, can disseminate into the lungs. Treat with oral erythromycin.
The third and least dangerous cause of neonatal conjunctivitis is herpetic. In this case you may see vesicles in the eye. Treat this with IV acyclovir.
Now onto this week’s podcast
Question 1
A 21-year-old man presents after he was bitten by a spider. He has a picture of the spider on his phone (shown above). Which of the following is a potential complication of a bite by this spider?
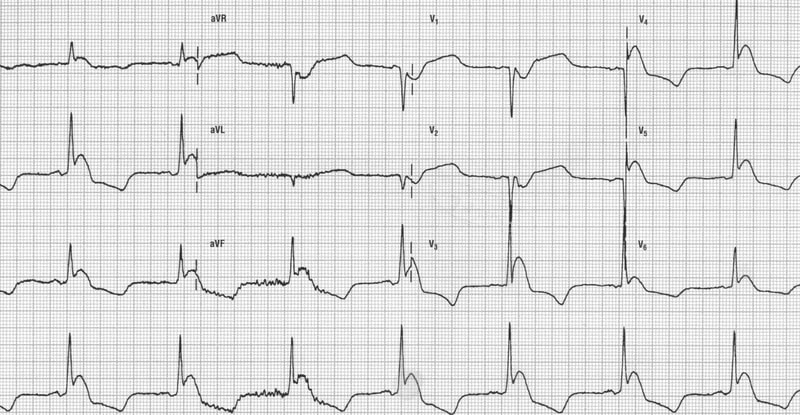
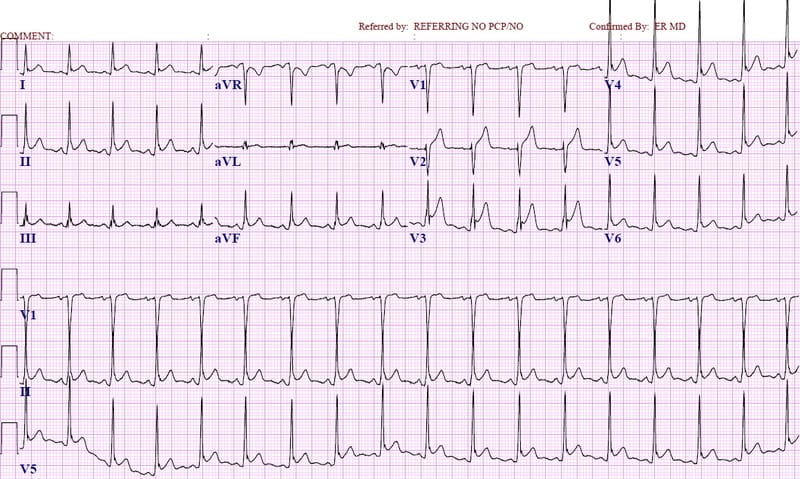
A 66-year-old man with hypertension and hyperlipidemia presents after an episode of severe chest pain while walking to work. He is currently asymptomatic. His vitals are T 36.27°C, HR 76/min, BP 143/85 mm Hg, RR 18/min, and oxygen saturation 99%. A 12-lead ECG is performed as seen above. Which of the following is the most appropriate next step in management?
A. Give 325 mg of aspirin, and activate the cardiac catheterization lab
B. Give 325 mg of aspirin, and admit for serial troponin testing and stress test
C. Give 325 mg of aspirin, and discharge home with cardiology follow-up in 24–48 hours
D. Send d-dimer, and consider CT pulmonary angiogram if elevated
A 17-year-old boy from New Jersey presents with a 3-day history of rash and a 1-day history of facial droop. He also complains of a headache. The images above represent the physical examination findings. In addition you note mild nuchal rigidity. A noncontrast head CT is performed and is normal. Which of the following is the next best step for this patient?
A 52-year-old man presents with decreased sensation in the upper extremities and chronic neck pain. He states that the loss of sensation has been progressive for months. On physical examination, he has decreased sensation to pain over the upper back, shoulders, and arms with intact proprioception and light touch. What disorder does this patient exhibit?
A patient with metastatic breast cancer presents with weakness and nausea. An ECG is shown above. What electrolyte abnormality is likely in this patient?
Brown recluse spiders have violin-shaped markings on their back. The toxin here can lead to hematologic abnormalities. There is no antivenin available in the US.
Black widow spiders, on the other hand, have a red hourglass shape on their ventral surface and their toxin causes autonomic instability and abdominal wall rigidity. There is an antivenin available, but it’s only used in severe cases.
Wellen’s syndrome type A demonstrates biphasic T waves in V1–V3 and type B demonstrates deeply inverted T waves in V1–V3. It is highly specific for a criticalstenosis of the LAD. Activate the catheterization lab!
There are three stages of Lyme disease:
Early Lyme manifests with the classic erythema migrans rash.
The second stage is acute disseminated infection which results in neurologic, cardiac, arthritic, and ophthalmic manifestations.
The third is late Lyme disease, which presents with worse neurologic manifestations and chronic Lyme arthritis.
The most common location of syringomyelia is the cervical spine. Patients present with a cape-like distribution of loss of pain and temperature sensation in the upper extremities with preservation of light touch and proprioception.
Anterior cord syndrome is characterized by loss of motor function below the lesion and preservation of position, touch, and vibration sensation.
Brown-Sequard syndrome presents with ipsilateral motor function loss and contralateral pain and temperature sensation loss.
Central cord syndrome presents with bilateral motor paresis and sensory impairment.
The most frequently seen oculomotor sign in Wernicke encephalopathy is lateral nystagmus.
Diagnosis of Wernicke encephalopathy requires two out of four of the following criteria: dietary deficiencies, oculomotor dysfunction, cerebellar dysfunction, and altered mental status.
Hypercalcemia can cause QT shortening, while hypocalcemia can cause QT prolongation.
Malignancy is the most commoninpatient cause of hypercalcemia while primary hyperparathyroidism is the most common outpatient cause.
That wraps up RoshCast Episode 44! Be sure to also check out the rest of the Rosh Review Blog for questions from prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast and @RoshReview. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions.
You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast. We’re launching on Google Play in the near future also.
Ep 43 Roshcast Emergency Board Review
Jul 10, 2018
Always do your best. What you plant now, you will harvest later.
–Og Mandino
Welcome back to RoshCast for Episode 43! After a long pause, we are back with new episodes and a lot of announcements. A lot has happened in the past few months. Jeff had a baby and moved to Pittsburg to start his EMS fellowship. In doing so, he is taking a break from Roshcast to focus on fellowship and his new baby. Megha Rajpal, a fourth-year resident at Mount Sinai, will be taking over as co-host.
For epiglottitis, the patient will usually have a rapid-onset fever and dysphagia. On exam, they could be leaning forward, drooling, and even have inspiratorystridor.
The typical radiographic finding for epiglottitis is thumbprint sign, which is seen on a lateral neck film.
The most common bacteria associated with epiglottitis are H. influenzae and Streptococcus.
For management in epiglottitis, airway is the crucial piece. Patients may need to be intubated immediately. Don’t forget to start the patient on antibiotics to treat for the common pathogens.
Now onto this week’s podcast
Question 1
Which of the following is the most common presenting vital sign abnormality seen in patients presenting with a pulmonary embolism?
A 72-year-old man presents with pain in the right knee. It has increased over the last 24 hours with redness and swelling. Joint aspiration reveals negative birefringent crystals. He reports an allergy to NSAIDs and is a brittle diabetic. Colchicine is prescribed. Which side effect limits its usefulness due to a narrow therapeutic window?
A patient presents to the ED after waking up and finding that he was drooling while drinking his coffee. When he looked in the mirror he noticed that the left side of his face was drooping. Which of the following findings is suggestive of a central process?
A 28-year-old man presents to the emergency department via ambulance after a terrorist set off a large bomb in an airport. On physical exam, he has bilateral tympanic membrane ruptures. Chest X-ray shows bilateral pulmonary contusion. These injuries are most consistent with which category of blast injury?
A 19-year-old man presents with eye pain and photophobia in his left eye after being punched there two days ago. He describes blurry vision. On exam, you note consensual photophobia. Which of the following is the most appropriate treatment?
Tachypnea is the most common presenting vital sign abnormality for a pulmonary embolism, while dyspnea at rest or exertion is the most common presenting symptom.
Joint aspiration in gout demonstrates negative birefringent monosodium urate crystals. NSAIDs are the first-linetreatment.
Colchicine can cause severe GI symptoms in more than 10% of patients.
When deciding on a central versus peripheral etiology for facial paralysis, preserved ability to raise the ipsilateral eyebrow or close the ipsilateral eye is more concerning for a central lesion than a peripheral lesion.
Clay shoveler’s fracture is a stable avulsion fracture of the spinous process of C6–C7.
Jefferson burst fracture, bilateral facet dislocation, odontoid type II and type IIIfractures, any fracture with a dislocation, hangman’s fracture, and teardropfracture are all unstable cervical spine fractures.
Primary blast injury occurs from direct effect from blast shockwaves.
Secondary blast injury occurs from the impact of fragments due to exploding devices.
Tertiary blast injury occurs when the blast wave propels the body into objects.
Quaternary blast injury is due to environmental contamination from the device.
In quinary blast injuries, there is bodily absorption of device additives.
Traumatic iritis is treated using cycloplegics like homatropine and topical steroids.
That wraps up RoshCast Episode 43! Rosh Review is excited to announce the launch of a new podcast called The PA Way hosted by Alison Callahan, PA-C. Definitely worth a listen. Be sure to also check out the RoshCast blog for questions from this episode and prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources there to help prepare you for the boards and the wards.
Don’t forget to follow us on twitter @RoshCast and @RoshReview. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 42 Roshcast Emergency Board Review
Feb 22, 2018
The secret of change is to focus all of your energy, not on fighting the old, but on building the new.
–Socrates
Welcome back to RoshCast for Episode 42! With the in-training exam around the corner, go back and power through old episodes during commutes to pick up as many points as possible. Good luck!
Patent ductus arteriosus (or PDA) closes, the neonate will present in heart failure and shock.
Turner’s syndrome is associated with coarctation. Turner’s is also associated with webbed neck, short stature, and low-set ears.
Individuals with Turner’s syndrome are missing an X chromosome as well, making it a 45,XO chromosomal condition.
A blood pressure differential between the arms and legs—specifically, the pressure in the arms is higher than the legs. Depending on the specific anatomy, you might even note a difference in the pressures between both arms.
Classic EKG and chest X-ray findings associated with coarctation of the aorta include left ventricular hypertrophy and rib notching, respectively.
Now onto this week’s podcast
Question 1
Which of the following is typically seen in Korsakoff syndrome?
A 24-year-old woman at full term presents with rupture of membranes and contractions. Sterile exam reveals a crowning infant with a visible cord. After elevating the fetal head, what management is indicated?
You suspect a 35-year-old man has epiglottitis with impending airway compromise. Which of the following is the best method for confirming the diagnosis?
A 21-year-old man presents with a stab wound to the right chest. His vitals are HR 157/min, BP 81/43 mm Hg, RR 28/min, and oxygen saturation 91%. The patient is intubated, and packed red blood cells are started. Physical examination reveals a bleeding wound to the right chest, a midline trachea, and decreased breath sounds on auscultation of the right hemithorax. Which of the following should be performed next?
A 65-year-old man with a history of hypertension presents with left-sided weakness beginning two hours prior to arrival. Vitals are BP 155/85 mm Hg, HR 102/min, RR 12/min, oxygen saturation 100% on RA. His CT scan is shown above. Which of the following therapies is appropriate?
A. Antihypertensives to lower mean arterial pressure by 25%
Korsakoff syndrome is a chronic neurologic disease caused by thiamine deficiency that typically presents with impairment of recent memory formation. Patients may also exhibit apathy and confabulation.
Wernicke’s encephalopathy often presents with ophthalmoplegia, nystagmus, ataxia, and mental status changes. Wernicke’s encephalopathy and Korsakoff syndrome or often seen simultaneously.
Treat both Wenicke and Korsakoff syndromes with thiamine and magnesium.
The most common physical exam finding in AAA is a pulsatile mass. At a diameter of 5 cm, the risk of rupture increases markedly. Diagnosis is made by ultrasound or CT scan.
For umbilical cord prolapse during delivery, plan for an emergent C-section. If C-section is not possible, attempt manual replacement of the cord into the uterus, followed by rapid vaginal delivery.
Epiglottitis classically presents with rapid onset of fever and dysphagia, often with drooling, anxiety, stridor, and a muffled voice.
The best method for confirming the diagnosis of epiglottitis is via indirect laryngoscopy, which can be done with a nasopharyngoscope. However, be careful as manipulation can lead to laryngospasm and airway obstruction. Make sure a surgical airway kit is available at the bedside.
The classic finding on lateral neck X-ray in those with epiglottitis is a thumbprint sign.
An ED thoracotomy would be indicated in a patient who loses vitals in route to the hospital or in the ED.
For intracranial hemorrages, treatment is first supportive with airway protection and maintenance of adequate perfusion. Elevate the head of the bed to 30 degrees and maintain normothermia, normocarbia, and euglycemia. Current data do not support the use of antiepileptics.
That wraps up RoshCast Episode 42! Be sure to also check out RoshCast blog for questions from this episode and prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources there to help prepare you for the boards and the wards. Don’t forget to follow us on twitter @RoshCast and @RoshReview. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Good luck on the in-training exam next week! Jeff and Nachi
Ep 41 Roshcast Emergency Board Review
Feb 05, 2018
We are what we repeatedly do. Excellence, then, is not an act, but a habit.
–Aristotle
Welcome back to RoshCast for Episode 41! As we get closer and closer to the in-training, now would be a great time to go back and listen to old episodes to brush up on some of the core EM knowledge that you may not come across regularly on shift. Let’s get started with a rapid review and our regular mixed content of questions, answers, and high-yield review.
Staph aureus is the most common bacterial cause of septic arthritis in adults.
In a patient with splenic dysfunction, the strep species are more likely to cause septic arthritis.
Septic arthritis classically presents with fever, monoarticular joint pain, and a decreased range of motion.
Joint aspirates with a white count > 50,000 with more than 75% PMNs are indicative of septic arthritis.
Now onto this week’s podcast
Question 1
Which of the following hematological disorders is characterized by intermittent venous and arterial thrombosis, splenomegaly, and abnormal proliferation of all three myeloid cell lines?
A 29-year-old man is brought to the ED for a gunshot wound to the right chest. He is diagnosed with a right-sided hemopneumothorax. A tube thoracostomy is subsequently performed with immediate drainage of 250 cc of blood. The nurse connects the chest tube to a commercial suction device, and a chest radiograph is performed that confirms proper placement. You note an absence of respiratory fluctuation of the fluid level in the drainage tube. A repeat chest X-ray shows the right-sided hemothorax remains. Which of the following is true regarding this finding?
A. An air leak is present
B. The lung is still collapsed
C. There is a blockage of the drainage tube
D. This is an expected finding
Question 5
Which of the following is true regarding Ranson’s criteria?
A. A score of 0–3 on admission constitutes a high-risk population
B. Glucose > 200 mg/dL on admission is associated with a higher mortality rate
C. Hematocrit < 35% at 48 hours is predictive of mortality
D. WBC < 10,000 is associated with a higher mortality rate
The Emergency Medical Treatment and Active Labor Law of 1986, or EMTALA, requires hospitals to provide which of the following?
A. Care to all patients
B. Interpreters for all patients in a timely manner
C. Screening exam, competent ED physicians and appropriate stabilization
D. Screening exam, stabilization process, appropriate transfer process
Question 7
A 58-year-old man with a history of cirrhosis presents with abdominal pain and fever. His abdomen is tender to palpation with guarding. You are concerned about spontaneous bacterial peritonitis. You perform a paracentesis and send the ascitic fluid for analysis. Which of the following is most consistent with a diagnosis of spontaneous bacterial peritonitis?
A. Low ascitic fluid glucose concentration
B. Polymorphonuclear neutrophil count < 250 cells/mm3
Polycythemia vera is a chronic myeloproliferative disorder marked by increased red blood cell production but can involve all three cell lines.
Polycythemia vera presents with pruritus, especially after bathing, headaches, bleeding, engorged retinal veins, splenomegaly, and gout. Treatment is with serial phlebotomy or with myelosuppressive agents.
Gilbert’s syndrome is associated with an elevated indirect bilirubin.
Alcoholic hepatitis is associated with an AST to ALT ratio of roughly 2:1.
In ischemic hepatitis, you would expect elevated transaminases over 10,000.
Hypomagnesemia can result in refractory hypokalemia not correctable by the administration of potassium.
Hypomagnesemia can lead to a prolonged QT, a widened QRS as well as atrial and ventricular dysrhythmias.
With respect to chest tubes, an air leak occurs when there is persistent air inside the pleural space.
An absence of respiratory fluctuation or a decrease in drainage of a chest tube implies that the system is blocked or the lung is fully expanded.
Ranson’s criteria is a scoring system designed to predict mortality from acute pancreatitis.
EMTALA, enacted in 1986, is a section of the Consolidated Omnibus Labor Act. It governs how physicians triage, register, examine, workup, treat and/or stabilize, discharge or transfer, utilize resources, and involve medical staff expertise when caring for patients who present to the ED.
Spontaneous bacterial peritonitis is diagnosed with an elevated ascitic fluid PMN cell count over 250 and a positive ascitic fluid bacterial culture, all in the absence of a secondary cause of peritonitis like a bowel perforation. SBP is also associated low ascitic glucose concentrations. It’s treated with a third-generation cephalosporin.
That wraps up RoshCast Episode 41! Don’t forget to follow us on twitter @RoshCast and @RoshReview. We can also be reached by email at RoshCast@RoshReview.com and are open to any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 40 Roshcast Emergency Board Review
Jan 19, 2018
Dreams and dedication are a powerful combination.
-William Longgood
Welcome back to Roshcast for Episode 40! After a quick detour last week to talk with Dr. Rosh, we are back at it with our regular routine. But before we get going, if you have any thoughts or feedback on last week’s episode, or even if you have any unanswered questions, make sure you send them our way to RoshCast@RoshReview.com, so that we can get them answered either individually by email or on another special episode.
This week, we are going to cover a few pediatric respiratory questions to parallel the EM Clerkship podcast’s most recent episode in addition to some bread and butter emergency medicine. Before we begin, let’s get warmed up with a rapid review covering environmental emergencies, since these are things we see less frequently in our day to do practice but ALWAYS appear on the in-training exam.
Pit viper bites cause local swelling and oozing from the wound. Severe envenomations can lead to a DIC like coagulopathy and hemorrhagic bullae.
Brown recluse spider bites cause a papule that later blisters and may necrose. Systemic symptoms include renal failure, pulmonary edema, and shock.
Black widow spider bites cause a local papule with a halo. Severe systemic symptoms include a peritonitic abdomen, muscle fasciculations, and diaphoresis. Remember that you can identify a black widow spider by the red hourglass on their abdomen.
Frostbite should be treated with immersion in a warm water bath set at 37-39 degrees Celsius.
Now onto this week’s podcast
Question 1
Let’s get right into with a pediatric respiratory question: A 3-year-old girl presents to the ED with 1 hour of a barking cough and inspiratory stridor at rest. On exam, she has mild retractions but is not hypoxic. Which of the following interventions has been shown to reduce hospital length of stay in moderate to severe croup?
A 33-year-old woman presents with intermittent, intense shooting pain to the left side of the face. She states that the pain begins near her ear and radiates to her chin. The pain is often brought on by chewing and brushing her teeth. Which of the following managements is most likely indicated?
You are working in a busy pediatric ED in December. During your shift, you evaluate and treat four children with moderate croup by administering oral dexamethasone and aerosolized epinephrine. You re-evaluate each child two hours after the initial racemic epinephrine treatment. Which of the following children can most safely be discharged home?
A. A 1-year-old boy with persistent stridor at rest
B. A 2-year-old uninsured boy with clinical improvement, but no primary care physician
C. A 3-month-old girl with a history of tracheomalacia who has clinical improvement
D. A 4-year-old girl with retractions that have since resolved
A 10-year-old boy presents with increased lethargy and vomiting. Mom states the patient has had three days of cough, rhinorrhea, sore throat, and fever. The nanny has been giving the patient an appropriate dose of over-the-counter cold medicine. The physical exam is remarkable for lethargy, mild icterus, and hepatomegaly. Laboratory results are remarkable for markedly elevated AST and ALT. Which medication is most likely responsible for this patient’s presentation?
A 52-year-old man with a history of renal failure status post-transplant presents with shortness of breath. He has had a non-productive cough with fevers for the last 3 days. His only medication is mycophenolate mofetil. With ambulation, he desaturates to 85% on room air and his resting saturation is 90%. Physical examination is notable for diffuse bilateral crackles. His chest X-ray is shown above. Which of the following is the most appropriate drug to administer next?
A 6-month-old girl born at 35 weeks gestation and previously well presents to the ED with wheezing and increased work of breathing. Mom reports that her daughter has had a low-grade fever, rhinorrhea, and cough for the past 3 days. In the ED, the patient’s vital signs are T 38.3ºC, HR 150/min, RR 72/min, and a pulse oximetry of 90% on room air. On exam, she is wheezing, using accessory muscles, and having subcostal retractions. An albuterol nebulizer treatment was given but no improvement was seen. Which of the following is the most appropriate next step in management?
A. Administer 1 mg/kg of oral dexamethasone
B. Administer another albuterol nebulizer treatment because the patient continues to be wheezing
C. Administer high-dose inhaled corticosteroids
D. Admit to the hospital and provide supportive care
Dexamethasone is the first-line treatment for croup. It reduces hospital length of stay in moderate to severe case of croup.
The Westley Croup Severity Score incorporates level of consciousness, cyanosis, stridor, air entry, and retractions to help guide management, which ranges from supportive care, to nebulized epinephrine, to ICU admission and intubation.
In children with croup, chest X-ray may show the classic steeple sign.
Trigeminal neuralgia presents with paroxysms of lancinating pain, typically in the V2 and V3 dermatomes. Treatment is with carbamazepine.
Bilateral facet dislocations, flexion teardrop fractures, Jefferson fractures, and type 2 and type 3 odontoid fractures are all unstable cervical spine fractures.
A flexion teardrop fracture is a fracture of the anterior inferior portion of the vertebral body, which disrupts the anterior and posterior ligamentous structures.
A Jefferson fracture is a burst fracture.
A type 1 odontoid fracture is an avulsion of the tip of the odontoid. A type 2 odontoid fracture, which is the most common, is a fracture at the base of the dens. A type 3 odontoid fracture is a fracture at the junction of the odontoid and the body of C2.
Reye syndrome presents with a rapidly progressive, non-inflammatory encephalopathy associated with altered mental status, cerebral edema, and hepatic dysfunction. Patients typically present with respiratory or a GI prodrome followed by an encephalopathic picture.
Reye syndrome is caused by salicylate usage in the setting of a viral illness. Influenza and chickenpox are commonly implicated viruses.
PJP pneumonia presents with bilateral perihilar infiltrates in a classic batwing appearance. Immunocompromised patients are at risk.
PJP pneumonia is ideally treated with trimethoprim-sulfamethoxazole. In sulfa allergic patients, consider primaquine-clindamycin or atovaquone for mild to moderate disease or pentamidine for severe disease.
Bronchiolitis should be treated with supportive care. In first-time wheezers, evidence suggests that there is no role for oral steroids or beta-agonists.
That wraps up RoshCast Episode 40! Be sure to also check out the blog for questions from this episode and prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources there to help prepare you for the boards and the wards. Don’t forget to follow us on Twitter @RoshCast and @RoshReview. You can always email us at RoshCast@RoshReview.com with any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast. We’ll be back soon with more high quality review.
Ep 39 Roshcast Emergency Board Review
Jan 04, 2018
“The person who creates structure the soonest, is the person who is most comfortable in residency the soonest.”
-Adam Rosh, MD
Welcome back to RoshCast episode number 39!
As we mentioned at the end of episode 38, this won’t be a regular old RoshCast. Instead of our regularly scheduled content, we put together an interview with Dr. Adam Rosh – the namesake of the Rosh Review, former program director, and most importantly an emergency physician who has dedicated the last 20 years of his life to education.
While this episode will not contain our usual board review content, it will include tactical advice on preparing for and taking your board exam.
This episode provides a gold mine of actionable information, tools, strategies, and tactics that you can use not only for your upcoming Shelf exam, In-Training exam, or ABEM Certification exam, but any high stakes endeavor.
Some of the topics Dr. Rosh talked about include:
The biggest studying challenges going from medical school to residency
The best advice Dr. Rosh received when he was an intern
A system to 10X your medical knowledge during residency
How to implement a study strategy called “layering” to build deep medical knowledge
How a “notebook system” made all the difference in the world to building confidence as a resident
An opportunity to aggregate Post-it Pearls
A system to capture mistakes to improve clinical practice
How studying material like the leads of an ECG looking at the heart can lead to improved understanding
Using interleaving to improve preparation for the actual exam
What do you do if you answered all of the questions in the Qbank?
How forgetting leads to improved recall
Avoiding the illusion of knowing
Choosing the right study material
Making sure you prevent people from stealing your time
The importance of exercise or simply taking a break to go for a walk to improve recall
That’s wraps up RoshCast Episode 39. Don’t forget to follow us on Twitter @RoshCast and @RoshReview. We can also be reached by email at RoshCast@RoshReview.com and are open to any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. To do so, write “RoshCast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
And let us know if you’d like us to do a Part 2 with Dr. Rosh.
Ep 38 Roshcast Emergency Board Review
Dec 20, 2017
Believe you can and you’re halfway there.
-Theodore Roosevelt
Welcome back to Roshcast episode 38, the last episode of 2018! Before we jump into this week’s episode, we have a few people to recognize. First, congrats to Zain who won the trauma ring tone challenge last episode and will be receiving a Rosh Review subscription. Special mention goes out as well to Clark, David, and Ryker who all responded soon after Zain. We should also recognize Sarah, who won the EM Clerkship-RoshCast crossover challenge and won a free copy of Case Files Emergency Medicine. Stay tuned for more contests to come! Let’s head back to the Rosh Blog and start out with a recent Rapid Review.
Central cord usually presents with sensory and motor deficits, with the upper extremities being affected more than the lower extremities. It’s most commonly caused by an extension injury.
Anterior cord syndrome presents with complete loss of motor, pain, and temperature below the level of the injury, but you would retain proprioception and vibration sensation. Anterior cord is most often caused by a flexion or vascular injury.
Brown Sequard classically occurs after penetrating trauma. It results in ipsilateral loss of motor, vibration, and proprioception with contralateral loss of pain and temperature.
Now onto this week’s podcast
Question 1
A 3-day-old girl presents with decreased feeding and is found to be limp and minimally responsive. After intubation, at what rate should breaths be delivered?
A previously healthy 5-year-old girl presents to the ED with left lower extremity pain and an inability to bear weight for 1 day. Mom denies any recent trauma. On exam, the patient has a T 37.9°C, HR 130/min, and RR 28/min. Her left lower extremity is slightly flexed and externally rotated. Lab evaluation reveals a WBC of 8,000, a C-reactive protein of 1 mg/dL, and an erythrocyte sedimentation rate (ESR) of 7 mm/hr. Radiographs are negative for fracture. The patient’s range of motion has improved following administration of ibuprofen. What is the most appropriate course of action in this patient?
A. Intravenous antibiotics and admission to the hospital
B. MRI to rule out osteomyelitis or septic arthritis
C. Orthopedic consultation for arthrocentesis
D. Treatment with NSAIDs and discharge with follow-up arranged for the following day
For infants, from birth to 1 year old, who require mechanical ventilation, set the rate at 30–60 breaths per minute. For toddlers, ages 1–3 years old, set the rate at 24–40 breaths per minute. For preschoolers, ages 3–6 years old, set the rate at 22–34 breaths per minute. For children 6–12 years old, set the rate at 18–30 breaths per minute.And lastly, for those 12 and older set the rate at 12–16 breaths per minute.
To estimate pediatric systolic blood pressure, use the formula 70 plus 2 times the age in years.
In the setting of malnutrition, folic acid deficiency and vitamin B12 deficiency can both lead to a megaloblastic anemia.
NSAIDs are first-line treatment for musculoskeletal lower back pain.
A supraorbital nerve block anesthetizes the ipsilateral forehead and scalp.
An infraorbital nerve block anesthetizes the area between the lower eyelid and the upper lip.
A posterior superior alveolar nerve block anesthetizes the second and third maxillary molars, as well as part of the first maxillary molar.
An inferior alveolar nerve block anesthetizes the ipsilateral mandibular teeth, lower lip, and chin.
An apical nerve block anesthetizes a single tooth.
The mental nerve block anesthetizes the chin as well as the skin and mucous membranes of the lower lip. Remember that the mental nerve is a branch of the inferior alveolar nerve.
Transient synovitis is the most common cause of acute hip pain in children ages three to ten years old. Treatment for transient synovitis is NSAIDs and rest.
Ductal dependent cardiac lesions include coarctation of the aorta, transposition of the great vessels, tetralogy of Fallot, tricuspid atresia, interrupted aortic arch, and hypoplastic left heart syndrome.
To temporarily preserve patency of the ductus arteriosus, treat with prostaglandin E1, or alprostadil, at a dose of 0.05–0.1 mcg/kg/min.
That wraps up RoshCast Episode 38. Don’t forget to follow us on Twitter @RoshCast and @RoshReview. We can also be reached by email at RoshCast@RoshReview.com and are open to any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. To do so, write “RoshCast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Ep 37 Roshcast Emergency Board Review
Dec 08, 2017
The most difficult thing is the decision to act, the rest is merely tenacity. The fears are paper tigers. You can do anything you decide to do. You can act to change and control your life; and the procedure, the process is its own reward.
-Amelia Earhart
Welcome back to Roshcast Episode 37! This week, we’re continuing our collaboration with the EM Clerkship podcast. We’ll cover 3 EKG related questions in addition to 3 randomly generated questions. Maybe we’ll even get to a trauma question…
As a reminder, listen closely for the trauma ring tone during this episode and the next episode. And e-mail us at roshcast@roshreview.com or tweet us at Roshcast the exact time of the ring tone to win a subscription. With the in-training exam right around the corner, this will certainly help get you ready for February 28th. Let’s get going with a rapid review from a recent post on the Rosh Review Blog.
Supracondylarfracture is the most common type of pediatric elbow fracture. Typically caused by falling on an outstretched hand — or a FOOSH.
In a posterolaterally displaced supracondylar humeral fracture,you should be concerned for the median nerve. This can be tested by asking the patient to make an “OK” sign and checking sensation at the volar tip of the index finger
For a posteromedially displaced supracondylar fracture you should be concerned about the radial nerve. Have the patient try to make a “thumbs up” sign. And check sensation along the dorsal web space of the hand.
Now onto this week’s podcast
Question 1
A previously healthy patient who presents with leg pain is found to have a clot within the tibial vein. Which of the following treatments is most likely indicated?
A. Aspirin for 6 months
B. Heparin and warfarin
C. Repeat ultrasound in 2–5 days
D. Warfarin alone
Question 2
Which of the following is associated with a shortened PR interval?
A 29-year-old man presents after a syncopal episode. His ECG reveals an epsilon wave, a small positive deflection buried in the end of the QRS complex. Which of the following tests will likely identify the cause of the patient’s syncope?
A 12-year-old boy is brought to the ED after being struck in the chest by a baseball during a baseball game. He collapsed immediately upon impact and has been unresponsive since. Which of the following dysrhythmias is most commonly associated with this condition?
A 57-year-old man with hypertension presents complaining of a 6-hour history of a “floater” in the right eye. He states that he has had increasing difficulty reading as the cloudy area blocks his visual field. Additionally, he complains of decreased vision in his right eye. Which of the following represents the appropriate management?
A. Administer timolol drops and emergently consult ophthalmology
B. Emergent ophthalmology consultation
C. Prescribe topical antibiotics and refer to ophthalmology
D. Refer patient to ophthalmology for further assessment Teaching Image
Question 6
A 27-year-old woman and her 25-year-old sister present with symptoms of facial flushing, headache, abdominal cramping, and diarrhea after eating in a seafood restaurant. They report that the fish they ate had a peppery taste. Which of the following is the most likely cause of their symptoms?
Isolated thromboses of the calf veins can be managed by repeating an ultrasound in 2–5 days to determine the need for anticoagulation.
Phlegmasia cerulean dolens is caused by extensive iliofemoral occlusion, which leads to vascular congestion and venous ischemia and a painful blue leg.
Phlegmasia alba dolens is caused by a massive iliofemoral thrombosis and spasm and leads to a white leg.
WPW is a congenital abnormality characterized by an abnormal accessory conduction pathway between the atria and the ventricle known as the bundle of kent. Look out for a delta wave, short PR, and widened QRS interval on EKG. The definitive treatment is ablation.
Brugada syndrome is a hereditary condition characterized by a right bundle branch block-like pattern with ST elevation in leads V1 through V3.
Wellens syndrome is caused by critical stenosis of the proximal LAD. On EKG you will likely see large inverted T waves or biphasic T waves in leads V2 and V3.
Epsilon waves, which are small positive deflections buried in the terminal QRS complex, are characteristic of arrhythmogenic right ventricular cardiomyopathy. It is diagnosed by cardiac MRI.
Arrhythmogenic right ventricular cardiomyopathy is treated with antiarrhythmics and an implantable cardiac defibrillator.
Commotio cordis occurs when an object strikes the chest over the heart. It can cause sudden death. Commotio cordis is most common in children 5–15 years old, and ventricular fibrillation is the most common underlying rhythm.
The commotio cordis risk window is the upstroke of the T wave in the cardiac conduction cycle.
Posterior vitreous detachment can cause floaters, decreased vision, and cloudiness. Acute changes warrant emergent ophthalmology consultation.
Scombroid poisoning presents with facial flushing, headache, abdominal cramping and diarrhea, palpitations, and rashes.Onset of symptoms can be anywhere from 10 minutes to 24 hours. Treatment is supportive with H1 and H2 blockers.
Ciguatera toxicity is associated with muscle weakness, paresthesias, vomiting, diarrhea, and reversal of hot-cold sensation.
That wraps up Roshcast Episode 37. Before we officially sign off for this week, we wanted to solicit your help for an upcoming episode. Very soon, we are bringing Adam Rosh, who is the founder of Rosh Review, onto the podcast to discuss everything from study tactics to his favorite pre-test meal. We have a couple of our own questions lined up, but we want to know what questions you have. Send us any questions for Adam to jeff@roshreview.com and we’ll try to squeeze them all in. That’s it for this week. Don’t forget to follow us on Twitter @Roshcast and @RoshReview. And you can always email us at roshcast@roshreview.com with any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast. We’ll be back soon with more high-quality review.
Ep 36 Roshcast Emergency Board Review
Nov 22, 2017
Do not go where the pay may lead, go instead where there is no path and leave a trail.
-Ralph Waldo Emerson
Welcome back to Roshcast Episode 36! This week we continue our collaboration with the EM Clerkship podcast, focusing on pediatrics. Don’t forget that we launched another trauma ring tone contest week, so listen up through Episode 38 to win a subscription to Rosh Review. For this week’s rapid review, we will be covering a few pearls from Yehuda’s most recentposts on the Rosh Review Blog. Let’s get started!
Cysticercosis is caused by Taenia solium, a common tapeworm. It’s transmitted via pork. Patients may present with seizures and CNS cysts.
Patients with acute angle-closure glaucoma classically present with severe eye pain, blurry vision, photophobia, and a dilated pupil. The intraocular pressure in this case would be elevated.
Iritis presents with peri-limbic injection, a constricted pupil, pain, photophobia, and blurry vision. You would expect the intraocular pressure to be normal or even low.
Now onto this week’s podcast
Question 1
A 4-week-old boy presents with a 2-week history of increasing dyspnea, cough, and poor feeding. On examination you note conjunctivitis, and a chest examination reveals tachypnea and rales. A chest X-ray shows hyperinflation and diffuse interstitial infiltrates. Which of the following is the most likely etiologic agent?
A 6-year-old immigrant boy from Bangladesh presents with fever and rash. The fever started three days ago followed by a rash which started on the head and spread to the rest of the body. Examination reveals a well-appearing child with a maculopapular rash and posterior cervical lymphadenopathy. Which of the following is the most likely causative organism for this disease?
A healthy 6-year-old boy presents to the ED with bloody diarrhea. He was in his usual state of health until one week ago when loose, watery stools (up to 10 per day) were noted. He was seen by his pediatrician four days ago but has since developed increasing amounts of blood and pus in his stools along with a low-grade fever. Mom states there is no recent travel, antibiotic use, or known sick contacts. His vitals are heart rate 118 beats per minute, oxygen saturation 100% on room air, and rectal temperature of 38.3°C. Your physical exam reveals a mildly tender abdomen without localization, rebound, guarding, or peritoneal signs. You note grossly bloody stool on rectal exam. A brief discussion with his pediatrician confirms your suspicion of an invasive bacterial diarrhea; a stool culture was positive for Shigella. Which of the following statements is true regarding this condition?
A.Antibiotics should be avoided because this is a severe case and the patient is at highest risk of developing hemolytic uremic syndrome
B. Antidiarrheal agents (such as diphenoxylate and atropine) are indicated, given the frequency of loose stools
C. Extraintestinal manifestations such as hallucinations, confusion, and seizures may occur
D. Oral rehydration should be avoided; IV fluids should be initiated
Chlaymdial pneumonia is often found in infants 3–16 weeks old. They usually present, non-toxic appearing and afebrile, but with tachypnea and a staccato cough, with or without rales. 50% also have conjunctivitis. Treat with azithromycin.
Infants with parainfluenza virus typically present with coryza, a low-grade fever followed by a classic barking cough of croup.
Infants with RSV present with lower respiratory tract infections like bronchiolitis.
Measles presents with a fever followed by a rash and Koplik spots.
Mumps is associated with an infectious parotitis.
Infants with parvovirus B19 often present with erythema infectiosum with the classic slapped cheek appearance.
Rubella, also called German measles, often presents with a mild febrile illness with a diffuse maculopapular rash, generalized malaise, along with lymphadenopathy.
When choosing an endotracheal tube for children use the following formulas. For uncuffed tubes, take the age, divide it by 4, and add 4. For cuffed tubes, take the age, divide it by 4, and add 3.5.
Retinal hemorrhages are the most common manifestation of abusive head trauma in infants.
Posterior rib fractureswithout overlying bruises, metaphyseal fractures, sternal fractures, scapular fractures, and skull fractures should raise your suspicion for non-accidental trauma.
For hypoglycemic childrenless than one year of age, use D10 5–10 ml/kg. For hypoglycemic children who are 1 to 8 years old, use D25 2–4 ml/kg. For hypoglycemic children over the age of 8, use D50 1–2 ml/kg.
Extraintestinal manifestations of Shigella include confusion, hallucinations, and seizures.
For children concerning for shigellosis, treat supportively with PO fluids if tolerated. Antidiarrheal agents should be avoided. Depending on the situation, antibiotics may be needed.
That wraps up Episode 36. Don’t forget to follow us on Twitter @Roshcast and @RoshReview. We can also be reached by email at roshcast@roshreview.com and are open to any feedback, corrections, or suggestions. You can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 35 Roshcast Emergency Board Review
Nov 09, 2017
Reach for it. Push yourself as far as you can.
-Christa McAuliffe
Welcome back to Roshcast Episode 35! It was great chatting with a bunch of listeners at ACEP last week. We received a lot of excellent feedback.
This week, we’ll be doing a couple of diarrhea questions to link up with the last EM Clerkship episode, in addition to a few randomly generated questions. Don’t forget that we are still running a trauma ring tone contest. Listen closely for a ring tone in an upcoming episode and e-mail us at roshcast@roshreview.com or tweet to us at @Roshcast the exact time of the ring tone to win a prize, which will certainly come in handy as we get closer to the in-training exam. Let’s get started with a review from recentposts on the Rosh Review Blog.
Pterygium is a fleshytriangular growth from the medial canthustowards thecornea. They are usually slow growing and seen in those with excessive sunlightexposure. They are managed with artificial tears.
Pterygium typically doesn’t require surgery but may need excision if it is causing a visual disturbance. Make sure the patient is already following with an ophthalmologist or give them a referral if needed.
Retinal detachments present with painless loss of vision, floaters, flashing lights, or as a curtain lowering sensation. On physical, you may see a hazy grayretina with whitish folds.
The most common location for an ectopic pregnancy is the fallopian tube.
Now onto this week’s podcast
Question 1
A 2-year-old girl presents after a witnessed seizure. The parents state that she has not been to daycare in two days, as she has bloody diarrhea and a fever. Her vitals on presentation are T 103.1°F, HR 167/min, BP 73/43 mm Hg, RR 48/min, and oxygen saturation 96%. Currently, the patient has a normal neurologic exam and minimal abdominal tenderness. There are no rashes. Labs show a WBC of 19,000, and urinalysis reveals an elevated specific gravity. Which of the following is the most appropriate next step in management?
A. Acetaminophen for fever and follow-up with primary care provider
B. Blood and stool cultures, IV antibiotics, and admission
C. Neurology consultation and admission
D. Oral antibiotics and follow-up with primary care provider
An 82-year-old nursing-home resident is sent to the emergency department with lower abdominal pain and bloody diarrhea. He has a history of vascular dementia, hypertension, and hyperlipidemia. On examination he is afebrile, and a nasogastric aspirate is negative for evidence of bleeding. Which of the following is the most likely cause of this patient’s bleeding?
A 35-year-old-man with a history of occasional bloody diarrhea and abdominal pain presents with acute onset severe abdominal pain. Vital signs are significant for a temperature of 39°C, heart rate 140/min, and blood pressure 82/55 mm Hg. On physical exam, his abdomen is distended and tympanic. Which of the following diagnostic studies is indicated first at this time?
A 45-year-old woman complains of two days of fluctuating diplopia and dysphagia. Her exam reveals a left cranial nerve VI palsy, ptosis, and proximal muscle weakness in her extremities. What is the pathophysiology of her disease?
A. Antibodies to the acetylcholine receptor at the neuromuscular junction
B. Inhibition of acetylcholine release at the synapse
C. Mutation of superoxide dismutase causing cell death
D. Reduced number of dopamine receptors in the midbrain
Patients with Shigella often present with fever, abdominal cramps, and diarrhea with mucus or blood. Infants with Shigella are also at risk for seizures.
Shigellosis should be treated supportively. Patients who are immunocompromised, have bacteremia, attend daycare, or live in a nursing home require treatment with antibiotics. Children should be treated with ceftriaxone, 50 mg/kg in a once-daily dose up to a max of 1.5g for 5 days.
Ischemic colitis is caused by inadequate blood flow through the mesenteric vessels. It often affects the watershed regions.
Ischemic colitis can be treated supportively with bowel rest and IV fluids unless there are signs of peritonitis or infarction.
Risk factors for suicide include male sex, age, history of mental illness, personal or family history of a suicide attempt, poor financial situation, unemployment, poor physical health, being Caucasian, and isolation.
With respect to suicide, marriage, and first-trimester pregnancy are both protective.
Swallowed foreign bodies that do not pass through the esophagus, which occurs 2% of the time, have a risk for esophageal perforation or erosion.
Emergent endoscopy is indicated if the swallowed foreign body is a battery, is sharp, or if there are signs of obstruction.
Coins in the sagittal plane on X-ray are more likely to be in the trachea than in the esophagus.
Toxic megacolon presents with colonic dilatation and systemic toxicity. Patients usually present after having symptoms of colitis for several days.
If there is concern for toxic megacolon, an abdominal X-ray should be the first imaging study to look for colonic dilatation, to a diameter greater than 6 cm.
Toxic megacolon can be precipitated by IBD, pseudomembranous colitis, CMV colitis, and bacterial colitis.
Myasthenia gravis is caused by antibodies to the acetylcholine receptor at the neuromuscular junction.
Ptosis and diplopia are the most common first symptoms of a myasthenic crisis. This is followed by proximal muscle weakness, dysphagia, and dyspnea. Respiratory failure can be seen in the later stages.
Myasthenia gravis can be diagnosed by the edrophonium or Tensilon test.
Myasthenia gravis can be treated with plasma exchange and IVIG. Icedecreases symptoms but is not a permanent solution.
That wraps up Episode 35. Don’t forget to follow us on Twitter @Roshcast and @RoshReview. We can also be reached by email at roshcast@roshreview.com and are open to any feedback, corrections, or suggestions. You can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 34 Roshcast Emergency Board Review
Oct 25, 2017
Keep your eyes on the stars and your feet on the ground.
-Theodore Roosevelt
Welcome back to Roshcast Episode 34! This week we continue our collaboration with the EM Clerkship podcast, focusing on appendicitis. Don’t forget that we launched another trauma ring tone contest last week, so listen up through episode 38 to win the prize. For this week’s rapid review, we reviewed dysbarism in honor of the Rosh Review Core Content Winner’s presentation. If you haven’t seen Dr. Sanders and Dr. Levin’s fantastic presentation, it’s definitely worth checking out. Let’s get started!
A diver with an arterial gas embolism would classically presents within 10 minutes with neurologic symptoms that resolve and then recur.
Typical symptoms of an arterial gas embolism include unconsciousness, respiratory or cardiac arrest, coma, stupor, confusion, unilateral neurologic changes, visual disturbances, dizziness, or convulsions.
Decompression sickness presents in a variety of ways. 68% of patients will present with joint pains, 63% will present with numb patches and paresthesias, and 41% will have constitutional symptoms and fatigue. Other less common symptoms include dizziness, weakness, itching, hearing loss, and tinnitus.
On scene, a diver with either an arterial gas embolismordecompression sickness should be treated with the standard IV fluids, supplemental oxygen, and then be placed on a monitor. Definitive treatment is with hyperbaric oxygen.
Now onto this week’s podcast
Question 1
Which of the following is the average duration of a typical generalized tonic-clonic seizure?
A. 1–2 minutes
B. 10–15 seconds
C. 30–40 seconds
D. 4–5 minutes
Question 2
A 23-year-old man presents with abdominal pain, vomiting and two loose, nonbloody stools. Physical examination reveals right lower quadrant tenderness to palpation. A CT is performed showing a normal appendix and some inflammation at the ileocecal junction. What pathogen is commonly implicated in this disorder?
A 9-month-old girl presents to the ED with signs of progressive dyspnea. The patient’s mother reports URI symptoms that have been present for two weeks. Over the previous 24 hours, the patient has been increasingly fussy, noted to be sweaty with feeds, and has become increasingly dyspneic. Her vital signs are T 38.3°C, HR 180, RR 38, POx 93%, and BP 60/40. On examination, you note rales at the lung bases. Her heart rhythm is irregular with an S3 gallop, and the liver is palpable 3 cm below the costal margin. Which of the following is the most appropriate therapeutic intervention?
The average duration of a generalized tonic-clonic seizure is 1–2 minutes.
Status epilepticus is defined as any seizure lasting greater than 5 minutes or 2 discrete seizures without a recovery to consciousness.
For the treatment of status epilepticus, benzodiazepines are the first-line agents. Second-line agents include phenytoin, fosphenytoin, valproic acid, phenobarbital, and levetiracetam. Pentobarbital and propofol are third-line agents.
Yersinia enterocolitica can cause ileocecitis which can mimic appendicitis. Other symptoms include colicky abdominal pain, fever, nausea, vomiting, and diarrhea. Treatment is supportive.
Pediatric heart failure is treated with dobutamine if hypotensive or with milrinone if normotensive or hypertensive.
Common causes for myocarditis include viruses, bacteria, parasites, cardiotoxins, systemic disorders, radiation, and hypersensitivity.
A leukocytosis is seen in up to 70% of patients with appendicitis.
Appendicoliths are rarely identified, they are only seen 10% of the time radiographically.
33% of patients diagnosed with appendicitisdo NOT report anorexia.
Phimosis is the inability to retract the foreskin over the glans.
Paraphimosis is the inability to return the retracted foreskin over the glans.
Varicocele is a collection of dilated and tortuous veins surrounding the spermatic cord. They usually cause no symptoms.
There is a high positive likelihood ratio for acute appendicitis with migration of pain from the periumbilical area to the right lower quadrant.
Obturator sign is the elicitation of pain with flexion and internal rotation of the right hip which signifies a pelvic location of the appendix.
Rosving sign is palpation of the left lower quadrant causing referred pain to the right lower quadrant.
That wraps up Episode 34. We will be at ACEP next week and hope to meet many of you there. Definitely swing by the Rosh Review booth (1442) to say hi and give us some feedback and suggestions!
Don’t forget to follow us on Twitter @Roshcast and @Roshreview. We can also be reached by email at roshcast@roshreview.com and are open to any feedback, corrections, or suggestions. You can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 33 Roshcast Emergency Board Review
Oct 11, 2017
People who are crazy enough to think they can change the world, are the ones who do.
-Rob Siltanen
Welcome back to Roshcast Episode 33! This episode marks an incredible milestone for Roshcast. Exactly 365 days ago, Roshcast was born (Apgars 7 and 9). It is wild to look back and think about how much we have covered – hundreds of questions, thousands of pearls, dozens of test-taking strategies, regular tweets, etc.
We couldn’t be more excited about where Roshcast has been or where it is going. In honor of hitting one year, we are doing another trauma ring tone competition. During episodes 34 to 38, listen for a trauma ring tone, and tweet the exact time to us or e-mail the time to us. A few weeks ago, we also launched a new partnership with the EM Clerkship podcast as a core EM corollary for selected topics. This week, we are doing another crossover episode, in which we return to cardiac arrhythmias — specifically, bradycardia. Let’s get the episode started with a rapid review of some essential vitamins, which were recently covered on the Rosh Blog.
The fat-soluble vitamins are A, D, E, and K.
Vitamin D deficiency can lead to rickets in children and osteomalacia in adults. Vitamin D deficiency is classical seen in the elderly, those with insufficient sunexposure, malnutrition, malabsorption, breastfeeding infants, and those who take anticonvulsants.
Vitamin E deficiency can present with areflexia, peripheral neuropathy, gait abnormalities, ophthalmoplegia, and decreased proprioception.
Vitamin A deficiency is associated with night blindness, xerosis (dryness of the skin, mucous membranes, and conjunctiva), as well as Bitot’s spots (white patches on the conjunctiva).
Now onto this week’s podcast
Question 1
A 66-year-old woman presents with generalized weakness and dyspnea on exertion for 2 weeks. Vital signs are BP 80/45, HR 40, RR 16, and pulse oximetry 97% on room air. Her ECG is shown above. There are no other ST-segment abnormalities. Which of the following is the most appropriate next step in management?
A. Administer aspirin, heparin and admit for acute coronary syndrome
B. Cardiac catheterization laboratory activation
C. Observation and arrange for follow up with cardiology
A 52-year-old man presents from his primary care physician’s office for evaluation of an abnormal electrocardiogram. His ECG is seen above. He has no symptoms. What is the appropriate intervention?
An infant with episodes of cyanosis and respiratory difficulty is diagnosed with Tetralogy of Fallot. Which of the following defects would you expect to see on echocardiographic examination?
A. Aorta-pulmonary artery transposition
B. Atrial septal defect
C. Left ventricular hypertrophy
D. Overriding aorta
Question 7
A 50-year-old woman presents to the ED with minor chest pain. She lifted some heavy groceries from the car yesterday. She has a history of hypertension that is controlled with metoprolol. In the ED, her vital signs are BP 120/80, HR 68, RR 14, and oxygen saturation 99% on room air. Her rhythm strip is seen above. Which of the following is the represented rhythm?
Second-degree type 1 block may be related to increased vagal tone or medications that block the AV node.
Second-degree type 2block and complete heart block require a pacemaker. If symptomatic or hemodynamically unstable, patients with such high degree AV block require immediate transcutaneous or transvenous pacing until a permanent pacer can be implanted.
Medications that block the AV node include adenosine, beta-blockers, calcium channel blockers, and digoxin.
Osborn waves, also known as late delta waves or J waves, are positive deflections of the J point that are characteristic of hypothermia and are usually only seen at temperatures below 32° Celsius.
Concurrent bullous myringitis and pneumonia is associated with Streptococcus pneumoniae. Treating the pneumonia will also treat the otalgia.
A Segond fracture is pathognomonic for ACL injury.
To test for ACL injury, perform either the Lachman or the anterior drawer test. The Lachman test is more sensitive.
Remember the PROVe mnemonic for the cardiac defects seen in Tetralogy of Fallot (ToF): Pulmonary stenosis, RV hypertrophy, Overriding aorta, and VSD.
That wraps up Episode 33, marking one full year of Roshcast. We will be at ACEP at the end of the month and hope to see many of you there. Definitely swing by the Rosh Review booth (1442) to say hi and give us some feedback or any suggestions you might have to improve the podcast! Don’t forget to follow us on Twitter @Roshcast and @Roshreview. We can also be reached by email at roshcast@roshreview.com. Remember that you can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 32 Roshcast Emergency Board Review
Sep 28, 2017
Somewhere, something incredible is waiting to be known.
-Sharon Begley
Welcome back to Roshcast Episode 32! We are returning to our regular format – letting the question back randomly generate this week’s material. We will have another collaborative episode with the EM Clerkship podcast soon. We start this episode off with another rapid review based on a recent blog post by Yehuda Wolf. Make sure you keep checking the blog for rapid reviews.
Rocky Mountain spotted fever often presents with an abrupt onset of severe headaches, photophobia, vomiting, diarrhea, and myalgias, along with a maculopapular eruption on the patients’ palms and soles.
Rocky Mountain spotted fever is transmitted by the Dermacentor tick.
Rocky Mountain spotted fever is treated with doxycycline, even in children.
Now onto this week’s podcast
Question 1
A 2-year-old boy is brought to the emergency department by his pregnant mother with complaints of hematemesis and bloody diarrhea and an episode of shaking that looked like a seizure. The patient has no past medical history; immunizations are up-to-date. His vital signs are BP 68/32 mm Hg, HR 170 beats per minute, RR 30 breaths per minute, temperature is 36.8°C, and oxygen saturation is 96% on room air. On physical exam, the child appears pale and lethargic. HEENT exam is normal with moist mucosa. His abdomen is nondistended but tender on palpation with active bowel sounds. His skin is cool and clammy. Laboratory results are as follows:
Sodium
137 mEq/L
WBC
17,000/µL
Potassium
5 mEq/L
Platelets
250/µL
Chloride
99 mEq/L
Stool guaiac
Neg
BUN
10 mg/dL
UA
Neg
Creatinine
0.5 mg/dL
UDS
Neg
CO2
16 mg/dL
Serum tox screen
Neg
Glucose
280 mg/dL
aPTT, PT w/INR
Normal
Which of the following arterial blood gases is most consistent with the patient’s diagnosis?
A 3-week-old boy presents with two days of nonbilious projectile vomiting. Examination reveals a mass in the infant’s right upper quadrant. On a barium upper GI series report, the radiologist states a “string sign” is present. Which of the following is this infant at greatest risk of developing?
A 47-year-old previously healthy man is transferred to your facility in Arizona with acute respiratory distress syndrome and cardiogenic shock. Two days ago, symptoms began with muscle aches, fever, chills, cough, nausea, vomiting, and diaphoresis. Two weeks earlier he was camping in an old, unkempt cabin in the San Rafael Valley, AZ. His two friends who stayed with him eventually began to show similar symptoms. Which of the following tests will confirm the suspected diagnosis?
A 16-year-old woman arrives to the ED via EMS after she collapsed at a Rave party. Her vital signs are 105.2°F, HR 160 RR 22, and BP 180/100. She is confused, agitated, combative, diaphoretic and has mydriasis. Her reflexes are 4/4 and clonus is noted. Her extremities demonstrate rigidity. Which of the following is the most likely diagnosis?
Iron overdose can cause an anion gap metabolic acidosis. Severe cases can lead to dehydration and shock.
Iron overdose should be treated supportively. In severe cases, IV deferoxamine can be given.
The fundal height at 12 weeks is approximately at the pubic symphysis. At 20 weeks, it is at the umbilicus. At 36 weeks, it is at the xiphoid process. And between 37 and 40 weeks, the fundal height regresses slightly.
Pyloric stenosis can cause a hypochloremic, hypokalemic metabolic alkalosis. Make sure you resuscitatebefore sending the patient to the operating room.
Pyloric stenosis presents with bilious, projectile vomiting. It typically occurs between 2 weeks and 2 months of age, and it is more common in males. Diagnosis is made with ultrasound or an upper GI series.
Hemoperitoneum can lead to relative bradycardia thought to be due to irritation of the vagus nerve.
The double decidual sign is a normal finding in early pregnancy. Later in the pregnancy, you can expect to see a gestational and yolk sac in the uterus.
B lines are indicative of pulmonary edema. A lines are a normal horizontal artifact.
Absence of lung sliding can be seen in the setting of pneumothorax, apnea, and superficial pneumonias.
Hantavirus is transmitted by feces and urine from deer mice and is found west of the Mississippi River. It can cause cardiopulmonary disease, renal disease, and hemorrhagic fevers. ECMO can be useful in severe cases.
Serotonin syndrome presents with fever, tachycardia, hypertension, agitation, and confusion. Treatment is with benzodiazepines, hydration, and aggressive cooling. MDMA or ecstasy can cause serotonin syndrome.
That wraps up Episode 32. Don’t forget to follow us on Twitter at @Roshcast and @RoshReview. We can also be reached by email at roshcast@roshreview.com. Please send over any feedback, corrections, or suggestions. You can also help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 31 Roshcast Emergency Board Review
Sep 13, 2017
The only journey is the one within.
-Rainer Maria Rilke
Welcome back to Episode 31! We are continuing our collaborative effort with the EM Clerkship podcast, focusing this week on tachydysrhythmias in addition to a mixture of random topics. We start the episode off with another rapid review of a few of the recent blogposts by Yehuda Wolf.
In a gravid female, the uterus will be palpable at the umbilicus at around 20 weeks. At 12 weeks, the fundal height will be around the pubic symphysis. Lastly, at 36 weeks the fundus will be at the xiphoid process.
Patients with polycystic ovarian syndrome are often obese and complain of hirsutism, irregular menses, acne, and sleep disordered breathing. You might also notice acanthosis nigricans and fatty liver disease.
Management for PCOS is typically done in an outpatient setting, but a common regimen could include OCPs, metformin, and lifestyle modification.
Now onto this week’s podcast
Question 1
A 58-year old man is brought to the ED for chest pain that started 30 minutes prior to arrival while he was jogging in the park. Initially, the patient’s cardiac monitor shows sinus tachycardia with a rate of 120 beats per minute. However, while you are interviewing the patient in the resuscitation bay, he suddenly becomes pale, pulseless, and the below rhythm is seen on the cardiac monitor. Which of the following is the definitive next step to manage this rhythm?
In a patient with traumatic brain injury, which of the following secondary insults should be given the highest priority for correcting in the ED?
A. Hypercarbia
B. Hyperpyrexia
C. Hypotension
D. Hypothermia
Question 4
A 45-year-old man with a history of opioid abuse presents to the ED with new onset syncope. While you are evaluating the patient, he becomes unresponsive and you note the rhythm below on the monitor. Which of the following medications is the most likely cause of this presentation?
An 84-year-old man presents from a nursing home. The patient is lethargic and unable to provide any history. The transfer record reports a new cough and chills. His vital signs are T 102°F, BP 88/42, HR 118, RR 22, and oxygen saturation 95% on room air. In addition to an intravenous normal saline bolus of 30 cc/kg, which of the following is the most appropriate empiric treatment?
In a witnessed cardiac arrest for a patient in ventricular fibrillation, immediatedefibrillation should be performed.
In an unwitnessed cardiac arrest with an unknown downtime, regardless of rhythm, chest compressions should be initiated immediately.
The defibrillating dose for a biphasic defibrillator is 200 J, whereas 360 J are required with a monophasic defibrillator. Biphasic defibrillators are preferred as they cause less cardiac damage and have higher first shock success.
In atrial fibrillation with WPW, avoid AV nodal blocking agents, like amiodarone, beta-blockers, calcium channel blockers, and digoxin.
For an unstable patient in atrial fibrillation with WPW, synchronized cardioversion should be performed.
In patients with traumatic brain injury, hypoxia and hypotension are associated with worse outcomes.
Torsades de Pointes is often caused by drugs that prolong the QT. Other risk factors for Torsades de Pointes include female gender, hypokalemia, hypomagnesemia, structural heart disease, stroke, brain injury, and bradyarrhythmias.
Torsades de Pointes should be treated with magnesium if the patient is stable. In an unstable patient, synchronized cardioversion or overdrive pacing should be performed.
There are four criteria to think of for healthcare-associated pneumonia:
Infection occurring within 90 days of a 2-day or longer hospitalization.
Resident from a nursing home or long-term care facility.
Infection within 30 days of receiving IV antibacterial therapy, chemo, or wound care.
A patient on hemodialysis.
HCAP should be treated with three drugs: one covering gram negatives including Pseudomonas, one for MRSA coverage, and lastly a third for atypical coverage.
Always draw blood cultures before giving antibiotics when treating suspected sepsis and start a 30 cc/kg bolus assuming they do not have contraindications.
Multifocal atrial tachycardia is often associated with COPD.
That wraps up Episode 31. Do not forget to follow us on Twitter @Roshcast and @Roshreview. We can also be reached by email at roshcast@roshreview.com. We are open to any feedback, corrections, or suggestions. You can also help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 30 Roshcast Emergency Board Review
Aug 31, 2017
Only I can change my life. No one can do it for me.
-Carol Burnett
Welcome back to Episode 30! First, we must congratulate Sean for winning the trauma ring tone challenge by being the first to respond after the episode release. An honorable mention goes out to Nich and Dhinakar. Stay tuned for future contests and prizes!
Today’s episode also marks the launch of a new partnership with the EM Clerkship podcast. Going forward, we are going to occasionally focus episodes on a specific topic—a topic that was recently covered by EM Clerkship. We will cover a few questions on that specific area and fill in the rest of the episode with the usual random assortment. You can listen to the podcasts in either order. Either start with Roshcast to see where you stand and then head over to EM clerkship for more detail—or alternatively, start with EM clerkship to learn the nuts and bolts, and then head back here to test yourself. Any time we do these joint releases, we will plan to match our mid-week release with their release a few days earlier on Sunday. Hopefully you enjoy our new collaboration!
Enough announcement. Let’s get going with the rapid review!
To diagnose Kawasaki disease, you must have a fever for five or more days and four of the following five criteria: bilateral bulbar conjunctival injection, oral mucous membrane changes, peripheral extremity changes, polymorphous rash, and cervical lymphadenopathy.
Kawasaki disease is treated with IVIG and aspirin.
Ocular findings associated with Wernicke’s encephalopathy include nystagmus, lateral rectus palsy, and conjugate gaze palsies.
When treating Wernicke encephalopathy, you should replace thiaminebefore repleting their glucose.
Now onto this week’s podcast.
Question 1
You are caring for a 60 kg patient who has been seizing for 30 minutes. You have already administered 4 mg of IV lorazepam and 1200 mg of phenytoin without termination of seizure activity. Which of the following should most likely be your next step?
A 33-year-old man presents with a seizure lasting for 5 minutes. EMS administered 2 mg of lorazepam with cessation of seizure activity. On presentation, the patient is confused. The patient’s medication list includes metoprolol and isoniazid. During the evaluation, he has another seizure lasting for 10 minutes and then a third seizure lasting for another 10 minutes. What adjunctive therapy should be given?
A 75-year-old nursing home patient presents with abdominal distension. Vital signs are normal and the patient is “nontoxic” appearing. An abdominal X-ray is obtained. What management is indicated?
A. Endoscopic detorsion
B. Intravenous antibiotics
C. Observation and reassessment
D. Surgical resection
Question 4
A 26-year-old woman with a history of dysmenorrhea and depression presents to the ED after having a seizure witnessed by her husband. He reports finding her on the bedroom floor with an empty pill bottle. Which of the following non-steroidal anti-inflammatory (NSAIDs) medications did she most likely ingest?
A. Celecoxib
B. Ibuprofen
C. Mefenamic acid
D. Rofecoxib
Question 5
An 8-month-old child presents to the emergency department having generalized tonic-clonic seizure activity. Her mother reports that she is bottle-fed and has been diluting her formula secondary to financial strains. Her serum sodium is found to be 120 mEq/L. She weighs 8 kgs. She is actively seizing. What is the most appropriate dose of 3% hypertonic saline to administer the patient?
A. 16 mL of 3% hypertonic saline
B. 4 mL of 3% hypertonic saline
C. 64 mL of 3% hypertonic saline
D. 80 mL of 3% hypertonic saline
Question 6
A full-term 3-week-old girl is brought in by her parents who report that she has been “acting funny” for 2 hours. They noticed that she has been moving her lips nonstop. She was a full-term, normal, spontaneous vaginal delivery and has been feeding well with adequate wet diapers since hospital discharge. She is afebrile and vital signs are normal. The anterior fontanelle is flat, and red reflexes are present. Heart, lung, and abdominal exams are normal. Her neurologic exam is positive for root, suck, and Moro reflexes, upgoing Babinski reflexes, and rhythmic lip-smacking movements. What is the most appropriate next step to take with this baby?
A. Administer phenobarbital
B. Initiate EEG monitoring
C. Perform a CT scan of the brain
D. Provide reassurance that this is normal behavior
Status epilepticus is defined as 2 or more continuous seizures without full recovery or continuous seizure activity for greater than 5 minutes.
Benzodiazepines are the first-line agents for status epilepticus. Midazolam has the fastest onset, but lorazepam has a longer half-life.
Second-line agents for status epilepticus include phenytoin, fosphenytoin, valproic acid, phenobarbital, or levetiracetam. Fosphenytoin is preferred as it can be given more quickly.
Third-line agents for status epilepticus include pentobarbital and propofol along with likelyintubation.
All seizing patients need to have their blood glucose checked.
In patients on INH having seizures, pyridoxine should be administered.
For sigmoid volvulus, the treatment of choice is endoscopic detorsion, typically a flexible sigmoidoscopy.
On a barium enema of a patient with sigmoid volvulus, the classic finding is a bird’s beak appearance.
Mefenamicacid is an NSAID given for menstrual pain. Overdose can cause seizures 2–7 hours after ingestion. Treatment is with benzodiazepines.
For seizures related to hyponatremia, 3% hypertonic saline at 2 mL/kg should be given with a max of 100 mL over 10–60 minutes.
Neonatal seizures are more likely to be focal than tonic-clonic. Look for signs like lip smacking, eye deviation, staring, rhythmic blinking, and bicycling movements.
Phenobarbital is the drug of choice for neonatal seizures.
First neonatal seizures require a full septic workup. Empiric antibiotics should be given.
That wraps up Episode 30. Don’t forget to follow us on Twitter at @Roshcast and @RoshReview. We can also be reached by email at roshcast@roshreview.com. Send over any feedback, corrections, or suggestions. You can also help us pick questions for the podcast by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Ep 29 Roshcast Emergency Board Review
Aug 03, 2017
Success is the sum of small efforts, repeated day in and day out.
-Robert J. Collier
Welcome back to Episode 29! This week we are starting out with a bit of psychiatry before swinging over to the Pediatric ER for a quick neonatal resuscitation. We may even stop by the trauma bay to see what is happening there and give you a chance to win a prize. We’ve said enough already. Let’s get warmed up with a rapid review. This week, we are trying something new – we will be reviewing some of the recentRapidReviews that Yehuda has been uploading to the blog. Make sure to check them out going forward too!
With primary hypothyroidism, you would expect a high TSH and a low T4. On physical, you may see periorbital edema, dry skin, and coarse brittle hair. Patients often complain of weakness, fatigue, facial swelling, constipation, cold intolerance, and weight gain.
With acanthosis nigricans, you would expect thickened, velvety, darkly pigmented plaques on the neck or axillae.
Cushing’s syndrome most commonly caused by hypercortisolism from an ACTH-secreting pituitary tumor. Cushing’s syndrome is diagnosed by a 24h urine cortisol and serum ACTH levels.
Now onto this week’s podcast.
Question 1
You are working in the ED when the police bring in a 26-year-old man who was involved in a bar fight. The patient is well known to staff as he frequently seeks treatment in the ED for injuries related to fights and alcohol abuse. He has been caught smoking cigarettes in the ED bathroom, has urinated on the floor, and been known to steal food trays and other patients’ belongings. As you enter his examination room, you overhear him giving the registration clerk a false identity. Which of the following personality disorders best fits with this patient’s behavior?
A term pregnant patient presents to the ED in active labor and delivery. There is no meconium seen, but the baby has a weak cry and poor tone initially. After clearing the airway, drying the baby vigorously, and providing warmth, the poor tone persists. On exam, the heart rate is 85 and the newborn appears apneic. Which of the following is the most appropriate next step?
A 13-year-old boy with no past medical history presents with a headache 3 days after a closed head injury. The patient states that he stood up from kneeling and hit the top of his head on a wood cabinet. There was no loss of consciousness or seizure activity. In addition to the headache, he complains of difficulty concentrating at school and dizziness. His physical examination is unremarkable. What management is indicated?
An 18-year-old man presents with red eyes. He has been sick with upper respiratory symptoms for two days. Examination is notable for bilateral conjunctival injection with scant discharge. He has rhinorrhea and sounds congested. He has a palpable preauricular lymph node on the left. Which of the following is the most likely cause of his red eyes?
Those with antisocial personality disorder often display a blatant disregard for others, violate societal norms, and lack a remorse for their actions. They are of often aggressive, irritable, and impulsive.
Borderline personality disorder is a cluster B personality disorder and is characterized by self-destructive, impulsive behavior. They often have erratic emotions and may come off as being overly sexual and are frequently in crisis.
Paranoid personality disorder is a cluster A personality disorder. Paranoid patients are often cold, humorless, and suspicious.
Schizoid personality disorder is also a cluster A personality disorder. Schizoid patients are often loners with fewfriends who are indifferent to praise and criticism.
In a neonatal resuscitation, the first step is to warm, dry, and stimulate the neonate and clear the airway if necessary. If there is no response to these measures, begin positive pressure ventilation at a rate of 40–60 breaths per minute.
Bradycardia in a newborn is often a sign of hypoxia.
In a child over 2 with a GCS less than or equal to 14or if are there signs of a basilar skull fracture or signs of AMS, there is a 4.3% chance of a clinically important traumatic brain injury. These children require head imaging.
Postconcussive syndrome may present with many nonspecific symptoms, including headache, dizziness, confusion, amnesia, difficulty concentrating, and blurry vision without a focal neurologic finding.
All patients with postconcussive syndrome should be referred to a neurologist for functional testing and tracking of symptom resolution. Caution patients about returning to contact sports too soon to prevent a second impact.
The most commonlyinjured organ in adult blunt abdominal trauma is the spleen. The liver is the second most commonly injured organ.
Splenic lacerations are graded 1-5. Most can be managed non-operatively. Hemodynamic instability warrants an exploratory laparotomy.
Conjunctivitis most commonly presents with redness, foreign body sensation, drainage, swelling of the lid, and even crusting in the morning. Treatment is supportive with compresses and artificial tears.
The most common cause of conjunctivitis is a viral infection, with adenovirus being the most common virus.
There are four cardinal signs of acute flexor tenosynovitis: 1) tenderness along the course of the flexor tendon 2) fusiform or symmetrical swelling of the finger 3) pain with passive range of motion 4) a flexed posture of the finger.
Flexor tenosynovitis is most commonly caused by penetrating trauma and direct inoculation of the actual sheath, but direct spread from other areas of the hand occur as well.
Flexor tenosynovitis is a surgical emergency and requires antibiotics and hand surgery consultation.
So that wraps up Episode 29. From neonatal resuscitation to personality disorders with a brief stop in the trauma bay, we have covered quite a bit. Hope you all enjoyed. Don’t forget to email us or tweet us if you caught the time of the trauma ring tone to win the prize.
Ep 28 Roshcast Emergency Board Review
Jul 20, 2017
Welcome back to Episode 28! We are already well into intern year. Remember it is a roller coaster, with ups and downs, but in the end, you will really appreciate just how far you have come. This week we start off with a quick ophthalmology review and then dive into the new material, covering OB/GYN, pediatric dermatology, torsades de pointes, and much more. Let’s get started.
Acute angle closure glaucoma classically presents with painful monocular vision loss. The pupil would be fixed and mid-dilated with a hazy cornea and perilimbic injection.
Optic neuritis is characterized by central vision loss with preserved peripheral vision. Patents may also have pain with eye movement and reduced color vision.
Retinal detachment is associated with painless monocular vision loss with floaters and flashing lights. The retina can appear dull and gray. Call ophthalmology immediately for any retinal detachment.
Now onto this week’s podcast.
Question 1
A 27-year-old woman presents with vaginal bleeding. Her last menstrual period was eight weeks ago. On physical examination, there is a small amount of blood in the vaginal vault with an open internal cervical os. Bedside ultrasound reveals an intrauterine pregnancy with a fetal pole but no heartbeat. Which of the following is the most likely diagnosis?
How does the Diagnostic and Statistical Manual (DSM-V) code personality and developmental disorders?
A. Axis I
B. Axis II
C. Section I
D. Section II
Question 3
A 35-year-old woman with a known history of seizure disorder is actively seizing in the ED. Which of the following is the first-line medication and route to treat her seizure?
Which of the following statements is true regarding airway management in children?
A. Adults are more susceptible to airway obstruction than children
B. Children have a lower basal oxygen consumption compared to adults which results in relative protection from hypoxia and decreased need for pre-oxygenation
C. The glottic opening in children is more anterior compared to that of adults
D. The vocal cords are the narrowest portion of the airway in children compared to the cricoid ring in adults
An 11-month old male is brought in by his mother for fever, irritability, and rash. She reports that other children at his daycare have similar symptoms. You see the following on physical exam as seen above. Which of the following is true regarding this condition?
A. Intravenous steroid administration is the mainstay of therapy
B. It is less common in children over 6 years of age
An incomplete abortion occurs before 20 weeks when the os is open and POC are visible either in the OS or in the vaginal canal.
An inevitable miscarriage presents with an open oswithout passage of any products of conception.
A missed abortion is a broader term that describes several conditions, in which the fetus is no longer viable, but remains intrauterine with a closed OS.
A threatened abortion is defined as any vaginal bleeding during pregnancy with a confirmed intrauterine pregnancy and a closed OS.
DSM-V is organized by sections. The multiaxial system of DSM-IV is gone. In DSM-V, Section 2 covers diagnostic categories and Section 3 covers conditions that need additional research.
In an actively seizing patient the first priority is airway protection – roll the patient onto the left lateral decubitus position to prevent aspiration.
The first line pharmacologic management for a patient in status epilepticus is a parenteral benzodiazepine. Midazolam has the fastest onset.
Second line agents for status epilepticus includes phenytoin, fosphenytoin, valproic acid, phenobarbital, or levetiracetam.
Do not forget to check a finger stick and consider INH toxicity in those in status epilepticus.
The glottic opening in children is more anterior to that of adults.
The narrowest portion of the pediatric airway is the cricoid cartilage.
As compared to the adult airway, in the pediatric airway, the tongue is proportionally larger and the epiglottis is longer and narrower.
Staph scalded skin syndrome most commonly affects those under 2 years of age, and it rarely occurs in those over 6 years of age.
Staph scalded skin syndrome is treated with IV fluids, aggressive wound management, and an anti-staphylococcal antibiotic.
Torsades de pointes is associated with a prolonged QT interval, hypomagnesemia, and hypokalemia.
Torsades de pointes is treated with intravenous magnesium.
That wraps up Episode 28. From psychiatry to obstetric emergencies to pediatric dermatology, we have covered the entire spectrum of emergency medicine this week. Hope you all enjoyed. Do not forget to listen for the trauma phone ring tone in the coming weeks for a chance to win a Rosh Review Subscription. Remember to tweet us @Roshcast or email us at Roshcast@roshreview.com the exact time you hear the ring to win the prize.
Ep 27 Roshcast Emergency Board Review
Jul 06, 2017
It is during our darkest moments that we must focus to see the light.
-Aristotle
Welcome back to Episode 27 and a big welcome to all the new interns who are only about 1 week into residency! We hope you find Roshcast to be easy to listen to and helpful in your education. As we have said from the outset, we want this to be as high-yield as possible to not only improve your in-training scores but also improve your care at the bedside. We are open to any suggestions, so please reach out.
Let’s get warmed up with a rapid review – this week, we are going over some HIV-related illnesses.
Toxoplasmosis is rarely seen with CD4 > 200. Be concerned in those with CD4 < 100.
Toxoplasmosis is transmitted through cat feces. It is treated with pyrimethamine, sulfadiazine, and folinic acid.
The classic X-ray finding for PJP pneumonia is diffuse interstitial infiltrates in a “bat wing” appearance.
In PJP pneumonia, if the PaO2 is less than 70 or the A-a gradient is greater than 36, treat with steroids in addition to trimethoprim-sulfamethoxazole.
Now onto this week’s podcast
Question 1
A 67-year-old man with hypertension and end-stage renal disease presents after an incomplete dialysis session secondary to shortness of breath. His vital signs are BP 110/95, HR 65, RR 22, T 37.3°C, and oxygen saturation 99% on 2L NC. You obtain the ECG shown above, which shows a widened QRS, almost resembling a sine wave. Which of the following is the most appropriate next step in this patient’s management?
EMS calls notifying you that there is a mass casualty situation. There was an explosion at a construction site and they will be bringing 20 ambulatory, asymptomatic patients to your emergency department. After checking airway, breathing and circulation, what test, if normal, would allow you to rapidly discharge patients?
A. Abdominal ultrasound
B. Ophthalmoscope evaluation of the eye
C. Otoscope evaluation of tympanic membranes
D. Oxygen saturation
Question 3
A 42-year-old woman with sickle cell anemia presents to the ED complaining of unilateral knee pain. You are worried she might have septic arthritis. Which of the following organisms is most likely to be responsible?
A 29-year-old man presents to the ED with partial-thickness burns to his entire back and right arm. The patient weights 70 kg. Based on the Parkland formula, how much crystalloid solution is required in the first 24 hours?
EKG changes seen in patients with hyperkalemia include peaked T waves, QRS widening, dropped P waves, and bradycardia.
Temporizing measures for managing hyperkalemia include calcium, insulinand glucose, sodium bicarbonate, and albuterol.
Furosemide and dialysis can be used to permanentlyremovepotassium from the body.
For blast injuries, make sure to examine the tympanic membranes. They are damaged at lower pressures than other parts of the body.
Primary blast injuries occur from blast overpressure. Secondary blast injuries are caused by flying debris. Tertiary blast injuries are caused by victims being thrown. And lastly, quaternary blast injuries are caused by environmentalhazardscaused by the explosion.
The most common cause of septic arthritis is Staphylococcus aureus in adults and children over 2, except for sexuallyactive younger adults, in which case Neisseria gonorrhoeae is more common.
On joint aspirate of a septic joint, the white blood cell count is typically greater than 50,000 and the aspirate appears purulent. Remember that if clinical suspicion is high, start antibiotics, consult an orthopedist early, and defer to the gram stain and culture for definitive diagnosis.
The most common extra-articular manifestation of ankylosing spondylitis is uveitis.
The narrowest part of the pediatric airway is the cricoid.
As compared to the adult airway, the pediatric airway has a proportionally smaller larynx, which is more anterior, the epiglottis is longer and narrower, the tongue is proportionally larger, the neck is typically shorter, and the adenoids are often larger.
The pediatric endotracheal tube should be placed to a depth of 3 x the endotracheal tube size.
The parkland formula can be calculated by the formula 4 x % TBSA burned x weight (kg). Give the first half in the first 8 hours and the second half over the next 16 hours.
Although, the parkland formula is a good guide, fluid resuscitation in burns should ultimately be guided by vital signs andurine output. In children, target 1–2 mL/kg/hr, and in adults, target 30 mL/hr.
That wraps up Episode 27. From blast injuries to hyperkalemia, we have covered the entire spectrum of emergency medicine this week. Hope you enjoyed. Do not forget to listen for the trauma phone ring tone in the coming weeks for a chance to win a Rosh Review Subscription. Remember to tweet @Roshcast or email Roshcast@roshreview.com the exact time when you hear the ring to win the prize.
Ep 26 Roshcast Emergency Board Review
Jun 22, 2017
There are two ways of spreading light: to be the candle or the mirror that reflects it.
-Edith Wharton
Welcome back to Episode 26! Remember to listen for a trauma ring tone and if you hear one send us the time via email or tweet us @Roshcast with the time you hear it. This week, we start out with a brief ultrasound review and then get into some ophthalmology, ID, and toxicology. We will discuss a challenging cyanide toxicity question thanks to a suggestion from one of our listeners. Hope you enjoy it!
Lung sliding on bedside ultrasound is a normal finding. Absence of lung sliding is indicative of a pneumothorax.
A lines are a normal finding on lung ultrasound. They are horizontal lines that are reflections of the pleura. B lines are concerning for pulmonary edema and appear as “vertical headlights” throughout the thorax.
Any pregnant patient with lower abdominal pain or vaginal bleeding who doesn’t already have a confirmed intrauterine pregnancy requires a pelvic ultrasound to rule out an ectopic pregnancy.
Now onto this week’s podcast.
Question 1
A 72-year-old man complains of decreased painless vision in his left eye associated with flashing lights and floaters. Visual acuity in the left eye is 20/200 and in the right eye is 20/30. Which of the following is the most likely diagnosis?
A 17-year-old man presents to the ED 30 minutes after intentionally ingesting an unknown amount of drain cleaner. The active ingredient is sodium hydroxide; the pH of the product is 13. Upon arrival, the patient is afebrile, heart rate is 120 beats per minute, blood pressure 130/70 mm Hg, respirations 22 breaths per minute, and oxygen saturation 97% on room air. He appears uncomfortable and reports chest discomfort. There are superficial burns of the oral mucosa and inflammation in the posterior oropharynx, but he is in no respiratory distress. Which of the following is true regarding this patient’s care?
A. Activated charcoal should be administered because the patient presented within an hour of ingestion
B. Dilution with milk or water may be performed
C. Gastric lavage should be performed to prevent systemic toxicity
D. He should be kept NPO in preparation for endoscopy
E. Induction of vomiting with ipecac may be attempted
A 45-year-old man is rescued from a house fire. He was unresponsive at the scene and was intubated by paramedics. Upon arrival, he is afebrile, tachycardic to 130 with a blood pressure of 90/60. His arterial blood gas is significant for a pH of 7.16, a carboxyhemoglobin level of 20%, and a lactate level of 11.5 mmol/L. What is the most appropriate treatment for potential cyanide toxicity in this patient.
A. Administer hydroxocobalamin as a 5 g IV infusion
B. Administer sodium bicarbonate to correct the acidosis
C. Administer the cyanide antidote kit (amyl nitrate, sodium nitrite, sodium thiosulfate)
D. Arrange for the patient to receive immediate hyperbaric oxygen therapy
E. Hyperventilate the patient and maintain FiO2 at 100%
Question 5
An 85-year-old man presents via ambulance after a reported fall. He is non-verbal, bed-bound, and incontinent of urine and stool at baseline. He requires round-the-clock care, which is primarily provided by his daughter, a retired nurse. There are also several grandchildren that assist with his care on a daily basis. The EMS team is concerned for elder abuse and alerts you of their concerns on arrival to the ED. Which of the following factors is associated with a greater likelihood of underlying elder abuse?
Retinal detachment is associated with painless monocular vision loss with floaters and flashing lights. The retina appears as a dull and gray. Retinal detachment is treated surgically or with laser therapy. Consult ophthalmology immediately.
Acute angle closure glaucoma classically presents with painful monocular vision loss. The pupil would be fixed and mid-dilated with a hazy cornea and perilimbic injection.
Optic neuritis is characterized by central vision loss with preserved peripheral vision. Patents may also report pain with eye movement and reduced color vision.
Temporal arteritis is a vasculitis that causes monocular vision loss and is associated with unilateral headaches and polymyalgia rheumatica.
In neonates, 75% of cases of meningitis are caused by Group B strep. Other causes include E. coli, Listeria, and other gram-negative bacilli. Treatment is with cefotaxime and ampicillin or gentamycin and ampicillin
In infants, bacterial causes of meningitis additionally include S. pneumoniae, N. meningitidis, and H. influenzae. Treat this age group with vancomycin, ampicillin, and cefotaxime or ceftriaxone.
In children 3 months to 18 years, the three most common causes of bacterial meningitis are S.pneumoniae,N. meningitidis, and H. influenzae. Treatment is with either ceftriaxone and vancomycin or cefotaxime and vancomycin.
In adults 18 to 50 years old, S.pneumoniae and N. meningitidis, are the most common pathogens. Treat them with ceftriaxone and vancomycin.
In those over 50, in addition to S.pneumoniae andN. meningitidis, gram-negative bacilli and Listeria are also more common cause of bacterial meningitis, so ampicillin must be added to the ceftriaxone and vancomycin.
After an alkali ingestion, early endoscopy is critical as it determines the extent of the injury and helps guide management, disposition, and follow up decisions. All patients should be kept NPO following their ingestion.
Cyanide toxicity can be treated by giving either hydroxocobalamin or with the traditional kit which includes a combination of amyl nitrite, sodium nitrite, and sodium thiosulfate.
For fire victims who also have elevated carboxyhemoglobin levels, cyanide poisoning should be treated with hydroxocobalamin.
In the traditional cyanide overdose kit, the nitrites cause a methemoglobinemia, regenerating the mitochondria, while the thiosulfate aids in excretion.
Elder abuse can come in any form: physical, sexual, emotional, neglect, abandonment, and even financial, failure to recognize it can lead to significant morbidity and mortality.
The lesions of chickenpox appear over days with multiple stages present at once. They first appear at the hairline and spread caudally.
Chickenpox is caused by the varicella-zoster virus, or human herpesvirus type 3. Treatment is supportive with antipyretics, antipruritics, and analgesia.
There are two vaccines for chickenpox – both are live attenuated vaccines and are recommended for all immunocompetent infants over the age of 1 and in all non-infected immunocompetent adults.
That wraps up Episode 26. As always, feel free to submit questions for us to review. Don’t forget to listen for the trauma phone ring tone in the coming weeks for a chance to win a Rosh Review Subscription. Remember to tweet us @Roshcast or email us at roshcast@roshreview.com the exact time you hear the ring to win the prize.
Ep 25 Roshcast Emergency Board Review
Jun 07, 2017
No act of kindness, no matter how small, is ever waster.
-Aesop
Welcome back to Episode 25—our silver anniversary episode! It was great connecting with a few listeners recently at SAEM. At the beginning of this week’s episode, we announced a new contest – be the first to tweet to us (@Roshcast) or email (Roshcast@roshreview.com) the exact time in episodes 26-30 that you hear a trauma phone ring tone to win a 30-day subscription to Rosh Review! First, let us get started with a rapid review covering fish poisonings.
Hot and cold sensation reversal is classically associated with ciguatera poisoning.
In scombroid poisonings, patients have reported a metallic, bitter, or even peppery taste.
In scombroid poisonings, histidine is broken down into histamine. Treat patients supportively with antihistamines.
Now onto this week’s podcast
Question 1
You are on a 10-day mountain climbing excursion in Colorado with one of your 55-year-old coworkers. After ascending to an altitude of 9200 feet, your coworker develops a mild bifrontal headache associated with nausea. He reports feeling “hung over” but denies drinking any alcohol the previous night. He has no other symptoms. On examination, there are no focal neurologic deficits. He desires to continue the climb. Which of the following is the most appropriate next step in the management of your coworker?
A 27-year-old woman, G2P1, presents with vaginal bleeding and right lower quadrant pain. She reports a positive pregnancy test and LMP 6 weeks prior to her evaluation. Vital signs are T 98.6°F, BP 110/68, HR 72, and RR 16. Her abdomen is soft with mild tenderness in the right pelvic area. Pelvic examination is notable for a small amount of red blood in the vagina and mild right adnexal tenderness. Bedside ultrasound shows an empty uterus and adjacent to the right ovary a gestational sac with yolk sac and fetal pole. Which of the following is a contraindication to methotrexate administration?
A. Fetal heart activity
B. Gestational sac greater than 2.5 cm in diameter
A 32-year-old woman, G2P1, at 33 weeks gestation presents to the emergency room for sharp abdominal pain. She has not had any prenatal care during this pregnancy. Her symptoms include vaginal bleeding, uterine pain between contractions, and fetal distress. Her first pregnancy was uncomplicated, with a vaginal delivery at term. Which one of the following is the most likely diagnosis?
An 18-year-old woman presents with fever, confusion, weight loss, and palpitations. Her vital signs are T 100.7°F, HR 140, BP 143/93, RR 20, oxygen saturation 95%, and finger stick glucose of 118. Physical examination reveals a thin woman who is alert and oriented x3 with a regular, fast heart rate, and brisk reflexes. Her roommate tells you that the patient has been taking a friend’s levothyroxine in an attempt to lose weight. What management should be initiated?
A. Beta-blocker
B. Beta-blocker, dexamethasone
C. Beta-blocker, dexamethasone, propylthiouracil, and potassium iodide
A 53-year-old man complains of fever and non-productive cough. He is also short of breath with exertion. His X-ray is shown above. Which test will be an important part of his overall evaluation?
Acute mountainsickness is characterized by headache, nausea, dizziness, and sleep disturbances after rapid ascent of an unacclimatized person at 2000 meters or higher.
Mildacute mountain sickness should be treated first by halting ascent and then supportively with fluids, oxygen, analgesia, and anti-emetics. Acetazolamide and dexamethasone can be used as a second-line agent.
When medically managing an ectopic pregnancy, methotrexate is relatively contraindicated when fetal heart activity is present, and contraindicated with hemodynamic instability or evidence of rupture on ultrasound. To be eligible for the treatment you need to have a gestational sac less than 3.5 cm and be able and willing to comply with post-treatment monitoring.
Riskfactors for an ectopic pregnancy include prior ectopic pregnancies, history ofPID, tubal surgery, or an IUD.
The fallopian tube is the most common location of an ectopic pregnancy.
Interstitial ectopicpregnancies occur with implantation of the developing fetus in the interstitium of the myometrium. In such cases, the sac may have an eccentric appearance on sonography, but there would be a thin endomyometrial mantle.
Placental abruption typically manifests as painful vaginal bleeding with evidence of fetal distress in the third trimester. Often the fundus will be tender and the patient will likely have pain between contractions.
Common risk factors for placental abruption include abdominal trauma, maternalhypertension, smoking, cocaine use, multiple gestation, and previous abruption.
Uterine rupture classically presents with a sudden tearing uterine painwith contractions with pain free intervals between contractions.
Placenta previa usually manifests as painless vaginal bleeding in the late 2nd or 3rd trimesters due to placental tissue overlying the internal cervicalos.
Vasa previa occurs when the umbilical cordinserts into the membranes of the lower uterinesegment and amniotic blood vessels present in front of the fetal head. This usually presentswith hemorrhage after amniotomyor spontaneous rupture of membranes.
Esophageal rupture carries significant morbidity and mortality. It should be treated with immediate antibiotics and a surgical consultation.
More than 90% of spontaneous esophageal ruptures occur in the distal esophagus.
With blunt trauma to the neck or thorax, esophageal rupture is usually in the proximalormiddle third of the esophagus. Iatrogenic injuries frequently occur at the pharyngoesophagealjunction.
Endogenous thyroid storm is treated with beta-blockers, PTU, potassium iodide, and dexamethasone. Exogenous thyroid storm is treated with beta-blockers and dexamethasone.
In thyroid storm, propranololreduces peripheral conversion of T4 toT3. PTUblockssynthesis of thyroid hormone.
Potassium iodideblockstherelease of thyroid hormone. Dexamethasoneblocks the peripheral conversion of T4 to T3 in addition to treating the relative adrenal insufficiency.
PJP, formerly PCP pneumonia, is typically seen in those who are immunocompromised. The x-ray will have bilateral interstitial infiltrates in a bat wing configuration. If the PaO2 is lessthan 70or the A-a gradient is greater than 35, treat with steroids in addition to trimethoprim-sulfamethoxazole.
So, that wraps up Episode 25. Do not forget to listen for the trauma phone ring tone in the coming weeks for a chance to win a Rosh Review Subscription. Remember to tweet (@Roshcast) or email (Roshcast@roshreview.com) the exact time you hear the ring to win the prize.
Ep 24 Roshcast Emergency Board Review
May 17, 2017
Shoot for the moon and if you miss you will be among the stars.
-Les Brown
Welcome back to Episode 24! We are coming to you live from Orlando at SAEM this week. Ok, it is not exactly live, but we are launching this episode from Orlando. Although the venue has changed, we have the same high-quality review for you this week. This week we begin with a renal rapid review and then get into the new material, starting with some OB and virology, and ending with the more obscure, but still important, altitude-related emergencies. Hope you enjoy!
When considering children with glomerulonephritis, in a child with mild to moderate edema, a normal blood pressure, and no respiratorysymptoms, discharge home with corticosteroids may be appropriate.
Winter’s formula, pCO2 = 1.5HCO3– + 8 ± 2, is used to determine if there is appropriate respiratory compensation in a metabolic acidosis.
The causes of a non-anion gap metabolic acidosis can be remembered with the mnemonic HARDASS: Hyperalimentation, Addison’s disease, RTA, Diarrhea, Acetazolamide, Spironolactone, and Saline infusion.
Now onto this week’s podcast
Question 1
A 17-year-old G1P0 woman at 25 weeks gestation presents with intermittent blurred vision. On presentation, she is asymptomatic. Vital signs are HR 84, BP 175/113, and oxygen saturation 97%. Physical examination reveals 2+ pitting edema on both lower extremities and urinalysis has 3+ protein on dip. Which of the following is most likely indicated?
A. Admit for further obstetrics evaluation
B. Antiepileptic medications
C. Arrange follow-up with the patient’s obstetrician
A 14-year-old girl is brought to your mountaineering base camp at 11,000 feet for evaluation of strange behavior while attempting to summit a nearby peak with her school group. What is the most sensitive clinical sign in diagnosing high-altitude cerebral edema?
A 33-year-old man presents to the ED with right eye pain, tearing, and “difficulty seeing” out of the right eye. His visual acuity is 20/30 on the left and 20/200 on the right. On physical exam, you notice a subconjunctival hemorrhage and teardrop-shaped pupil. Which of the following physical exam findings is consistent with the suspected diagnosis?
A. Cells and flare in the anterior chamber on slit lamp exam
B. Gross retinal hemorrhage on dilated funduscopic exam
Preeclampsia is defined as gestational hypertension after 20 weeks, with a blood pressure of 140/90 or higher and either proteinuria or signs of end-organ damage.
The definitive and curative therapy for preeclampsia is delivery of the baby. Magnesium may be given for seizure prophylaxis.
Both hydralazine and labetalol can be safely used in pregnancy to control blood pressure.
HELLP syndrome is a severe variant or complication of preeclampsia. It is characterized by hemolysis, elevated liver enzymes, and low platelets.
Scombroidpoisoning may cause a metallic, bitter, or even peppery taste.
Scombroid poisoning results from the breakdown of histidine into histamine resulting in facial flushing, diarrhea, severe throbbing headache, palpitations, and abdominal cramps.
Ciguatera poisoning leads to nausea, vomiting, diarrhea, myalgias, tingling and numbness, abdominal pain, and vertigo along with the classic association of hot and cold sensation reversal. In severe cases, hypotension, bradycardia, and coma may result.
The most common viralcause of pneumonia in adults is influenza.
Influenza is also the most common viralcause of rhabdomyolysis.
Splenic artery aneurysms are the most common visceral artery aneurysm.
Splenic artery aneurysms are managed with embolization in asymptomatic patients and operatively in those who are symptomatic.
The most sensitive clinical sign for diagnosis of high altitude cerebral edema (HACE) is cerebellar ataxia. Other signs include encephalopathy, severe lassitude, and a progressive decline of mental function and consciousness.
HACE is managed definitively with descent. Steroids, supplemental oxygen, and hyperbarics may also be used.
Globe rupture can be identified by a positive Seidel test on fluorescein stain exam. CT can also help in making the diagnosis.
Globe rupture should be managed by covering the eye with a shield, elevating the head of the bed, updating the tetanus vaccine, and starting antibiotics. Operative emergent repair is a must.
So that wraps up Episode 24. We will be in Orlando for a few more days, so please stop us and let us know what you think. We are always looking for ways to make Roshcast even better and are open to any ideas and suggestions. As always, don’t forget to follow us on Twitter @Roshcast for updates, high-yield images, and pearls in 140 characters or less.
Ep 23 Roshcast Emergency Board Review
May 04, 2017
We aim above the mark to hit the mark.
-Ralph Waldo Emerson
Welcome back to Episode 23! It was great running into a few listeners at CORD last week and hearing your feedback. This week, we start off with an OB/GYN related pharmacology review before jumping into the new material. Hope you enjoy!
Cervicitis is treated with ceftriaxone 250 mg IM and azithromycin 1 g PO.
Bacterial vaginosis is treated with metronidazole twice daily for 7 days.
Oxytocin or the prostaglandins can both be used in cases of maternal hemorrhage after delivery.
Now onto this week’s podcast
Question 1
A 16-year-old man presents to the ED complaining of 3 days of nasal rhinorrhea, cough, myalgias, and generalized malaise. After a coughing episode yesterday, he developed pleuritic chest pain radiating to the left neck. His vital signs are BP 130/70 mm Hg, HR 76, RR 16, T 36.6°C, and pulse oximetry 98% on room air. You obtain the chest radiograph seen above. Which of the following is the most appropriate next step in management?
A. Discharge home with close follow–up
B. Endoscopy
C. Needle decompression
D. Tube thoracostomy
Question 2
A 17-year-old man with no past medical history presents complaining of constant chest pain for 5 days. He states that he had a cold 2 weeks ago and feels like he never got better. His vitals are T 36.8°C, HR 91, BP 122/75, RR 18, and oxygen saturation 99%. A 12-lead ECG is performed as seen above. What is the appropriate immediate management for this patient?
A. Aspirin 325 mg and activation of the cardiac catheterization lab
B. Azithromycin 500 mg by mouth, followed by 250 mg once a day for 4 days
C. Ibuprofen and prompt follow–up with his primary care doctor
An 84-year-old woman with new-onset altered mental status is sent to the ED from her assisted living facility. According to the facility staff, she has had a productive cough for two days. Her vital signs are blood pressure 90/60 mm Hg, heart rate 92 beats per minute, respiratory rate 25 breaths per minute, temperature 38.3°C, and oxygen saturation 95% on room air. Laboratory results reveal a WBC of 11,000. A chest radiograph shows a right lower lobe infiltrate. Which aspect of this patient’s presentation is consistent with systemic inflammatory response syndrome?
A 27-year-old woman presents with a complaint of transient vision loss in her right eye. She states that she has had multiple similar episodes in the past 6 months. She also complains of incomplete bladder emptying, intermittent tremors and intermittent weakness in her left arm. The patient has a family history of multiple sclerosis. Which of the following is the best diagnostic test for the suspected diagnosis?
A father brings his 2-week-old newborn to the ED after a gagging episode at home where the infant “turned blue.” The newborn was sleeping in his father’s arms when he started choking, turned blue, and went limp. The father turned the baby over, did 5 back blows, and performed CPR for 5 minutes until the newborn started crying. On exam, the newborn appears sleepy but is easily arousable. Vital signs are HR 160, RR 30, T 37.6°C, and pulse oximetry is 99% on room air. Which of the following is the next best step in management?
A. Admit to hospital for further workup
B. Endotracheal intubation
C. Epinephrine (1:10 000) IV
D. Send home with reassurance
Pneumomediastinum requires no treatment and patients may be safely discharged.
The SIRS criteria are met if two of the following conditions are met: a heart rate > 90, a temperature > 38° C or < 36° C, a respiratory rate > 20 or a PaCO₂ < 32, or a WBC > 12,000 or < 4,000.
Multiple sclerosis classically presents with symptoms that are scattered in time. They can range from motor to sensory and can include bladder dysfunction.
So that wraps up Episode 23. Don’t forget to subscribe so Roshcast episodes are downloaded automatically as they are released. Follow us on Twitter @Roshcast for updates, high-yield images, and pearls in 140 characters or less. We’ll also be at SAEM in two weeks, so feel free to pull us aside and let us know what you think. We are constantly striving to make Roshcast as high yield as possible and welcome all feedback!
Ep 22 Roshcast Emergency Board Review
Apr 20, 2017
No matter what people tell you, words and ideas can change the world.
-Robin Williams
Welcome back to Episode 22! This week, we have some bread-and-butter emergency medicine with a lot of deeper learning points, so pay close attention as you listen through. Let’s start out with a review of pediatrics before we jump into the new material.
In treating epiglottitis, the first priority is airway management. Once the airway has been secured, it can be treated with either ampicillin-sulbactam or ceftriaxone.
The five congenital cyanotic heart defects can be remembered with the numbers 1 to 5.
One for trucus arteriosus in which the two vessels join to make one.
Two for transposition of the great vessels in which the two great vessels are switched.
Three for tricuspid atresia, remember three for tricuspid.
Four for the four defects of tetralogy of Fallot.
Five for the five words in total anomalous pulmonary vascular return.
The three common acyanotic heart lesions are atrial septal defects, ventricular septal defects, and patent ductus arteriosus
Now onto this week’s podcast
Question 1
A 19-year-old woman presents with acute onset of shortness of breath and chest pain. The patient’s chest X-ray is shown above. Which of the following provides definitive management for the condition?
A 25-year-old 36-week pregnant woman presents to the ED with a complaint of vaginal bleeding. She denies associated cramping, abdominal pain, or preceding traumatic event. She describes the blood as “bright red.” Which of the following is a risk factor for the development of this condition?
An 18-year-old man presents with an injury to his left index finger. The patient was cleaning the nozzle of a high-pressure paint injector when it fired and punctured his finger. The patient reports pain at the site. On exam, you note a small puncture wound and no exit wound. There is no erythema and the site is mildly tender to palpation. Plain films do not demonstrate a fracture. Which of the following is the most appropriate next step in management?
A 34-year-old woman with HIV presents with a cough and shortness of breath. Her oxygen saturation is 93% on room air, partial arterial oxygen tension of 75 mm Hg, and A-a gradient of 30 mm Hg. Her chest X-ray is shown above. What treatment is indicated?
A 16-year-old girl presents with pain to the right index finger after slamming it in a car door. Physical examination reveals a 50% subungual hematoma, and an X-ray shows a nondisplaced distal tuft fracture. What management is indicated?
A. Oral antibiotics, splinting, and follow-up
B. Splinting and follow-up
C. Trephination, splinting, and follow-up
D. Trephination, splinting, oral antibiotics, and follow-up
A tension pneumothorax may be managed immediately with needle decompression. Definitive management is with chest tube placement.
In patients with a pneumothoraxmore than a few days old, rapid re-expansion of the lung can lead to re-expansion pulmonary edema.
Placenta previa is caused by placental implantation in the lower uterine segment, either completely or partially overlying the cervical OS.
Placenta previa typically causes painless, bright red vaginal bleeding in the 2nd or 3rd trimester. The abdominal exam will be benign.
Risk factors for placenta previa include prior caesarean section, advanced maternal age, grand multiparity, previous placenta previa, multiple gestations, previous multiple induced abortions, and preterm labor.
High-pressure injection injuries should be treated with broad-spectrum antibiotics, extremity elevation, and hand surgery consultation. They carry significant morbidity with delayed treatment leading to tissue necrosis, infection, and possible amputation.
Suspect an air embolism whenever any diver loses consciousness upon ascent or within 10 minutes of surfacing.
Air embolisms can cause a wide range of symptoms, including stroke-like symptoms, dyspnea, hemoptysis, chest pain, and dysrhythmias. They are treated with hyperbaric recompression.
Nitrogen narcosis occurs in dives beyond 100 feet due to an increased concentration of dissolved nitrogen. Symptoms including impaired motor functionand behavior problems.
The bends is a dysbarism that occurs due to rapid ascent. It presents with diffuse muscle and joint pain due to nitrogen bubble release into the tissues.
PJP Pneumonia is associated with diffuse interstitial infiltrates, classically in a batwing appearance. It is treated with trimethoprim-sulfamethoxazole. If the arterial oxygen tension is less than 70 or the a-a gradient is greater than 35, corticosteroids have been shown to reduce mortality.
Histoplasmosis is found in the Ohioand Mississippi river valleys and is associated with bird and bat droppings.
Blastomycosis is found in the southeast US. In addition to pneumonia, it can cause bonelesions.
Coccidioidomycosis is found in the southwest US. It is associated with erythemanodosum and arthritis.
Legionella pneumonia is associated with hyponatremia and gastrointestinal symptoms.
Distal tuft fractures are treated with nail trephination (if indicated), splinting, and follow up.
Nail trephination can be accomplished with a heated 18-gauge needle or paperclip, or with an electrical cautery device. A single hole usually adequately relieves the pressure with the evacuation of a drop or two of blood.
That wraps up Episode 22. Remember to follow us on Twitter @Roshcast for updates and high yield EM pearls in 140 characters or less. Curious about the data driving Rosh Review? Check out Sean Michael’s post to get an inside look at the data and the educational philosophy at Rosh Review. Hope to see some of you at CORD!
Ep 21 Roshcast Emergency Board Review
Apr 05, 2017
Change your thoughts and you change your world.
-Norman Vincent Peale
Welcome back to Episode 21! We are all over the place this week, tackling topics from orthopedics to electrolyte abnormalities. Thanks to our listeners for the excellent feedback. Keep it coming to roshcast@roshreview.com. Let’s get started with a quick neurology rapid review from prior episodes!
Treatment for a radial nerve palsy is supportive with a wrist splint, and the condition is typically self-limited.
VP shunt obstruction occurs proximally more often than it occurs distally. Proximal VP shunt obstruction occurs due to choroid plexus obstruction or increased protein within the CSF. Distal VP shunt obstruction occurs due to abdominal pseudocyst formation, which typically presents with abdominal pain due to the large size of the cyst.
Lyme disease is the most common cause of a bilateral Bell’s palsy. Remember that a peripheral facial nerve palsy can be distinguished from a central one by involvement of the forehead.
Now onto this week’s podcast
Question 1
A patient presents to you as a transfer from an outside facility with the radiograph seen above. Which of the following exams will evaluate for the most commonly associated nerve injury in this type of fracture?
A 24-year-old man is brought to the ED after sustaining a stab wound to the right side of his chest. He is diagnosed with a hemothorax and a 38-French chest tube is placed in the resuscitation room. Which of the following best predicts the need for urgent thoracotomy?
A. Initial chest tube output of greater than 1,000 mL of blood
B. Initial chest tube output of greater than 10 mL/kg of blood
C. Persistent output of greater than 100 mL of blood per hour for the first 3 hours following chest tube placement
D. Persistent output of greater than 7 mL of blood per kilogram per hour following chest tube placement
A 45-year-old woman with a history of hypertension and atrial fibrillation presents with a complaint of sudden onset vision loss in her right eye that occurred 10 minutes prior to arrival in the emergency department. She denies associated pain or trauma to the eye. Visual acuity is 20/20 at baseline, however she can now only count fingers on the right. What is the appropriate next step?
A. Arrange for 24-hour follow-up with ophthalmology
A 19-year-old man presents to the ED after jamming his finger while playing basketball. On exam, he has swelling and tenderness to the proximal interphalangeal joint and pain with proximal interphalangeal joint extension. An X-ray is negative for a fracture. To prevent the deformity seen in the above image from developing, what type of splint should be placed?
A. Distal interphalangeal joint in extension, proximal interphalangeal joint and metacarpal phalangeal joint with full range of motion
B. Distal interphalangeal joint, proximal interphalangeal joint, and metacarpal phalangeal joint in extension
C. Proximal interphalangeal joint in extension, distal interphalangeal joint and metacarpal phalangeal joint with full range of motion
D. Proximal interphalangeal joint in flexion, distal interphalangeal joint in extension, and metacarpal phalangeal joint with full range of motion
A Galeazzi fracture is a fracture of the middle to distal third of the radius with dislocation or subluxation of the distal radioulnar joint.
In Galeazzi fractures, the anterior interosseous nerve (or AIN) is at risk. Check its function by testing the flexor pollicis longus and the flexor digitorum profundus by asking the patient to make an “OK” sign.
Asking the patient to show you a “thumbs up” tests the radial nerve.
The ulnar nerve is innervated by the C8–T1 spinal nerve roots.
Hypomagnesemia can be seen in patients with chronic malnutrition, including alcoholics, children with restricted diets, and in the elderly. It is also seen in patients on diuretics, those taking aminoglycosides, and patients on a PPI. Concomitant hypokalemia is common.
Hypomagnesemia typically presents with vague symptoms including muscle cramping and diffuse weakness. More serious complications include vertigo, ataxia, seizures, increased reflexes, and cardiac conduction abnormalities, such as atrial fibrillation, PVCs, and ventricular tachycardia.
Indications for emergent thoracotomy in a patient with a traumatic hemothorax include:
Initial chest tube drainage of over 20 ml/kg of blood
>3 mL/kg/hr of blood for 4 hours
Persistent bleeding of over 200 ml/hour for 3 hours
Persistent bleeding of 7 ml/kg/hour
Refractory shock
Chest that remains more than half full of blood on chest X-ray despite tube insertion
Traumatic hemothorax is usually due to lung parenchymal injury which is usually self-limited. It may also be due to small or large vessel vascular injury or even cardiac injury.
Central retinal artery occlusion (CRAO)risk factors include hypertension, atrial fibrillation, diabetes, valvular heart disease, arteriosclerosis, hyperlipidemia, sickle cell anemia, carotid artery disease, and vasculitis.
CRAO typically presents with acute painless vision loss followed by the development of a Marcus-Gunn pupil. On exam, you would expect a pale retina and cherry red macula.
Treatment for CRAO includes digital globe massage and medications like acetazolamide, mannitol, topical timolol, and sublingual nitro. More advanced measures include hyperbaric oxygen and anterior chamber paracentesis.
A boutonnière deformity, which has PIP flexion and DIP extension, is most commonly caused by rheumatoid arthritis, but may also be caused by trauma. In the traumatic setting, it is typically caused by a central slip injury.
To treat presumed traumatic central slip injury, splint the patient in PIP extension, leaving the DIP and MCP in full ROM. If there is an associated fracture, internal surgical fixation may be required.
Anticonvulsant hypersensitivity syndrome, now more broadly classified under DRESS, presents with a 1–2 week period of nonspecific symptoms followed by a diffuse erythematous rash. Severe cases are associated with fever, rash, and internal organ involvement and carry a 10% mortality.
Treatment for DRESS is with IV steroids and immunoglobulin, in addition to supportive care and cessation of the offending agent.
So that wraps up Episode 21. Remember to follow us on Twitter @Roshcast and check out the new Teaching Image series on the blog.
Ep 20 Roshcast Emergency Board Review
Mar 23, 2017
As knowledge increases, wonder deepens.
-Charles Morgan
Welcome back to Episode 20! We have a great episode lined up for you this week, again covering topics that run the gamut of Emergency Medicine. We are excited to say that we have covered over 100 questions in approximately five hours of Roshcast over six months! As always, send us any feedback or suggestions to roshcast@roshreview.com. Let’s get going with this week’s content!
TTP is treated with plasmapheresis. If plasmapheresis cannot be performed expediently, FFP can be used as a temporizing measure.
For any patient on warfarin with a life-threatening bleed, FFP, PCC, or Recombinant factor VIIa should be given. For a patient on aspirin with a life-threatening bleed, DDAVP should be given in addition to platelets.
For patients with intracranial hemorrhages, new evidence from the PATCH trial suggests that platelets may actually increase the risk of death and dependence, so such patients should only be given DDAVP.
Both Hemophilia A and B are X-linked recessive disorders.
Now onto this week’s podcast
Question 1
A 23-year-old man presents with chest tightness after intranasal cocaine use. Vital signs are HR 133, BP 155/95, and oxygen saturation 95%. ECG reveals sinus tachycardia with no ischemic changes. What medication should be administered?
A 59-year-old man is found naked under a bridge. He is unresponsive and does not respond to painful stimulation. His rectal temperature is 32ºC. The patient is intubated for airway protection, warm blankets are placed, and active internal rewarming measures are initiated. The patient’s temperature slowly rises to 35ºC, but then begins to fall. Which of the following is most likely responsible for this phenomenon?
A. Cooling of blood during cardiopulmonary circulation
A 32-year old woman with HIV presents for the evaluation of a headache. She denies fever and her neurologic examination is normal. A CT scan of the head is performed and shown above. Which of the following is true regarding the finding on the CT scan?
A. It is caused by reactivation of a previous infection
B. It is transmitted through dog feces
C. The CD4 count is typically less than 50 cells/mm3
A woman suffers from an acute attack of vertigo, nausea, and vomiting. You suspect viral labyrinthitis. Which of the following medications is the best choice in treating the vertigo?
In the PATCH trial, platelets were shown to increase the risk of death in acute intracranial hemorrhage in patients on aspirin.
Cocaine chest pain should be treated with benzodiazepines to both relieve vasospasm and decrease sympathetic surge.
Beta-blockers should be avoided in those with cocaine chest pain due to unopposed alpha agonism.
The most common type of migraine is a migraine without an aura.
The classic migraine is a slow onset, unilateral, pulsating, headache with moderate to severe intensity. It may be associated with nausea, vomiting, photophobia, or phonophobia.
Migraines affect women twice as often as they affect men.
The most typicalmigraine auras are visual.
When actively rewarming a patient, a decrease in core temperature is common as cold blood returns from the periphery.
In hypothermia, expect a 2% increase in the hematocrit for every 1 degree Celsius drop in temperature.
Salicylate overdoses are associated with poor fetal outcomes as salicylates readily crossthe placenta, causing acidosis, kernicterus, and prematurely closure of the ductus arteriosus.
The treatment for a salicylate overdose is gastric decontamination, urinary alkalization, and hemodialysis.
Indications for dialysis in a salicylate overdose are altered mental status, renal failure, pulmonary edema, rising levels despite alkalinization, coma, or clinical deterioration.
In carbon monoxide poisoning in pregnancy, the threshold for initiating hyperbaric oxygen therapy is lower as the half-life of carbon monoxide is almost 5 times longerin the fetus than in the mother.
Toxoplasmosis occurs due to reactivation of a prior infection in patients with HIV and a CD4 count less than 100. It is transmitted through cat feces and can cause encephalitis. Treatment is with pyrimethamine, sulfadiazine, and folinic acid.
Viral labyrinthitis should be treated with rest, hydration, antiemetics, vestibular depressants, and corticosteroids. Benzodiazepines may also be used.
That wraps up Episode 20. Don’t forget to follow us on Twitter @Roshcast for updates and high-yield EM pearls in 140 characters or less. We will primarily be posting on material that we have already covered on the podcast to add yet another element of spaced repetition. Be sure to take full advantage! And take a look at our new Teaching Image series on the blog. The first three posts are already up: Cardiac Tamponade, Tinea Versicolor, and Basilar Skull Fracture.
Ep 19 Roshcast Emergency Board Review
Mar 09, 2017
Knowing is not enough; we must apply. Willing is not enough; we must do. -Johann Wolfgang von Goethe
Welcome back to episode 19! We are certainly relieved to have this year’s in-training exam behind us, and we are sure you are too. We hope you recognized some of the content we reviewed in episodes 1-15 and were able to grab a few extra points. Now that we’ve all had a brief break, we are back with new material to help you prepare for next year’s exam and to help improve your clinical acumen. It is important to keep reviewing all year-round.
The Nexus criteria are used to rule out the need for cervical spine imaging. Use the mnemonic NSAID to remember the criteria: neurologic deficit, spinal tenderness, altered mental status, intoxication, and distracting injury.
A pneumothorax can be identified on lung ultrasound by the absence of lung sliding.
A simple pneumothorax, which is one involving less than 10% of the hemithorax, can be treated with a non-rebreather. Larger pneumothoraces will often require a chest tube or a pigtail catheter.
The most common EKG finding for a myocardial contusion is sinus tachycardia. The most common course is a spontaneous resolution of the symptoms. However, with severe injuries, the mostserious complication is delayed rupture.
Now onto this week’s podcast
Question 1
A 55-year-old man who is taking several antihypertensive medications presents to the ED with nausea, vomiting, shortness of breath, and a rash after eating a home-cooked Thai meal at a friend’s house about 1 hour ago. The symptoms began within seconds of the first bite of his meal. Despite the patient being administered 2 doses of intramuscular epinephrine, diphenhydramine, dexamethasone, and crystalloid fluids, his blood pressure remains at 75/38 mm Hg. Which other medication should be considered in this patient?
A. Cimetidine
B. Glucagon
C. Norepinephrine
D. Octreotide
Question 2
A 45-year-old woman with type 1 diabetes mellitus presents with fatigue in the setting of medication non-compliance. Her laboratory tests reveal a Na+ 125, K+ 3.1, chloride 97, bicarbonate 10, glucose 761, and pH 7.21. The patient is started on intravenous fluids. What therapy is most important to start next?
A 56-year old woman with a known left bundle branch block presents after a syncopal episode. EKG shows a regular, wide complex tachycardia with a rate of 160 beats/minute. Which of the following EKG features suggests a diagnosis of ventricular tachycardia over a diagnosis of supraventricular tachycardia with aberrancy?
A 74-year-old woman with a history of congestive heart failure, hypertension, and coronary artery disease presents with confusion, abdominal pain, and nausea. Her medications include hydrochlorothiazide, aspirin, and digoxin. The patient’s ECG is shown above. She has a potassium level of 6.3 mEq/ml. Which of the following treatments should be initiated?
An 18-year-old woman with no significant past medical history falls while rock climbing and sustains a knee dislocation. Posterior tibial and dorsalis pedis pulses are unable to be palpated on the affected side. Her last meal was 2 hours ago. Which of the following statements is true regarding pre-procedural fasting?
A. Current fasting guidelines are based on results of randomized controlled trials comparing fasting status and incidence of aspiration
B. She is at risk of complications from knee dislocation and reduction should be performed regardless of fasting status
C. She should wait an additional 4 hours, until it is 6 hours since her last meal, since she is at increased risk of aspiration
D. Vomiting and loss of airway reflexes during procedural sedation is common
Question 6
A 32-year-old woman who is 8 weeks pregnant by dates presents to the ED with a 2-cm laceration to her index finger sustained while she was cutting a tomato. On review of systems, she also notes 2 days of vaginal spotting and lower abdominal cramping. Vital signs are within normal limits. Physical exam is consistent with a simple 2-cm laceration. The pelvic exam reveals a closed os and no adnexal tenderness or masses. Which of the following statements best describes the next step in management?
A. Delay treating her laceration until her pregnancy status is further clarified
B. Treat her laceration as indicated, and perform a beta-hCG quantitative level
C. Treat her laceration as indicated, perform a beta-hCG quantitative level, and obtain a pelvic ultrasound
D. Treat her laceration as indicated, then discharge with outpatient obstetrical follow-up
Glucagon may be used for beta-blocker reversal.
Common side effects of glucagon are vomiting, dizziness, hypokalemia, hyperglycemia, hypertension, and tachycardia.
When treating DKA, replete potassiumbefore starting insulin. Most protocols advocate for a potassium of at least 3.5 before starting insulin.
Capture beats and fusion beats are indicative of ventricular tachycardia.
A capture beat is a narrow complex supraventricular beat that is conducted within a run of ventricular tachycardia.
A fusion beat is a beat formed from a supraventricular and ventricular impulse, resulting in a hybrid QRS complex.
Digoxin toxicity can cause confusion, abdominal pain, nausea and vomiting as well as almost any type of dysrhythmia. PVCs are the most common EKGabnormality.
The Salvador Dali mustache or scooped ST segments seen in patients on digoxin is indicative only of digoxin use and not toxicity.
In digoxin overdoses, the potassium levels are helpful in prognosticating survival. A potassium level of > 5.5 mEq portends a worse outcome. The treatment is digoxin-specific antibody.
Charcoal binds digoxin and can be given in acute overdoses if the patient has a normal mental status. There is no role for hemodialysis.
Procedural sedation should not be delayed because the patient is not fasting. There is no good literature to suggest worse outcomes in those not fasting.
In any pregnant patient with lower abdominal pain or vaginal bleeding, who does not yet have a confirmed IUP by ultrasound, a beta-hCG and pelvic ultrasound are required to rule out an ectopic pregnancy.
Up to 20% of all pregnant patients will develop vaginal bleeding within the first 20 weeks of gestation. Of these, 50% will miscarry and the other 50% will go on to have a term pregnancy.
Thanks to Megha for the question suggestion. Remember to write “Roshcast” in the submit feedback box as you work through the question bank to flag questions you would like us to cover in future episodes.
For those of you thinking it is too early to start studying, do not forget there are 1200 questions in the Rosh review bank so you are better off starting sooner rather than later to get through it. Many of you already have the yearly subscription, so take full advantage by reviewing the questions there now. Lastly, follow us on Twitter at @Roshcast for updates and high-yield EM pearls in 140 characters or less!
Ep 18 Roshcast Emergency Board Review
Feb 18, 2017
Believe you can and you’re halfway there.
–Theodore Roosevelt
Welcome back to Episode 18! This is the last and final rapid review before the In-Training Exam! Remember to pause the podcast as you go through the review and quiz yourself. Let’s get started with Ob/GYN.
OB/GYN Emergencies
The most common cause of maternal mortality during delivery is maternal hemorrhage. Maternal hemorrhage can be caused by uterine atony, genital trauma or retained products. Uterine atony is treated with oxytocin or uterine massage. Genital trauma is treated with pressure or ligation. Retained products require removal of the products to control the hemorrhage.
Vaginal candidiasis is treated with fluconazole or clotrimazole. Bacterial vaginosis is treated with metronidazole, twice daily for 7 days. Lastly, trichomoniasis is treated with a single dose of metronidazole.
PID is typically caused by gonorrhea, chlamydia, or both. It is treated with ceftriaxone 250 mg IM once and doxycycline 100 mg PO BID x 14 days if the patient can tolerate PO. Cervicitis is treated with ceftriaxone 250 mg IM and azithromycin 1g PO.
Fitz-Hugh-Curtis syndrome is a perihepatitis associated with PID. It is a difficult diagnosis to make, but suspect it in sexually active woman with right upper quadrant pain.
Pediatric Emergencies
Suspect epiglottitis in those who were incompletely vaccinated. The first priority is airway management, which ideally involves intubation in an operating room. The second priority is antibiotics. Ampicillin-sulbactam or ceftriaxone are often used.
Pertussis has three stages: the catarrhal stage, the paroxysmal stage, and the convalescent stage. Treatment is with a macrolide.
There are five common congenital cyanotic heart defects, which can be remembered by the numbers 1–5. One is for Truncus Arteriosus, in which two vessels join to make one. Two is for Transposition of the Great Vessels in which the two great vessels are switched. Three is for Tricuspid Atresia. Remember three for TRIcuspid. Four is for the four defects of Tetralogy of Fallot. Lastly, five is for the five words of Total Anomalous Pulmonary Vascular Return.
The three common acyanotic heart lesions are atrial septal defects, patent ductus arteriosus, and ventricular septal defects. Symptomatic children with such lesions typically present with congestive heart failure by 6 months of life.
Acrocyanosis is a transient blue discoloration of the hands and feet, which can occur when a newborn is cold. Typically, the pulse oximetry reading is normal.
Procedural Emergencies
The emergence reaction from ketamine is the most common adverse effect. The most serious adversereaction is laryngospasm. The laryngospasm can be treated with bag valve mask ventilation. Ketamine can also be used for analgesia in lieu of opiates at a dose of 0.1–0.3 mg/kg.
Renal Emergencies
Hematuria with hearing loss is associated with Alport syndrome. Hematuria and hemoptysis is associated with Goodpasture’s syndrome.
Winter’s formula (pCO2 = 1.5HCO3– + 8 +/-2) is a formula to determine if there is appropriate respiratory compensation in a metabolic acidosis.
MUDPILES mnemonic can be used to remember the causes of an anion gap metabolic acidosis: Methanol, Uremia, DKA, Propylene glycol, Iron or INH, Lactic acidosis, Ethylene glycol, and Salicylates.
The HARDASS mnemonic can be used to remember the causes of a non-anion gap metabolicacidosis: Hyperalimentation, Addison’s disease, RTA, Diarrhea, Acetazolamide, Spironolactone, and Saline infusion.
Pulmonary Emergencies
A ventilation perfusion scan (V/Q) has the highest sensitivity for excluding pulmonary embolism.
With pulmonary embolisms, the most common finding is sinus tachycardia. Do not forget about the classic S1Q3T3 pattern.
The common cause of SVC syndrome is malignancy. The four most common malignancies are bronchogenic carcinoma, small cell lung cancer, squamous cell lung cancer, and lymphoma.
In drowning victims, a 4 to 6 hour observation period is typically sufficient before discharge with normal vitals and a normal exam. Any oxygen requirement or pulmonary finding on exam requires admission.
Hypoxemia can be broken down into five categories: low inspired O2, shunt, diffusion impairment, hypoventilation, and V-Q mismatch.
With right to left shunt, diffusion impairment, and V-Q mismatches, the A-a gradient is increased. With hypoventilation, the A-a gradient is normal.
The hypoxemia of right to left shuntdoes not improve with supplemental O2, but with diffusion impairment, hypoventilation, and V-Q mismatches it would improve.
COPD accounts for 70% of the cases of secondary spontaneous pneumothoraces. Remember that the incidence is also three times greater in men than it is in women.
A BNP of less than 100 essentially rules out heart failure, but an elevated BNP is not necessarily indicative of failure. Obesity can also lead to a spuriously low BNP.
Toxicological Emergencies
Emergent dialysis is required for an acute ingestion with a lithium level greater than 4 mEq/L or for a chronic ingestion with a lithium level greater than 2.5 mEq/L. Emergent dialysis should also be initiated if there are any neurologic findings secondary to the ingestion.
In lithium overdose, there are three classic findings: bradycardia, T wave flattening, and QT prolongation.
Treatment for amphetamine overdoses is mostly supportive. The complex tachydysrhythmias are treated with sodium bicarbonate, agitation is treated with benzodiazepines, and hyperthermia is treated with aggressive cooling measures.
Anticholinergic toxicity can be remembered by the mnemonic: mad as a hatter, blind as a bat, red as a beet, hot as a hare, and dry as a bone. Do not confuse the anticholinergic toxicity with the sympathomimetic toxicity as they are similar, but sympathomimetic overdoses are typically associated with diaphoresis, not dryness.
The cholinergic toxidrome is marked by salivation, lacrimation, urination, defecation, GI upset, and emesis. Remember SLUDGE. The most deadly symptoms can be remembered by the killer b’s: bronchorrhea, bronchospasm, and bradycardia.
A knee X-ray with hyperdense lines at the metaphysis is a classic finding in lead poisoning. Lead poisoning is treated with either succimer or IV EDTA in acute overdoses.
Bupivacaine toxicity is treated with intralipid.
Hydrofluoric acid is treated with calcium gluconate, either topically or intra-arterially.
Benzodiazepine overdoses should be treated with flumazenil but use caution in those who use them chronically as reversal may precipitate seizures.
Iron overdoses occur with ingestions of greater than 40 mg/kg. They should be treated with deferoxamine. For less significant overdoses, GI decontamination may be attempted. Charcoal is of no use here, as it does not bind Iron.
Symptomatic colchicine overdoses must be admitted because of an elevated risk of sudden cardiac death. Other complications include renal failure, rhabdomyolysis, bone marrow suppression, and ARDS.
The Amanita genus of mushrooms can be identified by dots or scales on theircap. They produce the deadly amatoxin.
Amatoxin poisoning has four stages culminating in liver failure and then death. Mortality is commonly cited as 10-30%. Activated charcoal and hemoperfusion can be considered.
Traumatic Emergencies
On bedside ultrasound, the absence of lung sliding is indicative of a pneumothorax. A-lines are horizontal lines that are the normal reflection of the pleura. B-lines are vertical “headlights” that are indicative of pulmonary edema.
A simple pneumothorax is one involving < 10% of the hemithorax and should be treated with a non-rebreather to increase the speed of resorption. With larger pneumothoraces, a chest tube or pigtail catheter will likely be needed.
The NEXUS mnemonic can be remembered by the mnemonic NSAID: Neurologic deficit, Spinal tenderness, Altered mental status, Intoxication, and Distracting injury. The NEXUS and Canadian C-spine rules are tools to rule patients out from the need for imaging in trauma. They both have nearly 100% sensitivity, but very poor specificities and therefore cannot rule in injury.
Myocardial contusions are a sequela of blunt chest trauma. The most common EKG finding is sinus tachycardia. These patients require an echocardiogram. The most common course is spontaneous resorption of resolution of the symptoms. The most serious complication is delayed rupture.
That wraps up part three, the last episode in our brief In-Training Exam review! We hope you enjoyed listening! We will be taking next week off for the ITE but will resume shortly thereafter with new episodes. If you have made it this far in our podcast, you clearly take your studying seriously, and we have no doubt you will do well on the exam!
Good luck, Jeff and Nachi
P.S. In case you missed it, here is the rest of the review: Episode 16 and Episode 17.
Ep 17 Roshcast Emergency Board Review
Feb 16, 2017
Put your heart, mind, and soul into even your smallest acts. This is the secret of success.
–Swami Sivananda
Welcome back to Episode 17! This is part 2 of the 3 part ITE rapid review series. In Episode 16, we covered abdominal emergencies, cardiovascular emergencies, cutaneous emergencies, endocrine emergencies, and environmental emergencies. Today we jump right in with HEENT emergencies. Let’s get started!
HEENT Emergencies
The target pH for eye irrigation after a chemical burn is 7.0–7.2. Alkali burns usually cause more damage than acidic burns due to liquefactive necrosis.
Acute glaucoma classically presents with a red, painful eye, blurry vision, and asymmetric pupils. First line treatment options include beta-blockers, carbonic anhydrase inhibitors, steroids, and miotics.
Corneal abrasions should be treated with topical antibiotics such as erythromycin or ciprofloxacin. Tetanus vaccination should also be updated if needed.
The three most common bacterial causes of acute otitis media are Streptococcus, Haemophilus, and Moraxella. However, viral pathogens are far more common. If treating with antibiotics, the first line is typically amoxicillin.
Hematologic Emergencies
Angioedema secondary to ACE-inhibitor use occurs due to a buildup of bradykinin.
Hereditary angioedema is caused by a deficiency or dysfunction of the C1 esterase inhibitor. Episodes are typically precipitated by stress or trauma. Treatment is with replacement of C1 esterase inhibitor or with FFP if the inhibitor is not available.
TTP is treated with plasmapheresis. If plasmapheresis cannot be performed expediently, FFP can be used as a temporizing measure.
For any patient on warfarin with a life-threatening bleed, FFP, PCC, or recombinant factory VIIa should be given. For a patient on aspirin with a life-threatening bleed, DDAVP should be given in addition to platelets.
Predisposing risk factors for DVT include malignancy, immobilization, recent surgery, obesity, smoking, oral contraceptives, recreational drugs, and hypercoagulable states.
Chronic alcohol abuse leads to a macrocytic anemia and even pancytopenia due to ethanol’s suppressive effects on the bone marrow.
Patients on long-standing isoniazid are at risk for sideroblasticanemia due to a pyridoxine deficiency.
Vitamin B12 deficiency causes a megaloblastic anemia called pernicious anemia. It usually occurs secondary to absorptive problems rather than poor dietary intake.
Giant Cell Arteritis commonly presents with unilateral temporal headache, jaw claudication, tender temporal artery, and even sudden painless monocular vision loss. The ESR is usually between 50-100. 50% of patients with giant cell arteritis also have polymyalgia rheumatica.
Giant cell arteritis should be treated with immediate steroids, long before biopsy confirms the diagnosis.
In giant cell arteritis, aortic involvement can lead to valvular disease and dissection.
Both hemophilia A and Bare x-linked recessive diseases. Hemophilia A is caused by decreased synthesis of factor VIII. Hemophilia B or Christmas disease is caused by decreased synthesis of factor IX. Treatment is with specific factor replacement or if unavailable, with cryoprecipitate.
Immune System Emergencies
For a new mother with mastitis, she should be advised to continue nursing from the affected breast. Dicloxacillin is the antibiotic of choice.
Prophylaxis for Neisseria meningitidis should be offered to high-risk contacts, which includes household members, school contacts in the prior 7 days, and those with direct exposure to patients. The preferred antibiotic regimen for prophylaxis is two days of rifampin. Ceftriaxone and ciprofloxacin can also be used but they are slightly less effective.
Fight bites are at risk for contamination with Eikenella. Amoxicillin-clavulanate is the oral antibiotic of choice. If an IV antibiotic is required, ampicillin-sulbactam, cefoxitin, or piperacillin-tazobactam can be used.
Streptococcus pneumoniae is classically associated with rusty colored sputum, whereas Klebsiella pneumoniae is associated with currant jelly sputum. In alcoholics, Streptococcus pneumoniae is the most common bacterial cause of pneumonia, however the incidence of Klebsiella pneumoniae is higher in this population due to their increased risk of aspiration.
There are three common painless penile lesions. They are caused by Chlamydia, Klebsiella, and Treponema pallidum. Chlamydia causes LGV, which presents as a shallow ulcer. Klebsiella causes granuloma inguinale, which presents as a beefy red ulcer and a painless papule. Treponema pallidum causes syphilis, which presents as a painless chancre.
H. ducreyi causes chancroid, which typically presents with multiple painful papules that ulcerate. HSV causes genital Herpes that tends to present as tender, shallow penile lesions.
Balanitis is typically caused by a candidal infection. The treatment is with topical clotrimazole.
In the modified Centor score, give one point for tonsillar exudates, one point for tender anterior cervical adenopathy, one point for fever by history, one point for the absence of a cough, and one point for age less than 15. For an age over 45, you subtract one point. For a score of 0 or 1 points, treat supportively; for a score of 2 or 3 points, test and treat only if positive; and, lastly, for a score of 4 or 5 points, treatempirically. The mainstay of treatment is amoxicillin.
Herpes simplex virus is the most common infection associated with erythema multiforme. Hepatitis C can also be associated with erythema multiforme, but that usually occurs in the setting of active treatment with telaprevir.
Musculoskeletal Emergencies
A nursemaid’s elbow can be reduced by either supination followed by elbow flexion or with hyperpronation.
NSAIDs are the first-line therapy for gout. Although there is mixed research on this, classically allopurinol is contraindicated during an acute presentation for fear of worsening the attack.
Gout is associated with negatively birefringent crystal on joint aspiration, whereas pseudogout is associated with positively birefringent crystals. Gout typically affects the first metatarsophalangeal joint, whereas pseudogout most commonly affects larger joints like the knees and ankles.
The Hill-Sachs defect is the most common complication of anterior shoulder dislocations, occurring in 40% of cases. The Hill-Sachs defect is a depression fracture of the posterolateral surface of the humeral head. Do not confuse it with a Bankart lesion, which is a fracture of the anterior aspect of the inferior glenoid rim.
The axillary nerve is the most commonly injured nerve in anterior shoulder dislocations. Its function can be tested by arm abduction and sensation over the deltoid muscle.
Nervous System Emergencies
Severe cases of myasthenia gravis can be treated with IVIG or plasma exchange. Although not a cure, symptoms may also be decreased by cooling. The edrophonium test can be used to make the initial diagnosis.
Polycystic kidney disease is associated with an increased incidence of subarachnoid hemorrhages.
Lyme disease is the most common cause of a bilateral Bell’s palsy.
A peripheral facial nerve palsy can be distinguished from a central one by involvement of the forehead.
VP shunt obstruction occurs proximally more frequently than distally. Proximal VP shunt obstruction occurs due to choroid plexus obstruction or increased protein within the CSF. Distal VP shunt obstruction occurs due to abdominal pseudocyst formation, which typically presents with abdominal pain due to the large size of the cyst.
A radial nerve palsy is treated supportively with a wrist splint.
A Marcus Gunn pupil is another term for a pupil with an afferent pupillary defect.
That is it for part two. We have part three ready for release tomorrow. Let us know what you think about this review by emailing us at Roshcast@roshreview.com.
Ep 16 Roshcast Emergency Board Review
Feb 15, 2017
What we think, we become
-Buddha
Welcome back to Episode 16! With the In-training Exam next week, we are doing things a little different this week. Instead of covering new material before the exam, we are launching three episodes, back to back, reviewing the most high-yield points that we have covered so far, organized by topic. We think this extra layer of spaced repetition will help you gain a few extra points during your test. We have set it up in a quiz format, so you can pause the podcast as you go along.
Now onto this week’s podcast
Abdominal Emergencies
Small bowel obstructions are caused most commonly by postoperative adhesions followed by malignancy.
Large bowel obstructions are caused most commonly by malignancy followed by volvulus.
Reynolds’ pentad for acute cholangitis consists of fever, right upper quadrant pain, jaundice, altered mental status, and hypotension.
The initial treatment for GERD should always begin with lifestyle and behavior modifications including weight loss, head of bed elevation, and avoiding eating prior to sleeping. If lifestyle modifications are not providing adequate relief, PPIs are the empiric treatment of choice for GERD.
Untreated GERD can lead to Barrett Esophagus, which increases the risk for esophageal neoplasm.
Cardiovascular Emergencies
Nitrates reduce both the preload and the afterload by dilating vascular smooth muscles. Avoid nitrates in inferior MIs and in those on phosphodiesterase inhibitors.
The most common finding in an acute aortic dissection is hypertension.
Capture beats are normal narrow supraventricular beats within a run of wide complex beats. Fusion beats occur when impulses from two different locations activate the ventricle. One impulse is typically ventricular and the other is supraventricular, resulting in a QRS complex with hybrid morphology of a sinus beat and an intraventricular beat.
For hemodynamically stable patients, AVNRT can be treated with beta-blockers, calcium channel blockers, or, less commonly, digoxin. Unstable or refractory cases require cardioversion.
The mnemonic FROM JANE (Fever, Roth’s spots, Osler’s nodes, Murmur, Janeway lesions, Anemia, Nail-bed hemorrhages, and Emboli), can be used to remember the findings associated with bacterialendocarditis.
In IV drug users with endocarditis, the tricuspid valve is most commonly affected and Staph aureus is the most common bacteria isolated.
In native valve endocarditis, the mitral valve is most commonly infected followed by the aortic valve.
Strep bovis endocarditis is associated with colon cancer (remember: cancer in the colon, bovis in the blood).
In cardiac arrest, AED use, early bystander CPR, amiodarone for shock-resistant ventricular tachycardia or ventricular fibrillation, therapeutic hypothermia, and cardiac catheterization for ventricular dysrhythmias, even in EKGs that do not meet STEMI criteria, have all been shown to improve outcomes.
MAP = CO x SVR + CVP. Its’ more easily estimated by the formula MAP = ⅓SBP + ⅔DBP.
The right coronary artery occlusion supplies the AV node in the majority of patients. Acute occlusion can lead to heart black.
The six P’s of acute arterial occlusion are paresthesias, paralysis, pallor, pulselessness, poikilothermia, and pain out of proportion to exam. Paralysis and paresthesias require emergent surgical intervention.
Acute arterial embolisms should be managed by embolectomy, whereas in situ thromboses may respond to anticoagulation.
Left ventricular thrombus formation after an MI is the most common source of an arterial embolus.
Cutaneous Emergencies
Escharotomies are performed along the medial and lateral aspects of both the upper and lower extremities.
The Parkland formula = 4 x percentage burned x weight (in kg). Give the first half of the fluid over the first 8 hours and the second half of the fluid over the next 16 hours.
Staph scalded skin syndrome is caused by an exotoxin. These patients will have a positive Nikolsky’s sign. Rupturing the bullae will not spread the toxin, as it is spread via the blood stream.
Trousseau’s syndrome is a migratory thrombophlebitis associated with pancreatic cancer.
Erythema nodosum is an inflammatory condition characterized by tender red-violet nodules under the skin. The most common cause is an infection but drugs can also cause erythema nodosum, with OCPs being the most common culprit. The treatment is NSAIDs for mild to moderate cases. Potassium iodine can be used in severe cases.
Endocrine Emergencies
Sulfonylurea anti-hyperglycemia can cause recurrent episodes of hypoglycemia.
In factitious hypoglycemia,C-peptide should be low and insulin levels should be high due to exogenous administration of insulin.
Environmental Emergencies
Scorpion stings cause local redness and edema with a heightened sensitivity to touch in the area. You can also have numbness and weakness in the affected area. Systemic symptoms include fasciculations, disconjugategaze, temperature reversal, and pancreatitis.
Black widow spiders are found throughout the entire United States. They can be identified by the hourglass on their abdomen. In contrast, brown recluse spiders are found in the Midwest.
Black widow spiderbites cause a local papule with a halo. Severe systemic symptoms include a peritoniticabdomen, muscle fasciculations, and diaphoresis. Brown recluse spider bites cause a papule that later blisters and may necrose. Systemic symptoms include renalfailure, pulmonaryedema, and shock
Pit viper snakebites cause local swelling and oozing from the wound. Severe envenomation can lead to a DIC-like coagulopathy and hemorrhagic bullae.
Frostbite should be treated with immersion in a warm water bath at 37 to 39 degrees Celsius. Water at a higher temperature will warm no faster and cause increased pain and potentially tissue damage.
So, that’s it for part 1. Stay tuned for the remaining two parts. Was this review helpful? Do you want us to change anything? Send us your thoughts at roshcast@roshreview.com.
Until next time, Jeff and Nachi
P.S. If you missed Episode 15, including arterial emboli, listen here.
Ep 15 Roshcast Emergency Board Review
Feb 09, 2017
All our dreams can come true — if we have the courage to pursue them.
-Walt Disney
Welcome back to episode 15! As promised, we are back to our weekly episodes leading into the ITE. We start this week with a rapid review of some of the infectious disease high-yield points that we have covered in the past few months, and then we dive right into the new material. Stay tuned for some comical outtakes at the end of the podcast for an inside look at the recording of Roshcast. We think you will enjoy it. Let’s get on with the rapid review.
The most common cause of a painless, clean-based, sharply defined penile ulcer is a chancre, seen in syphilis.
The small shallow ulcer of LGV and the red beefy ulcer of granuloma inguinale are painless also.
Corneal abrasions can be treated with either erythromycin ointment or ciprofloxacin drops. Do not forget to update the tetanus vaccine if indicated.
Native valve endocarditis is seen most commonly in the mitral valve.
The most common cause of pneumonia in alcoholics is Streptococcus pneumoniae.
Now onto this week’s podcast
Question 1
Which of the following is the most common infection associated with erythema multiforme?
A 72-year-old man presents with chest heaviness associated with diaphoresis and shortness of breath. His ECG demonstrates complete heart block. Acute blockage of which of the following coronary arteries is most likely to be causing his dysrhythmia?
A 55-year-old woman presents to the ED for swelling of her tongue and lips. She recently started a new antihypertensive medication. Which of the following is the direct mediator for her condition
A 3-year-old boy presents with stridor. His mother states that he was eating a grape and suddenly started choking. The patient has normal vital signs except for an increased respiratory rate. Physical examination reveals an anxious child who is able to speak, but has stridor. Which of the following management is most likely indicated?
That wraps up episode 15! What do you guys think of the pauses after questions? Let us know by emailing us at Roshcast@roshreview.com. Do not forget to check out the high-yield questions and explanations in the Rosh Review Emergency Medicine Qbank.
Until next time, Jeff and Nachi
P.S. If you missed last week’s episode including frostbite, listen here.
Ep 14 Roshcast Emergency Board Review
Feb 02, 2017
If opportunity doesn’t knock, build a door.
-Milton Berle
Welcome back to Episode 14! After a short break for Jeff’s honeymoon, we are back this week with more high-quality review. We have weekly episodes in the works to keep you motivated. Take note of a small change to the format this week: after each question, you will hear a one-second pause to contemplate the answer or to pause the podcast to give you even more time. We made this change in response to listener feedback; keep more feedback coming to Roshcast@roshreview.com.
We have one more exciting change to announce this week. As you go through the Rosh Review EM question bank and you come across a difficult question or a question you think would be perfect for Roshcasting, hit the “submit feedback” button and type “Roshcast.”
This will prompt the feedback to alert us, and we will work on incorporating the question as quickly as possible. Let’s get started with this week’s episode.
The Hill-Sachs defect (a depression fracture of the posterolateral surface of the humeral head) is the most common complication of an anterior shoulder dislocation. It is seen in about 40% of cases.
Fight bites should be treated with orally with amoxicillin-clavulanate to cover Eikenella If the patient requires IV antibiotics, ampicillin-sulbactam, cefoxitin, or piperacillin-tazobactam can be administered.
Nursemaid’s elbow can be reduced by supination followed by flexion or by hyperpronation. X-rays are not routinely required.
Now onto this week’s podcast
Question 1
Which of the following signs has the greatest likelihood ratio for acute otitis media?
A 4-year-old boy with hemophilia A presents to the ED after he fell from the monkey bars and struck his head on the ground. On exam, he has a large occipital hematoma and a GCS of 14. Which of the following should be administered?
A 22-year-old woman presents with lower abdominal pain and abnormal vaginal discharge for 4 days. She is sexually active with multiple partners and does not consistently use barrier contraception. She has bilateral adnexal tenderness and yellow discharge on pelvic exam. Her urine pregnancy test is negative. In addition to a 1-time dose of ceftriaxone, what is the appropriate outpatient course of antibiotics for the patient?
A 6-year-old boy presents with a fever of 38.5°C, sore throat, and tender anterior cervical adenopathy. He does not have a cough or a runny nose. His younger sister was treated for streptococcal pharyngitis last week and his mother would like him to be treated for streptococcal infection. According to the modified Centor criteria, which of the following is the most appropriate action?
A. Empiric antibiotic treatment for streptococcal pharyngitis
B. Rapid antigen detection testing
C. Streptococcal antibody titers
D. Tonsillectomy when he recovers from this infection
A 48-year-old homeless man is brought in by EMS. He has been walking outside in the snow for many hours wearing only tennis shoes. He is complaining that he is unable to feel his feet. On examination, his feet are cold to the touch, whitish in color, and swollen. He has delayed capillary refill and multiple clear, fluid-filled bullae on his toes. Which of the following is the most appropriate thawing technique?
A. Water immersion at temperatures between 35–36°C
B. Water immersion at temperatures between 37–39°C
C. Water immersion at temperatures between 40–42°C
D. Water immersion at temperatures between 43–45°C
A 19-year-old man with diabetes presents with penile pain and dysuria. Physical examination of the penis reveals the image above. The patient states he has had similar episodes in the past. What management is indicated?
Acute otitis media is most commonly caused viral pathogens. In cases of bacterial infection, Streptococcus, Haemophilus, and Moraxella are the three most common causes. The treatment is amoxicillin.
Hemophilia A is treated with factor VIII replacement and Hemophilia B is treated with factor IX supplementation. Alternatively, cryoprecipitate can also be used in cases of shortages.
PID is typically caused by gonorrhea or chlamydia or both. It is treated with ceftriaxone 250 mg IM once and doxycycline 100 mg PO BID x 14 days if the patient can tolerate PO. Do not confuse PID with the more benign cervicitis, which is treated with ceftriaxone and a single dose of 1 gram of azithromycin.
Fitz-Hugh-Curtis syndrome is aperihepatitisassociated with PID. It is a difficult diagnosis to make, but suspect it in those with both pelvic and right upper quadrant pain.
In the ModifiedCentor Score, you get one point fortonsillar exudates, one point for tender anterior cervical adenopathy, one point fever by history, one point for the absence of cough, and one point for age less than 15years old. For an age over 45, you subtract one point.
In the ModifiedCentor Score, for a score of 0 or 1 points, treat supportively; 2 or 3 points, test and treat if positive; and 4 or 5 points, empirically treat. The mainstay of treatment is amoxicillin.
Frostbite should be treated withimmersion in a warm water bath at 37 to 39 degrees Celsius. Water at higher temperature will warm no faster and cause increased pain and potentially tissue damage.
Ep 13 Roshcast Emergency Board Review
Jan 19, 2017
You must do the things you think you cannot do. -Eleanor Roosevelt
Welcome back to lucky Episode 13! We will start with a cardiology review based on teaching points from prior episodes. Then, we will take you through some new topics from orthopedics to burns.
Hypertension is the most common finding in acute aortic dissection.
Fusion beats are a QRS complex with hybrid morphology of a sinus beat and an intraventricular beat resulting from impulses from two different locations activating the ventricle. One of the impulses is typically ventricular and the other is typically supraventricular.
Nitrate therapy works by reducing both the preload and afterload by dilating veins, coronary arteries, and systemic arteries. It works by relaxing vascular smooth muscles.
There are five cyanotic congenital heart lesions. Remember the 5 T’s and the 1-5 mnemonic: one for truncus arteriosus, two for transposition of the great vessels, three for tricuspid atresia, four for Tetrology of Fallot, and 5 for total anomalous pulmonary vascular return (TAPVR).
Now onto this week’s podcast
Question 1
Which of the following is the most common complication associated with an anterior shoulder dislocation?
A 35-year-old woman presents for evaluation of chest pain. The patient describes a burning pain that begins in the subxiphoid area and radiates up into her neck. Occasionally she has a bitter taste in her mouth. Her electrocardiogram and chest radiograph are normal. Which of the following is most likely to help her symptoms?
You diagnose a 43-year-old patient with alcohol withdrawal. Lab studies reveal a hemoglobin of 8 g/dL and an MCV of 115. Which of the following is the most common cause of these findings
A 36-year-old woman with multiple sclerosis presents with progressive monocular vision loss over the preceding several hours. Which of the following exam findings would be expected?
Which of the following describes a burn that causes pressure and discomfort, extends into the dermis, and may have thick-walled blisters or be leathery white?
A. First-degree burn
B. Second-degree deep partial-thickness burn
C. Second-degree superficial partial-thickness burn
The Hill-Sachs defect is the most common complication of anterior shoulder dislocations, occurring in 40% of cases.
The Hill-Sachs defect is a depression fracture of the posterolateral surface of the humeral head, not to be confused with a Bankart lesion, which is a fracture of the anterior aspect of the inferior glenoid rim.
The axillary nerve function can be tested by arm abduction and sensation over the deltoid muscle.
Initial treatment for GERD should begin with lifestyle and behavior modifications such as weight loss and head of the bed elevation. Empiric medical therapy can be started with a trial of PPIs.
Untreated GERD can lead to Barrett Esophagus, which increases the risk for esophageal neoplasm.
In chronic alcohol abuse, you may see macrocytic anemia and pancytopenia due to the bone marrow suppressive effects of ethanol.
Pyridoxine deficiency leads to a sideroblastic, microcytic anemia. It is seen in children and in patients on isoniazid.
Vitamin B12 deficiency usually occurs secondary to absorptive problems rather than poor dietary intake. Vitamin B12 deficiency causes a megaloblastic anemia and pancytopenia.
The progressive monocular vision loss seen in MS causes an afferent pupillary defect also known as a Marcus Gunn pupil.
Temporal arteritis commonly presents with unilateral temporal headache, jaw claudication, tender temporal artery, sudden painless monocular vision loss, and an ESR between 50–100.
Up to 50% of patients with temporal arteritis have polymyalgia rheumatica.
Temporal arteritis should be treated with immediate steroids, long before biopsy confirms the diagnosis.
In giant cell arteritis, aortic involvement can lead to valvular disease and dissection.
First-degree burnsaffect the epidermis, have a superficial thickness, and are characterized by pain,redness, and mild swelling.
Superficial partial-thickness burnsaffect the papillary region of the dermis. They cause pain, blisters, splotchy skin, and severe swelling.
Deep partial-thickness burns affect the reticular region of the dermis and are white, leathery, and relatively painless.
Full-thickness burns affect the hypodermis and are charred, insensate, and may form eschars.
Fourth-degree burns affect the deeper tissues like the subcutaneous fat, muscles, and bone.
That finishes off lucky Episode 13. We hope you enjoyed this week’s episode. Keep the feedback coming to Roshcast@roshreview.com, so we can tailor this podcast help it fit your learning habits. We will be skipping one week, so Jeff can enjoy his honeymoon!
Until next time, Jeff and Nachi
P.S. If you missed last week’s episode including penile lesions, listen here.
Ep 12 Roshcast Emergency Board Review
Jan 12, 2017
The best preparation for tomorrow is doing your best today. -H. Jackson Brown Jr.
Welcome back to Episode 12! This week we once again continued our theme-based review. We focused on a few high-yield bites and envenomation. This material is easy to gloss over since we do not come across it too often clinically. Not only will this prepare you at the bedside, but it will also help you pick up a few easy points on the In-Training Exam, which, by the way, is right around the corner.
Envenomation by a Portuguese Man O’ War is treated by immediate removal of the nematocyst followed by a salt-water wash.
Black widow spiders have a red hourglass on their abdomen.
Bites from a black widow spider produce a local papule with a halo. Severe symptoms include muscle fasciculations and a peritonitic abdomen.
Brown recluse spider bites cause a papule that blisters and then necroses. Severe symptoms include renal failure, pulmonary edema, and shock.
A pit viper snake envenomation causes local swelling and oozing from the wound. Severe envenomation can cause a DIC-like coagulopathy with hemorrhagic bullae.
Now onto this week’s podcast!
Question 1
A 4-year-old boy is brought to the Emergency Department after a drowning. Bystanders noted the child was underwater for less than a minute. After quickly being pulled up from the bottom of the pool, he coughed and vomited once. He arrived at the ED awake and alert with a GCS 15. On examination, he is afebrile with heart rate 105 beats/minute, respiratory rate 20 breaths/minute, and oxygen saturation 96 % on room air. His lungs are clear to auscultation. What is the next step in management?
A. Admit to telemetry unit for 24-hour observation
B. Discharge home
C. Observe for 4–6 hours and discharge home if there is no change in his clinical status
A 23-year-old man presents with chest pain after a motor vehicle collision. The patient’s chest struck the steering wheel. He has no other complaints or injuries. Chest X-ray is unremarkable. ECG shows sinus tachycardia with anterior ST depressions. A troponin is sent and is positive at 3.50 mg/dl. What management is indicated?
A. Activate the cardiac catheterization laboratory
Which of the following mechanisms of hypoxemia is associated with the failure of arterial oxygen levels to increase in response to supplemental oxygen?
A 19-year-old man presents with an ulcer on his penis. He denies pain, tenderness, and itching of the ulcer. He also denies penile discharge and dysuria. Genital examination reveals a clean-based, sharply defined, circular ulcer on the shaft of his penis. There are no other rashes or lymphadenopathy. Which of the following organisms is the most likely cause of his symptoms?
When caring for a drowning victim with normal vitals and abnormal exam, a 4 to 6 hour observation period is sufficient before discharge. Any oxygen requirement or pulmonary finding on exam requires admission.
Elderly patients with abdominal pain are more likely than younger patients to require an emergent surgical procedure.
The two most common causes of SBOs are adhesions followed by cancer.
Large bowel obstructions are caused most commonly by cancer followed by volvulus.
Mean arterial pressure is defined as Cardiac Output x Systemic Vascular Resistance + Central Venous Pressure. It is often approximated by two-thirds of the diastolic blood pressure plus one-third of the systolic pressure.
Myocardial contusions are a sequela of blunt chest trauma. The most common EKG finding is sinus tachycardia. These patients require an echocardiogram. The most common course is spontaneous resorption of resolution of the symptoms. The most serious complication is delayed rupture.
The hypoxemia of right-to-left shunt would not improve substantially with supplemental oxygen and the A-a gradient would be increased.
Diffusion impairment occurs as a result of interstitial disease which improves with supplemental O2 and has a large A-a gradient
Hypoventilation occurs during drug overdoses, CNS lesions, and neuromuscular junction disorders. Hypoxemia in this setting improves with supplemental oxygen, and the A-a gradient is usually normal.
In V-Q mismatches, hypoxemia improves with supplemental oxygen, and there is an increased A-a gradient.
There are three painlesspenile lesions to remember: The small, shallow ulcer ofLGV caused by Chlamydia. The beefy red ulcer and painless papule of Granuloma Inguinale caused by Klebsiella. Lastly the painless chancre of Syphilis caused by Treponema pallidum.
The two painful penile lesions are the multiple painful papules that ulcerate of Chancroid caused by H. ducreyi and the shallow tender painful lesions of Genital Herpes caused by HSV.
Hope you enjoyed this week’s episode. Send us feedback and comments to Roshcast@roshreview.com. Do not forget to check out the high-yield questions and explanations in the Rosh Review Emergency Medicine Qbank.
Until next time, Jeff and Nachi
P.S. If you missed last week’s episode including mushroom toxicity, listen here.
Ep 11 Roshcast Emergency Board Review
Jan 04, 2017
If you set your goals ridiculously high and it’s a failure, you will fail above everyone else’s success. -James Cameron
Welcome back to Episode 11! Hope you all had a fantastic holiday and New Year’s break. With the In-Training Exam (ITE) just a few months away, it is time to kick the studying into high gear!
We changed the brief initial Rapid Review to cover topics from all prior episodes for better spaced repetition. In this episode, we go over important mnemonics. Consider pausing the podcast briefly and quizzing yourself as you are listening. Do not forget to check out the blog for the other episodes as well as a few new Rosh Quizzes. Lastly, learn some tricks from the high-scoring test-taker Ryan Ribeira, MD.
For acute lithium ingestions, a concentration of 4 mEq/L or greater requires emergent dialysis. In chronic lithium ingestions, a level of greater than 2.5 mEq/L requires emergent dialysis. Additionally, any patient with neurologic findings secondary to the ingestion requires treatment.
Lead poisoning is treated with either succimer or IV EDTA. Remember the mnemonic “it sucks to eat lead.”
For wide complex tachydysrhythmia in a patient presenting with an amphetamineoverdose, you should administer sodium bicarbonate. Do not forget to address the agitation with benzodiazepines and the hyperthermia with cooling, which will also help control symptoms.
Now onto this week’s podcast
Question 1
An 88-year-old man with Parkinson’s disease presents confused. He is using a rivastigmine patch as part of his therapy but has mistakenly put on five patches. What physical examination finding would you expect to see in this patient?
Which of the following is true in the post-cardiac arrest patient who experiences a return of spontaneous circulation (ROSC)?
A. Antiplatelet and anticoagulant therapy should be avoided in post-arrest patients
B. Post arrest angioplasty or stenting of acute coronary lesions with a normal ECG has been shown to be an independent predictor of survival after cardiac arrest
C. Post arrest prophylactic antiarrhythmic therapy has been shown to reduce adverse events
D. There is no proven benefit to therapeutic hypothermia
Question 5
A mother delivered a full-term boy in the ED about 30 minutes ago. On exam, he has cyanosis of the distal extremities, as seen above. His mucous membranes and trunk are pink, and he has +2 distal pulses. No murmurs are heard. His remaining physical exam was normal. Which of the following is most likely his pulse oximetry reading?
A 53-year-old man presents to the emergency department with vomiting, diarrhea, and abdominal cramping which occurred 1 hour after eating a meal prepared from mushrooms he found growing in the forest. Which of the following most predicts a benign course of disease?
A. Absence of neurologic symptoms
B. Dots or scales on the cap of the mushroom
C. Normal serum liver function tests on initial presentation
In a metabolic acidosis, you can use Winters’ Formula, which dictates that the pCO2 should be 1.5 times the bicarbonate +8 +/- 2 for appropriate respiratory compensation.
The mnemonic MUDPILEScan be used to remember many of the common causes of anion gap metabolic acidosis: Methanol, Uremia, DKA, Propylene glycol, Iron or INH, Lactic acidosis, Ethylene glycol, and Salicylates.
For the causes of non-anion gap metabolic acidosis remember HARDASS: Hyperalimentation, Addison’s disease, RTA, Diarrhea, Acetazolamide, Spironolactones, and Saline infusion.
In cardiac arrest, Automated External Defibrillator (AED) use, early bystander CPR, Amiodarone in shock-resistant ventricular tachycardia or ventricular fibrillation, and therapeutic hypothermia are all proven interventions to improve outcomes.
Acrocyanosisis a transient blue discoloration of the hands and feet, which can occur when a newborn is cold. Typically the pulse oximetry reading is normal.
Amanita mushrooms produce a deadly renal and hepatic toxin: the amatoxin.
Amatoxin poisoning leads to 4 stages of symptoms culminating in liver failure. Mortality is commonly cited as 10-30%. Activated charcoal and hemoperfusion can be considered.
TheAmanita genus of mushrooms can be identified by dots or scales on their cap.
From Post-ROSC cardiac care to toxic mushroom ingestion, this concludes episode 11. Let us know how to make this even better by sending Please send feedback to Roshcast@roshreview.com — we want to hear your feedback to keep improving this podcast. Do not forget to check out the high-yield questions and explanations in the Rosh Review Emergency Medicine Qbank.
Until next time, Jeff and Nachi
P.S. If you missed last week’s episode on spider bites, you can catch up here:
Ep 10 Roshcast Emergency Board Review
Dec 20, 2016
Fear is the great extinguisher of dreams… Conversely, it can be your best mentor and source of motivation. –Paula Amato
Welcome back to episode 10! This week we review some key ophthalmologic findings with excellent teaching images for you to see. We also hit the lung, the joints, the extremities, and even spend time on scorpions, snakes, and spiders.
We begin each episode with a rapid review of the previous week’s highlights then dive into the Q&A and wrap up with another rapid review of the covered content. Let’s get started.
The most common cause of pneumonia in an alcoholic is Streptococcus pneumoniae.
Radial nerve palsy is a peripheral nerve lesion caused by compression of the radial nerve in the axilla. The most common findings are wrist drop and hand numbness over the first to third digits. It is managed conservatively with a wrist splint.
IV drug abusers are at risk for tricuspid endocarditis. The most commonly implicated organism is staph aureus.
Colchicine overdoses cause severe GI distress, bone marrow suppression, rhabdomyolysis, renal failure, metabolic acidosis, and even ARDS.
The mainstay of treatment for herpes zoster is pain control. Acyclovir may be prescribed within the first 72 hours of onset of the lesions.
Now onto this week’s podcast
Question 1
A 43-year-old man is currently undergoing palliative radiation therapy for pancreatic cancer. He presents to the emergency department with a 4-day history of gradually worsening left lower extremity pain. Pain is localized to the calf and made worse with ambulation. Exam shows mild edema of the left calf without erythema or warmth. Which of the following is the most likely diagnosis?
A 25-year-old man presents to the ED with right eye pain, tearing, and photophobia. After instilling fluorescein into the affected eye, you see the above on slit lamp exam. Which of the following is the most likely prognosis of this condition?
A 52-year-old man presents with a red right eye that is associated with severe pain and blurred vision. On exam, there is some cloudiness to the cornea. Pupils are 5 mm OD and 3 mm OS. Which of the following is the most likely diagnosis?
What is the most common symptom seen in acute bronchitis?
A. Chest pain
B. Cough
C. Fever
D. Sputum
DVTs typically present with non-specific symptoms including unilateral limb swelling, pain, redness, warm, or even distended collateral veins.
Predisposing risk factors for DVT include malignancy, immobilization, recent surgery, obesity, smoking, oral contraceptives, recreational drugs, and hypercoagulable states.
Corneal abrasions typically resolve within 24-72 hours. They are most commonly caused by ocular trauma or an ocular foreign body. Corneal abrasions are treated with a topical antibiotic such as erythromycin or ciprofloxacin. Tetanus vaccination should be given to patients who are not up to date.
Allopurinol is contraindicated in an acute presentation of gout. The first-line therapy is NSAIDs.
Acute glaucomaoften classical presents as a red, painful eye with blurry vision and asymmetric pupils.
Acute angle-closure glaucoma is caused by closure of the anterior chamber. Treatment should begin with topical beta-blockers, carbonic anhydrase inhibitors, steroids, and miotics.
Scorpion stings produce local redness and edema with a heightened sensitivity to touch in the area of the sting with numbness and weakness of the affected area. Systemic symptoms include fasciculations, disconjugate gaze, temperature reversal, and pancreatitis.
Black widow spider bites cause a local papule with a halo. Severe systemic symptoms include a peritonitic abdomen, muscle fasciculation’s, and diaphoresis. Black widow spiders have a red hourglass on their abdomen and can be found throughout the entire United States.
Brown recluse spidersare found in the Midwest. They cause a papule that later blisters and may necrose. Systemic symptoms include renal failure, pulmonary edema, and shock.
Pit viper snakebites cause local swelling and oozing from the wound. Severe envenomations can lead to a DIC-like coagulopathy and hemorrhagic bullae.
The most common symptom of acute bronchitis is a cough. The most common cause is a viral illness that should be treated with supportive care.
Need to beef up on your colchicine toxicity knowledge? Check out last week’s episode
Don’t forget that the high-yield questions, explanations, and images can be found in the Rosh Review Emergency Medicine Qbank. We will be taking some time off over the holidays, but be ready to go with us in 2017, since the in-service exam will only be a few weeks away.
Happy Holidays from the Roshcast team as well as everybody from Rosh Review!
We’re sitting on a train oblivious to the fact that it’s moving at 80 miles per hour, but anyone sitting outside the train watches it whiz right by! This is the value of learning to see the world through the eyes of others. -Andy Grove
Welcome back to episode 9! This week we review many high yield associations such as organisms and valvular endocarditis. The episodes are short and sweet, so you can even listen twice! We will start this week’s episode off with a Rapid Review of the previous week’s highlights. Be sure to listen to last week’s episode if you missed it.
Hematuria without RBCs on urine microscopy would be seen in rhabdomyolysis
Hematuria and hearing loss is associated with Alport syndrome.
Hematuria with hemoptysis is associated with Goodpasture syndrome.
Be cognizant of the increased incidence of hematuria caused by schistosomiasis in recent immigrants to the United States.
VP shunt obstruction occurs more frequently proximally than distally due to either choroid plexus obstruction or increased protein within the CSF.
Eikenella is a common contaminant of fight bites. Treatment is typically with amoxicillin-clavulanate.
Now onto this week’s podcast
Question 1
A 45-year-old man, with a long history of alcohol abuse, presents to the ED complaining of fever and cough for three days. Which of the following organisms is the most common cause of pneumonia in this population?
A 45-year-old man with a history of alcohol abuse presents with numbness and weakness of the left hand. He states he slept on a bench last night and awoke this morning with the symptoms. Physical examination reveals decreased sensation over the first, second, and third digits and a wrist drop. What management is indicated?
A 75-year-old man with dementia presents to the ED with severe vomiting and diarrhea. He is admitted to the hospital for renal failure and dehydration. An infectious workup is initiated because he has a leukocytosis. The following day, he develops pancytopenia, renal failure, and acute respiratory distress syndrome. He is transferred to the intensive care unit where he has a cardiac arrest and expires. When the family arrives, they report the patient was in his usual state of health until three days ago, when he suffered a gout flare and began to take excessive amounts of a new medication to control the pain. Ingestion of what medication could account for this patient’s presentation and clinical course?
The mnemonic FROM JANE can be used to help remember many of the findings associated with bacterial endocarditis. Fever, Roth spots, Osler nodes, Murmur, Janeway lesions, Anemia, Nail-bed hemorrhages, Emboli.
Absence of lung slidingis indicative of a pneumothorax. A lines are horizontal lines that are the normal reflection of the pleura. B lines are vertical “headlights” that are indicative of pulmonary edema.
Hope you enjoyed this week’s episode. Let us know how to make this better by sending feedback to Roshcast@roshreview.com.
Here is last week’s emergency medicine board review podcast where Jeff and review fight bites, VP shunts, cyanotic heart lesions, hemolytic uremic syndrome, and much more
In the end the great truth will have been learned, that the quest is greater than what is sought, the effort finer than the prize, or rather that the effort is the prize, the victory cheap and hollow were it not for the rigor of the game.
-Justice Benjamin Cardozo
Welcome back to episode 8! With Thanksgiving behind us, let’s keep up the momentum, as the In-Training Exam is right around the corner. Here is a sneak peek into the category breakdown established by ABEM for the ITE.
Roshcast episodes are 10–15 minutes long so you can focus on a few topics at a time without feeling overwhelmed. The short duration of each episode also allows you to go back and review episodes you may have missed or want to reinforce.
We begin each episode with a quick Rapid Review of the previous week’s highlights.
Rh immunoglobulin administration can be delayed up to 72 hours. The correct dose is 50 mcg for those less than 12 weeks gestation and 300 mcg for those 12 weeks and over.
Haloperidol and other typical antipsychotics can cause a dystonic reaction. The treatment is either benztropine or diphenhydramine. 50% of reactions occurring within 48 hours of administration and 90% occur within 5 days.
The target pH for eye irrigation should be between 7.0–7.2, but do not delay irrigation to confirm a staring pH.
Sulfonylureas commonly cause recurrent hypoglycemia as they stimulate the islet beta cells to secrete more insulin, increase the sensitivity of peripheral tissues to insulin, and have a prolonged half-life.
Now to this week’s podcast
Question 1
Which of the following patients requires emergent consultation with an orthopedic specialist?
A. A 36-year-old woman with a femur fracture and distal cyanosis
B. 58-year-old man with extension-based chronic low back pain and leg numbness
C. 75-year-old ambulatory woman with a tibial osteosarcoma
D. An 18-year-old man with a reduced sacral ala fracture and BP 130/86
Question 2
A 12-year-old boy presents to the ED with headache, vomiting, and lethargy for two days. He had a ventriculoperitoneal shunt placed for hydrocephalus one year ago. What is the most likely cause of his shunt malfunction?
A 25-year-old man presents to the emergency department after being in an altercation at a music concert. On exam, you note the findings seen above. Which of the following organisms is of most concern?
Which of these children with hematuria needs admission to the hospital?
A. A 10-year-old boy with recent sore throat treated with amoxicillin, tea-colored urine, and normal urine output; UA shows microscopic hematuria and proteinuria; blood tests are normal
B. A 12-year-old girl with lower abdominal pain, dysuria, urgency, frequency, and pink urine; UA shows microscopic hematuria, > 50 WBCs/hpf, + leukocyte esterase, + nitrites; urine pregnancy test is negative
C. A 6-year-old boy with nausea, vomiting, bloody diarrhea, and decreased urine output; UA shows microscopic hematuria and hyaline casts; blood tests show a high WBC count, low hemoglobin, and low platelets
D. An 8-year-old girl with diffuse mild edema, tea-colored urine, and normal urine output; UA shows microscopic hematuria and proteinuria; blood tests show a normal WBC count, hemoglobin, and platelets but low protein
A 68-year-old man presents to the ED after a fall down 12 stairs. His only medication is warfarin, which he takes for atrial fibrillation. On physical exam, you note a large parietal scalp hematoma. His noncontrast computed tomography scan of the head is shown above. His INR is 4.5. Which of the following is the most appropriate treatment?
With respect to VP shunt malfunction, slit ventricle syndrome occurs when the ventricles are over drained and they collapse, obstructing the proximal shunt orifice. With the reaccumulation of fluid, the obstruction is relieved. Patients typically present with cyclical symptoms.
In treating patients with fight bites, we are concerned for Eikenellacontamination. In fight bites overlying the metacarpal, a hand surgery consultation is necessary.
In human bites, amoxicillin-clavulanateis typically the first-line antibiotic of choice. For established infections, IV antibiotics such as ampicillin-sulbactam, cefoxitin, or piperacillin-tazobactam may be used.
For a child with mild to moderate edema, with a normal blood pressure and no respiratory symptoms, the child can typically be discharged home with outpatient nephrology follow up. The treatment is typically corticosteroids.
For any patient on warfarin with a life-threatening bleed, FFP, PCC, or recombinant factory, 7a should be given.
For a patient on aspirinwith a life-threatening bleed, DDAVP should be given in addition to platelets.
Until next time, Jeff and Nachi
P.S. If you like Nachi and Jeff’s content, remember to check out Rosh Review’s emergency medicine qbank with thousands of high yield questions, explanations, images, audio, and video teaching files.
I wish to do something great and wonderful, but I must start by doing the little things like they were great and wonderful. -Albert Einstein
Welcome back to another episode of Roshcast. This is Episode 7 and we’ll be talking about Rh immunoglobulin, dystonic reactions, chemical-induced corneal burns, medication-induced hypoglycemia, vaginal candidiasis, ocular trauma, and much more.
Hydrofluoric acid exposure is treated with calcium gluconate (topically or intra-arterially).
Benzodiazepine overdoses can be treated with flumazenil. However, be careful in chronic users so as to no precipitate a withdrawal seizure.
An iron ingestion of greater than 40 mg/kg typically requires chelation. Treatment should be with deferoxamine as charcoal does not bind iron and is therefore of no use.
Trousseau’s sign is associated with pancreatic cancer. It is a migratory thrombophlebitis.
Erythema nodosum is a tender, reddish-violet nodule deep under the skin. They can be caused by infections, typically strep, or drugs, with OCPs being the most commonly implicated drugs.
In a patient with an EBV infection, treatment with either ampicillin or amoxicillin may result in a morbilliform rash.
Please send us feedback so we can continue to make small improvements to the show.
Remember to leave your comments below to any questions you have on the content and our discussion.
Now to this week’s podcast
Question 1
A 22-year old woman presents with vaginal bleeding. She should be approximately 10 weeks pregnant based on a previous ultrasound, which confirmed an intrauterine pregnancy. On today’s bedside ultrasound, no intrauterine pregnancy is visualized. Her blood type is A negative and the father’s blood type is unknown. Which of the following is true regarding the administration of Rh immunoglobulin?
A. A test dose is administered first because of the risk of an anaphylactoid reaction
B. Rh immunoglobulin 300 micrograms is indicated
C. Rh immunoglobulin is not indicated
D. She can delay Rh immunoglobulin for up to 72 hours
A 34-year-old woman presents complaining of dysuria and vaginal itching. Your speculum exam reveals a vaginal vault filled with a thick, curdy white discharge. Which of the following statements is correct regarding this diagnosis?
A. A fishy odor is present when vaginal discharge is mixed with potassium hydroxide
B. Metronidazole is the recommended treatment
C. Multiple petechiae are often seen on the vaginal wall
An 18-year-old softball player is struck in the face with a softball. The CT shows a fracture of the inferior orbital floor. She has numbness over the anteromedial cheek and upper lip. Which of the following nerves is likely to be affected?
Rh immunoglobulin administration can be delayed up to 72 hours. The correct dose is 50 mcg for those less than 12 weeks gestation and 300 mcg for those 12 weeks and over.
Haloperidol and other typical antipsychotics can cause a dystonic reaction. The treatment is either benztropine or diphenhydramine. They can both be given IV or IM, with IV being the preferred route.
A chemical splash to the eye should be immediately treated with high volume irrigation. The eye should be irrigated copiously or to a target pH of 7.0-7.2. Alkali burns typically cause more damage than acidic burns due to their characteristic liquefactive necrosis.
In factitious hypoglycemia, blood work would typically show a low c peptide but high insulin levels due to the exogenous administration of insulin.
Vaginal candidiasis is characterized by a thick, white, odorless vaginal discharge. It is treated with fluconazole or clotrimazole. The pH of the discharge is typically less than 4.5.
A fishy-smelling vaginal odor is classic for bacterial vaginosiswhich is treated with metronidazole. Metronidazole is also the treatment for trichomonas.
“As to diseases, make a habit of two things — to help, or at least, to do no harm.” ― Hippocrates
Welcome back to episode 6! Last week’s episode included a new intro Rapid Review…let us know what you think of it. Should we continue it? Keep sending your thoughts to feedback@roshreview.com. This podcast is fluid, and we are open to making changes that would best suit our listeners’ learning styles.
Let’s get started.
Prophylaxis for Neisseria meningitidis should be offered to household members, school contacts in the prior 7 days, and those with direct exposure to the patient. The preferred antibiotic regimen is rifampin BID for two days.
The most common cause of a bilateral Bell’s palsy is Lyme disease.
The most common cause of maternal mortality during delivery is maternal hemorrhage, which can be caused by uterine atony, genital trauma, retained products, or, DIC.
The most serious adverse reaction to ketamine is laryngospasm, which is treated with bag-valve-mask ventilation. Tthe most common adverse reaction is an emergence reaction.
Now to this week’s podcast.
Question 1
Which of the following antidotes is paired with the correct poisoning?
A 3-year-old girl presents to the ED with altered mental status. She was in her usual state of health until one day prior to presentation when she developed abdominal pain, vomiting, and bloody diarrhea after she was found with a bottle of vitamins from the family’s medicine cabinet. She transiently improved for a few hours then became increasingly lethargic. On arrival, she responds only to painful stimulus. Her blood pressure is 65/40 mm Hg and her heart rate is 160 beats per minute. She appears profoundly dehydrated. Her arterial blood gas demonstrates a metabolic acidosis. What is the most definitive therapy for this patient?
You are the physician for a patient who is diagnosed with pancreatic adenocarcinoma. The oncologist makes a note of a positive Trousseau’s syndrome in the documentation. Which of the following is she referring to?
A 15-year-old G1P0 woman at 23 weeks presents with sharp, left lower quadrant abdominal pain for 1 hour. She has had an ultrasound confirming the presence of a single intrauterine pregnancy. The pain is severe and associated with nausea. Pelvic examination reveals tenderness of the left adnexa. The patient’s urinalysis is unremarkable. What test should be ordered to diagnose the patient?
Which of the following statements is true regarding the diagnosis of Epstein-Barr virus infection?
A. Guillain-Barre syndrome is a possible complication
B. Neutrophilia predominates
C. Splenomegaly occurs in 10% of patients
D. The virus is transmitted via respiratory droplets
Bupivacaine toxicity is treated with intralipid.
Hydrofluoric acid is treated with calcium gluconate, either topically or intra-arterially.
Benzodiazepine overdoses should be treated with flumazenil but use caution in those who use them chronically as reversal may precipitate seizures.
Iron overdoses occur with ingestions of greater than 40 mg/kg. They should be treated with deferoxamine. For less significant overdoses, GI decontamination may be attempted. Charcoal is of no use here, as it does not bind Iron.
The 5 stages of iron toxicity are GI irritation, recovery, shock and metabolic acidosis, fulminant hepatic failure, and bowel obstruction leading to scarring.
Trousseau’s syndrome, a migratory thrombophlebitis, is associated with pancreatic cancer.
Erythema nodosum is an inflammatory condition characterized by tender red-violet nodules under the skin. The most common cause is infection. Drugs can also cause erythema nodosum, with OCPs being the most common culprit.
Erythema nodosum is treated with NSAIDs. Potassium iodine can be used in severe cases.
Ovarian torsion is difficult to diagnose. It is commonly seen in women of childbearing age and more commonly occurs on the right, especially in ovaries with large cysts. Laparoscopy is the only way to definitively rule out the condition.
EBV infection can lead to many neurologic complications such as encephalitis, meningitis, and Guillain-Barre Syndrome.
EBV infection is associated with a profound lymphocytic predominance, with atypicallymphocytes seen on the peripheral smear.
Splenomegaly is a common sequela of EBV infection, so remember to tell athletes to abstain from contact sports for up to 4 weeks after infection.
That concludes episode 6. We’ll keep new episodes coming throughout the holiday season so make sure to set your favorite podcast player to download them automatically. Also, don’t forget to write a short review for Roshcast on iTunes when you have a minute.
If you’d like to start at episode 1 to hear more of our educational pearls, just follow this link back to Roshcast.
“The young physician starts life with 20 drugs for each disease, and the old physician ends life with one drug for 20 diseases.” -Osler
Welcome back to another episode of Roshcast. This week are adding a new level of spaced repetition by doing a brief review of previous week’s key take away points before diving into the new material.
The most common causes of small bowel obstructions are (1) adhesions and then (2) cancer. In comparison, large bowel obstructions are caused most frequently by (1) cancer and then (2) volvulus.
Nursemaid’s elbow is treated by either supination followed by elbow flexion or hyperpronation.
Nitrates reduce both preload and afterload by dilating vascular smooth muscle.
Lithium toxicity can cause bradycardia, t wave flattening and QTc prolongation.
The most common finding in aortic dissection is hypertension.
Let us know how you feel about this feature by sending feedback to feedback@roshreview.com.
And please leave us comments. We want to hear from you.
Let’s get going with the new material from Episode 5.
Question 1
Which of the following requires chemoprophylaxis for meningitis exposure?
A. Breastfeeding mother of an infant with E. coli meningitis
B. Classmates of a 7-year-old with S.pneumoniae meningitis
C. Respiratory therapist for a 10-year-old with H.influenzae meningitis
A 4-year old boy presents with a facial laceration. He has been ill with an upper respiratory infection. Procedural sedation with ketamine is planned for his wound repair. Which of the following is a potential serious adverse reaction?
Which of these statistical terms describes the risk of committing a Type I error?
A. Alpha
B. Beta
C. p value
D. Power
Question 6
A 22-year-old man presents after encountering a Portuguese man-of-war in the ocean. He reports significant stinging to his leg with some paresthesias. Which of the following has been shown to be most effective to neutralize additional nematocysts?
A 33-year-old woman, with chronic persistent asthma, presents with palpitations. Her vital signs are HR 210, BP 118/73, and pulse oxygenation of 97% on room air. An ECG is shown above. Which of the following treatments is contraindicated in the treatment of this patient’s disorder?
A. Beta-blocker
B. Calcium channel blocker
C. Digoxin
D. Synchronized cardioversion
Prophylaxis for Neisseria Meningitidis should be offered to high-risk contacts, including household members, school contacts in the prior 7 days, and those with direct exposure to patients.
The preferred antibiotic regimen for prophylaxis is two days of rifampin. Ceftriaxone and ciprofloxacin may also be used but they are slightly less effective.
The most common cause of a bilateral Bell’s Palsy is Lyme disease.
Peripheral facial nerve palsies can be distinguished from central ones based on involvement of the forehead.
The most common cause of maternal mortality during delivery is maternal hemorrhage.
Maternal hemorrhage can be caused by uterine atony, which is treated with oxytocin or uterine massage. Genital trauma is treated with pressure or ligation. Retained products require removal of the products to control the hemorrhage.
One of the potentially serious adverse reactions to ketamine is laryngospasm, which is treated with bag valve mask ventilation. Always remember to set up your procedural sedations with all of your airway equipment at the bedside just as you would for a planned intubation.
The emergence reaction from ketamine is the most common adverse effect. Ketamine can be given IV or IM and can be used for analgesia in lieu of opiates at a dose of 0.1-0.3 mg/kg.
The statistical term alpha describes a type 1 error: detecting an effect that is not present.
A type 2 error, or beta, is failing to detect an effect that is present.
Nematocyst envenomation is treated by immediate removal of the nematocyst followed by salt-water wash.
In asthmatic with tachydysrhythmias, such as AVNRT, beta-blockers should be avoided.
AVNRT can be treated with beta-blockers, calcium channel blockers, digoxin, or electrical synchronized cardioversion for hemodynamically unstable or refractory cases.
Hope you enjoyed this week’s episode. Let us know what you think about the intro rapid review. Remember, this podcast is meant to maximize your learning, so send us a message, and let us know how to optimize our approach. For those of you listening in real time, do not forget the 2017 Emergency Medicine In-service exam is scheduled for Wednesday, February 22. No better time than now to start churning through the Rosh Review Emergency Medicine Question Bank.
Remember to leave comments. We want to hear from you.
Until next time, Jeff and Nachi
P.S. If you missed our previous episodes they can all be found at Roshcast.
“Live as if you were to die tomorrow. Learn as if you were to live forever.” –Mahatma Gandhi
Welcome back! Despite using randomly generating questions, a lot of the question in this episode involved mnemonics. We also review many core concepts in emergency medicine. Enjoy.
A 55-year-old woman with a history of gallstones presents to the ED with right upper quadrant abdominal pain. Her blood pressure is 98/64 mmHg, heart rate is 110 beats per minute, respiratory rate is 22 breaths per minute, and temperature is 39.8°C. She has scleral icterus and appears jaundiced. She is also mildly confused. She is tender in the RUQ with guarding. What is the most likely diagnosis?
A 5-year-old girl presents to the ED with a rash that started on her face and spread to her neck, axillae, and groin. Mom states that the patient had an upper respiratory infection one week prior. On examination, the patient’s rash is tender to the touch. Which of the following statements regarding the diagnosis of this patient’s condition is correct?
A. Deep layers of the dermis are involved
B. It often leaves the patient disfigured from scarring
C. Mucous membrane involvement is common
D. The disease is caused by an exotoxin-producing bacterium
A 20-year-old woman with a history of depression and previous overdose presents with altered mental status. The patient is disoriented with mumbling speech. Her vitals are: T 101.2°F, HR 122, BP 130/82; RR 16. Physical examination is notable for dilated pupils, dry mucous membranes and flushed skin. On ECG, her QRS interval is 60 ms. Which ingested medication is most likely?
A 3-year-old girl with a past medical history of constipation is brought to the ED for evaluation of a limp and left knee pain. Her physical exam is unremarkable. You obtain the knee radiograph seen above. What do you expect to see on her peripheral blood smear?
Acute cholangitis is defined by Reynolds’ pentad of fever, right upper quadrant tenderness, jaundice, altered mental status, and hypotension
The NEXUS and Canadian C-spine rules are tools to rule patients out from the need for imaging in trauma. They both have nearly 100% sensitivity, but very poor specificities and therefore cannot rule in injury
NEXUS can be remembered by the mnemonic NSAID: neurologic deficit, spinal tenderness, altered mental status, intoxication, and distracting injury
Staph scalded skin syndrome is caused by an exotoxin. It is essentially a severe form of bullous impetigo. These patients have a positive Nikolsky’s sign. Rupturing the bullae will not spread the toxin. It is spread hematogenously.
Subarachnoid hemorrhages cause a sudden onset thunderclap headache. 80% are due to aneurysms. Polycystic kidney disease is associated with an increased incidence of subarachnoid hemorrhage. Approximately 10% of strokes are caused by SAH.
Anticholinergic toxicity can be remembered by the mnemonic: mad as a hatter, blind as a bat, red as a beat, hot as a hare, and dry as a bone. They can be treated with physostigmine. Anticholinergic toxicity can be easily confused for sympathomimetic toxicities. However, sympathomimetic overdoses are typically associated with diaphoresis, not dryness.
A knee X-ray with hyperdense lines at the metaphysis is a classic finding in lead poisoning. Lead poisoning is treated with either succimer or IV EDTA in acute overdoses.
Please provide us feedback at feedback@roshreview.com Hopefully you enjoyed listening to this week’s episode and learned a thing or two as well. Don’t forget to subscribe to Roshcast on your favorite media player (iTunes, downcast, etc.) to ensure you will be the first to know about new episodes as they go up.
 Stay Connected
Stay Connected