Lifetime incidence parameters hover around 1 in 11, presenting with a prominent male sex skew.
Peak demographic manifestation concentrated within the 30–60 age band.
High-yield temporal parameter: 50% recurrence vector within a 5-year post-initial-insult window.
Mineralogical Composition Vectors
Calcium oxalate crystals represent the predominant structural matrix.
Struvite configurations (magnesium ammonium phosphate matrix) account for 1–2% of cohorts.
Struvite stones function explicitly as infection-driven configurations secondary to upper tract proliferation; higher distribution index noted in female cohorts.
Etiological & Modifiable Relational Dynamics
Profound systemic dehydration or low baseline fluid throughput states.
High-sodium diet structures and heavy animal-protein consumption loads.
Positive genetic/familial history variables.
Relative risk modulation: Each variable independently operates to expand baseline risk by a factor of 2x to 3x.
Distinctive behavioral marker: Renal colic pacing/writhing behavior with zero antalgic position availability.
Concomitant autonomic triggers: Nausea and emesis manifest in 50% of acute presentations.
Physical Exam Discordance Metrics
Severe subjective distress contrasted with a characteristically soft, completely non-tender abdominal palpation exam.
CVA tenderness is completely variable and lacks reliable negative predictive value.
Atypical Presentation Classifications
Vague, poorly localized abdominal pain presentations occurring in up to 20% of active cases.
Isolated lower urinary tract irritative signs including acute frequency or severe urgency.
Incidental & Asymptomatic Dynamics
Silent intrarenal or ureteral stones found incidentally.
Longitudinal tracking demonstrates up to 33.3% of initially asymptomatic cohorts convert to fully symptomatic renal colic within a multi-year tracking window.
2. EXCLUSION DIAGNOSES & CRITICAL PATHWAY RED FLAGS
Vascular Mimics: AAA rupture/expansion. This is a mandatory exclusion pathway in elderly cohorts presenting with acute flank or back pain. Physical tracking requires active exploration for an expansile, pulsatile abdominal mass.
Gynecologic Emergencies: Ruptured ectopic pregnancy. Demands universal screening protocols via rapid beta-hCG testing in all female patients of childbearing potential presenting with lower abdominal/pelvic localization.
Infectious Upper Tract Decompensation: Acute uncomplicated pyelonephritis. Differentiated via persistent high spikes, high fevers, systemic shaking chills, and profound pyuria.
Genitourinary Structural Crises: Acute testicular torsion. Mandates a thorough, explicit scrotal/testicular structural exam if the flank pain radiates into the scrotum.
Gastrointestinal and Adnexal Torsional Confounds: Acute appendicitis variants, acute mesenteric/bowel ischemia, and ovarian torsion syndromes.
3. LABORATORY TESTING & PHYSIOLOGIC EVALUATION
Urinalysis Interpretation Nuances
Microscopic or gross hematuria presents in approximately 66% to 90% of acute cases.
Critical Pathological Caveat: Complete absence of hematuria documented in 20% to 33.3% of confirmed, acute obstructing ureteral stones.
Diagnostic rule: A pristine urinalysis with zero red blood cells is entirely insufficient to exclude acute ureterolithiasis.
Urinary pH as a Composition Clue
Consistently low urinary pH parameters (pH < 5.5) point strongly toward a uric acid crystalline composition.
Elevated urinary pH parameters (pH > 7.5) indicate the presence of urease-producing microbial pathogens, pointing toward a struvite infection stone.
Infectious Screening Metrics
Active tracking for marked pyuria, positive leukocyte esterase, and bacterial nitrites to rule out an obstructed, infected upper urinary tract system.
BMP
Immediate quantification of baseline serum creatinine to establish accurate eGFR values.
Targeting detection of post-renal AKI from bilateral obstruction, unilateral obstruction in a single functioning kidney, or severe volume depletion.
CBC
Evaluation for marked leukocytosis.
Physiologic Nuance: Mild-to-moderate white blood cell count elevations frequently represent non-specific stress demargination driven by severe pain and repetitive vomiting.
High-grade white blood cell shifts demand immediate exclusion of systemic bacteremia or an infected, obstructed urinary system.
Adjunctive Lab Pathways
Rapid qualitative urine hCG testing.
Reflex urine culture execution whenever urinalysis metrics display significant inflammatory profiles or clinical suspicion of UTI is high.
Gold standard; diagnostic sensitivity and specificity parameters exceed 95% for stones >2 mm.
Provides precise quantification of stone diameter (mm), exact localization (proximal, mid, or distal ureter), and degree of secondary hydronephrosis.
Excellent structural visualization for detecting or ruling out alternate retroperitoneal, vascular, or intra-abdominal pathologies.
Contrast-Enhanced CT Protocols
Indicated when alternative intra-abdominal surgical pathology is highly suspected over isolated renal colic.
Retains diagnostic capability to identify urinary tract stones >3 mm even within contrast-enhanced phases.
NCCT Structural Architecture Limitations
Standard stone protocol CT scans are executed in a prone position without IV contrast enhancement. It does not opacify the ureteral lumen.
Presents a cumulative radiation exposure penalty when utilized serially across recurrent ED presentations.
POCUS / Radiology Ultrasound
Direct stone visualization capabilities are modest, operating at approximately 50% to 60% sensitivity, and is highly dependent on anatomical positioning at the extreme proximal ureter or the UVJ.
Secondary obstruction tracking: Demonstration of hydronephrosis operates at a high sensitivity of approximately 80%.
POCUS Clinical Utility Metrics
Eliminates ionizing radiation exposure and allows immediate, rapid real-time execution directly at the patient’s bedside.
Confirmation of significant hydronephrosis within a classic clinical presentation yields high post-test probability for stone presence while lowering suspicion for vascular catastrophes like a AAA.
KUB Radiography
Extremely poor overall diagnostic sensitivity, hovering around 57%.
Fails to image radiolucent configurations (pure uric acid matrices) or small stones measuring <5 mm.
Avoided in acute ED diagnostic pathways; selectively considered as a low-radiation tracking step in pediatric cohorts or pregnant populations.
Large-scale multi-center randomized controlled trial assessing POCUS first vs. Radiology US first vs. NCCT first pathways in acute ED cohorts.
Primary Clinical Outcomes
No statistically significant variations in missed high-risk alternative diagnoses (AAA, appendicitis, bowel ischemia, or adnexal torsion rates remained rare at ~0.4%).
No differences noted in serious adverse event rates, subjective pain-control scores, return ED visits, or overall hospitalization frequencies.
Radiation Modulation Impact
An ultrasound-first initial strategy reduced cumulative, downstream radiation exposure by approximately 50%.
Algorithmic Selection Guidelines
Establishes the clinical premise that raw diagnostic sensitivity does not automatically equate to superior clinical utility or better patient outcomes.
An ultrasound-first diagnostic pathway paired with selective escalation to NCCT is safe and indicated for recurrent, young, clinically stable cohorts.
6. IMAGING SELECTION MATRIX
Indications Favoring an Ultrasound-First Approach
Age parameters <35 years to mitigate lifetime cumulative radiation risks.
Confirmed, well-documented history of recurrent nephrolithiasis presenting with identical symptoms to prior events.
Hemodynamic stability paired with reassuring, classic clinical tracking.
Indications Favoring Immediate NCCT Imaging
Advanced age parameters.
First-time presentation with zero history of stone disease.
Atypical clinical presentation or diagnostic uncertainty.
Persistent, unmitigated symptoms refractory to standard ED interventions.
High pre-test probability of immediate surgical or urological decompression.
7. EMERGENCY PHARMACOTHERAPY & COLIC MANAGEMENT
First-Line Analgesic Paradigms
NSAIDs: Specifically Ketorolac (Toradol) titrated at 15–30 mg.
High-Yield Data Marker: Multiple trials confirm IV NSAIDs provide equivalent pain reduction scores to titrated IV opioids in acute renal colic.
Mechanism: Targets localized ureteral smooth muscle spasms and downregulates prostaglandin-mediated hyper-filtration and local tissue inflammation.
NSAID Absolute/Relative Contraindications
Significantly depressed GFR or active acute renal failure states.
Active gastrointestinal hemorrhage risks or history of severe peptic ulcerations.
Third-trimester pregnancy.
Second-Line Analgesic Titration
Intermittent titration of IV opioids (e.g., Morphine) indicated if the NSAID maximum ceiling effect is reached or if explicit contraindications prevent NSAID administration.
Antiemetic Adjuvant Therapy
Concomitant use of Ondansetron (Zofran) to manage reflex nausea and vomit-induced dehydration.
Fluid Resuscitation Realities
Targeted IV fluids to correct explicit volume deficits driven by emesis or reduced oral intake.
Physiologic Caveat: Aggressive, high-volume fluid hydration does not accelerate stone transit speed or improve the spontaneous passage rate.
8. MEDICAL EXPULSIVE THERAPY (MET) CLINICAL PARAMETERS
Pharmacologic Agent
Tamsulosin (Flomax) dosed at 0.4 mg orally once daily for a maximum duration of 28 days.
Target Efficacy Window
Highly specific for distal ureteral stones measuring between 5 mm and 10 mm.
Yields modest improvements in spontaneous clearance rates within this specific size band.
Literature Controversies
A 2015 Lancet randomized controlled trial demonstrated neutral primary endpoints.
Subsequent large-scale meta-analyses and network meta-analyses identify a significant signal for benefit, particularly for combinations.
Stones Measuring <5 mm
MET is generally not indicated or cost-effective.
Spontaneous passage rates are high, making the side effect profile of alpha-blockade unjustifiable.
Side Effect Profile
Orthostatic hypotension, transient dizziness, and retrograde ejaculation.
Obstructed Urinary Tract + Concomitant Infection: Co-existence of an obstructing stone and upper tract infection (fever, systemic chills, pyuria, nitrites, leukocytosis) is a urologic emergency. It carries a high risk for rapid progression to pyonephrosis, perinephric abscess, overwhelming urosepsis, and cardiovascular collapse. Requires emergent urologic consultation for surgical retrograde stent placement or percutaneous nephrostomy tube insertion.
Refractory Symptom Complexes
Intractable pain scores or persistent emesis failing aggressive ED parenteral therapies.
High-Risk Patient Anatomy / Physiology
Solitary functioning kidney or renal transplant anatomy presenting with acute obstruction (high risk for sudden anuric renal failure).
Complete clinical anuria.
High-grade, progressive acute kidney injury (AKI) that fails to stabilize following targeted volume resuscitation.
Acute obstructing ureterolithiasis manifesting within a pregnant patient.
High Structural Stone Burden
Stone diameter >10 mm. Spontaneous resolution is unlikely; needs shockwave lithotripsy, ureteroscopy, or specialized stenting.
Prolonged Structural Symptoms
Documented stone impaction or symptom tracking extending past a 4-week timeline without clear passage.
Pain score controlled with oral medications; tolerating adequate PO oral fluids; stable renal function panel; zero systemic or local signs of infection.
Outpatient Prescribing Packets
Scheduled or high-dose PRN oral NSAIDs plus short-course rescue oral opioids for breakthrough colic episodes.
Tamsulosin 0.4 mg once daily if stone localization is distal and diameter measures 5–10 mm.
Oral anti-emetics for home management.
Discharge Guidance and Counseling
Vigorous oral hydration to maintain constant, high volumetric urine throughput.
Provide a urine strainer to capture the stone matrix for metabolic and chemical composition testing.
Explicit Return Precautions
Instruct the patient to return to the ED for temperature spikes, shaking chills, or unmanageable pain spikes.
Instruct the patient to return for relentless vomiting preventing fluid retention.
Clinical Follow-up Tracking
Ensure structured outpatient urology follow-up within a 1- to 2-week window.
The Hematuria Diagnostic Confound: Up to 33% of patients with a confirmed obstructing stone will exhibit a completely normal urinalysis with zero RBCs. Never drop nephrolithiasis from the differential based on a negative dipstick.
Leukocytosis Interpretation: Severe colic and violent vomiting induce physiological demargination. Treat the overall clinical presentation and temperature curve; do not over-interpret an isolated WBC.
Hydrative Fluid Mechanics: Fluids address dehydration from emesis. Over-hydrating a patient in acute colic does not push the stone out faster and may worsen pain by increasing renal capsular hydrostatic pressure.
The 4-Week Functional Boundary: Ureteral obstruction lasting longer than 4 weeks requires specialized intervention to prevent permanent nephron damage.
Size and Anatomy Rules: A 3 mm stone at the UVJ passes spontaneously in ~90% of cases. An 11 mm stone in the proximal ureter has a <10% clearance rate and requires early urologic involvement.
Definition: Life-threatening hypermetabolic state resulting from decompensated thyrotoxicosis.
Hormonal Profile: Absolute levels of total T₄/T₃ often mirror uncomplicated thyrotoxicosis; storm is driven by rapid rate of rise, increased catecholamine sensitivity, or increased free T₄/T₃ concentrations.
Clinical Presentation:
Hyperpyrexia (e.g., 104.2°F)
Tachycardia/Arrhythmias (e.g., 155 bpm)
Altered Mentation: Agitation, delirium, or psychosis; often the primary differentiator between “storm” and “compensated” hyperthyroidism
Aggressive IV fluids; patients are often profoundly dehydrated
May require 3–5 liters of isotonic crystalloid per 24 hours
Take Home Points
I. Diagnostic Essentials
Clinical Diagnosis: Based on hyperpyrexia, cardiovascular dysfunction, and altered mentation.
Key Differentiator: Altered mentation (agitation, delirium, psychosis) is often the sole finding distinguishing “storm” from “compensated” thyrotoxicosis.
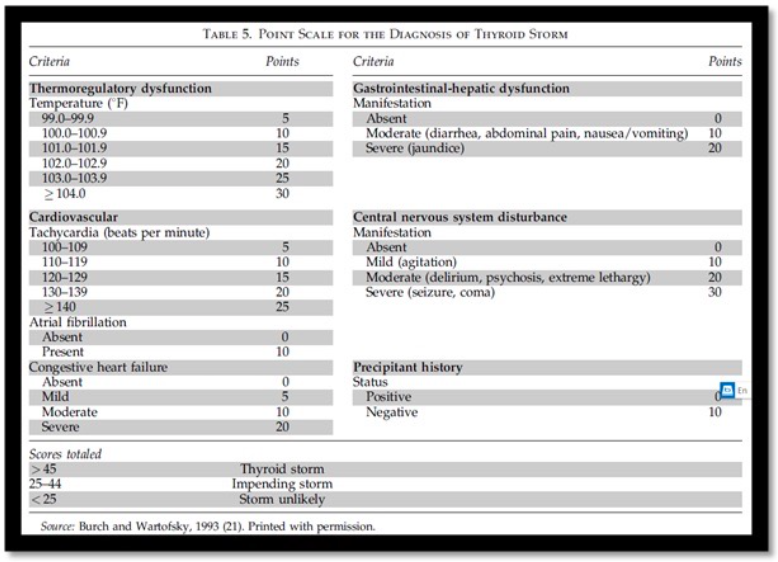
Burch-Wartofsky Point Scale (BWPS):
≥ 45: Highly suggestive of storm.
25–44: Suggests impending storm.
< 25: Storm unlikely.
Note: High sensitivity, low specificity (e.g., hyperthyroid + flu can score > 45).
Triggers: Infection, trauma, parturition, or abrupt cessation of antithyroid drugs.
II. The Four-Step Blocking Strategy
Beta Blockade (Propranolol):
Dose: 60–80 mg PO q4–6h or 0.5–1 mg IV over 10 min.
Action: Blocks symptoms and inhibits peripheral T4 to T3 conversion.
Caution: Avoid in acute decompensated heart failure with systolic dysfunction.
Thionamides (PTU):
Dose: 200 to 250 mg every four hours. (note: some resources suggest a loading dose beforehand)
Action: Preferred over methimazole; blocks new hormone synthesis and peripheral T4 to T3 conversion.
Iodine (SSKI/Lugol’s):
Timing: Must wait ≥ 60 minutes AFTER thionamide dose.
Action: Blocks hormone release.
Pitfall: Early iodine provides substrate for new hormone synthesis, worsening the condition.
Glucocorticoids (Hydrocortisone):
Dose: 300 mg IV load, then 100 mg IV q8h.
Action: Blocks conversion and provides adrenal support.
III. Critical Supportive Care
Hyperpyrexia: Use Acetaminophen.
NEVER Use Aspirin: Displaces thyroid hormone from binding proteins, acutely increasing free T4/T3 levels.
Volume: Aggressive fluid resuscitation; patients may require 3–5 L/day due to profound dehydration.
Definition: Systemic toxicity secondary to local anesthetic (LA) via accidental intravascular injection or excessive systemic absorption.
Threshold: Occurs when plasma concentration exceeds the safety threshold for cardiac and neural tissue.
Agent Profile: Bupivacaine (High Risk)
Highly lipophilic with high protein binding.
“Fast-on, Slow-off” Kinetics: Strong Na+ channel binding with extremely slow dissociation during diastole.
Myocardial Depression: Direct inhibition of Ca2+ release from the sarcoplasmic reticulum, impairing contractility.
Low CC:CNS Ratio: The dose required for cardiac collapse is very close to the dose that triggers seizures (narrow safety margin).
Contributing Factors:
Acidosis/Hypercapnia: Increases the fraction of free drug and promotes ion trapping in the brain/heart; shifts the LA-binding curve toward higher toxicity.
Hypoxemia: Exacerbates myocardial depression and lowers seizure threshold.
II. Risk Assessment & Prevention
Patient-Specific Risk Factors
Extremes of Age: Neonates (low α-1-acid glycoprotein) and elderly (reduced clearance).
Body Composition: Low muscle mass/frailty (decreased volume of distribution).
Organ Dysfunction:
Hepatic: Reduced metabolism of amide LAs.
Renal: Accumulation of metabolites; risk of metabolic acidosis lowering seizure threshold.
Cardiac: Reduced cardiac output slows hepatic delivery/clearance; heart failure patients are more sensitive to Na+ channel blockade.
Pregnancy: Increased sensitivity to cardiotoxicity.
Procedural Risk Factors
Vascularity of Site (Highest to Lowest Risk):
Intercostal blocks (highest absorption rate).
Caudal/Epidural.
Interfascial plane blocks (e.g., TAP block).
Psoas compartment/Sciatic.
Brachial plexus.
Technique: Large volume infiltration, lack of ultrasound, lack of incremental injection.
Prevention Mandates
Weight-Based Dosing:
Lidocaine (Plain): Max 4.5 mg/kg.
Lidocaine (with Epi): Max 7 mg/kg.
Bupivacaine: Max 2.5–3 mg/kg.
Incremental Injection: 3–5 mL aliquots with frequent aspiration.
Intravascular Marker: Use Epinephrine (1:200,000) to detect accidental IV placement (HR increase >10 bpmor SBP increase >15 mmHg).
Unexpected Agitation: In a patient who just received a block, don’t assume “anxiety.”
Wide QRS: Any widening of the QRS complex post-injection is LAST until proven otherwise.
Refractory Arrest: Standard ACLS failing in a patient who received LA. Lipid must be given.
Critical Note: LAST is a clinical diagnosis. Do not wait for serum lidocaine levels or laboratory confirmation to initiate Lipid Emulsion Therapy. Immediate correction of pH and PaCO2 is as vital as the lipid itself.
Maximize your commute with the new Core EM Modular CME Course, featuring the most essential content distilled from our top-rated podcast episodes. This course offers 12 audio-based modules packed with pearls! Information and link below.
Course Highlights:
Credit: 12.5 AMA PRA Category 1 Credits™
Curriculum: Comprehensive coverage of Core Emergency Medicine, with 12 modules spanning from Critical Care to Pediatrics.
Maximize your commute with the new Core EM Modular CME Course, featuring the most essential content distilled from our top-rated podcast episodes. This course offers 12 audio-based modules packed with pearls! Information and link below.
Course Highlights:
Credit: 12.5 AMA PRA Category 1 Credits™
Curriculum: Comprehensive coverage of Core Emergency Medicine, with 12 modules spanning from Critical Care to Pediatrics.
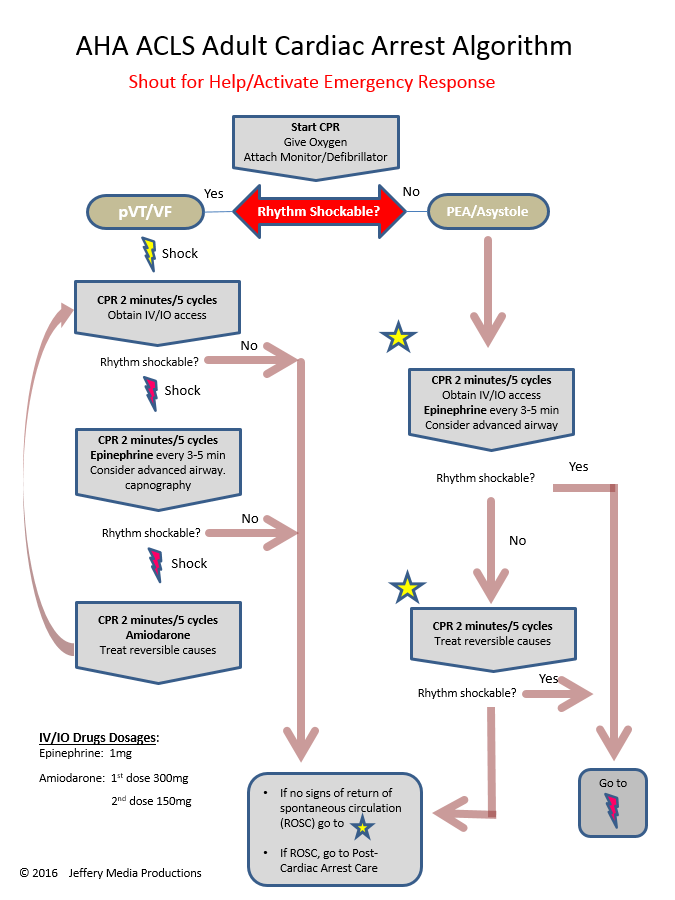
High-Risk Period: Rearrest rates reach 30% within the first minutes post-ROSC.
Shock Incidence: Two-thirds of patients develop profound hypotension/shock as initial resuscitative efforts subside.
Catecholamine Washout: Super-physiologic “code-dose” epinephrine (1mg IV) typically wears off within ~3 minutes post-ROSC, leading to predictable hemodynamic collapse.
Diagnostic Yield: 50% for clinically significant findings (causes or consequences of arrest).
Contrast Risk: Negligible (1–2% increase in AKI risk) compared to the high diagnostic utility.
Avoid Anchoring: Do not assume ischemic EKG changes are the cause; they are frequently a consequence of the global arrest-induced ischemia.
III. Hemodynamic & Respiratory Targets
Mean Arterial Pressure (MAP)
Autoregulation Shift: In acute brain injury/post-arrest, the lower limit of cerebral autoregulation shifts right, often requiring MAPs of 110–120 mmHg for adequate perfusion.
Clinical Target: Aim for MAP >80 mmHg.
The BOX Trial Nuance: While the BOX trial showed no difference between MAP 63 vs. 77, its cohort (Denmark) had exceptionally high survival rates (70% back to work) and short response times, which may not generalize to North American populations with lower shockable rhythm incidence.
Permissive Hypertension: If the patient is “self-driving” to higher pressures, do not aggressively lower them, as this may be a physiologic demand for cerebral blood flow.
Ventilation and Oxygenation
PaCO2 Management:
Target: High-normal to slightly hypercarbic (45–55 mmHg).
Rationale: Avoid accidental hyperventilation (PaCO2 <30), which can cut cerebral blood flow by 50%.
PaO2 Management: Maintain normoxia; avoid extreme hyperoxia, though trial data (BOX trial) suggests small variances (70 vs 90 mmHg) are likely neutral.
IV. Neurological Prognostication & Communication
The “Stunned” Brain
Anoxic Depolarization: Occurs within ~2 minutes of pulselessness as ATP-dependent ion pumps fail.
Clinical Pitfall: Early neurological exams (absent pupils, no motor response) are unreliable in the first hours as they reflect global neuronal “stunning” rather than definitive permanent injury.
Time Horizon: Meaningful recovery is measured in days/weeks, not minutes/hours.
Family Engagement
Presence: Bring family to the bedside immediately, including during procedures or continued resuscitation.
Psychological Impact: Significantly reduces PTSD, anxiety, and depression in survivors’ families.
Prognostic Honesty: Explicitly state “I don’t know” regarding etiology and outcome.
Framing: Define “No News” as the best possible early outcome (preventing rearrest and stabilization).
Maximize your commute with the new Core EM Modular CME Course, featuring the most essential content distilled from our top-rated podcast episodes. This course offers 12 audio-based modules packed with pearls! Information and link below.
Course Highlights:
Credit: 12.5 AMA PRA Category 1 Credits™
Curriculum: Comprehensive coverage of Core Emergency Medicine, with 12 modules spanning from Critical Care to Pediatrics.
Clinical Evolution: Initial assessment noted cachexia and a large ventral hernia. Following initial workup, the patient became acutely altered (A&O x0) and febrile to 102.9°F.
Physical Exam Findings:
Brudzinski Sign: Positive (knees flexed upward upon passive neck flexion).
Kernig Sign: Discussed as highly specific (resistance/pain during knee extension with hip flexed at 90°).
Meningeal Triad: Fever, nuchal rigidity, and AMS (present in 40% of cases; 95% of patients have at least two of the four cardinal symptoms including headache).
Imaging:
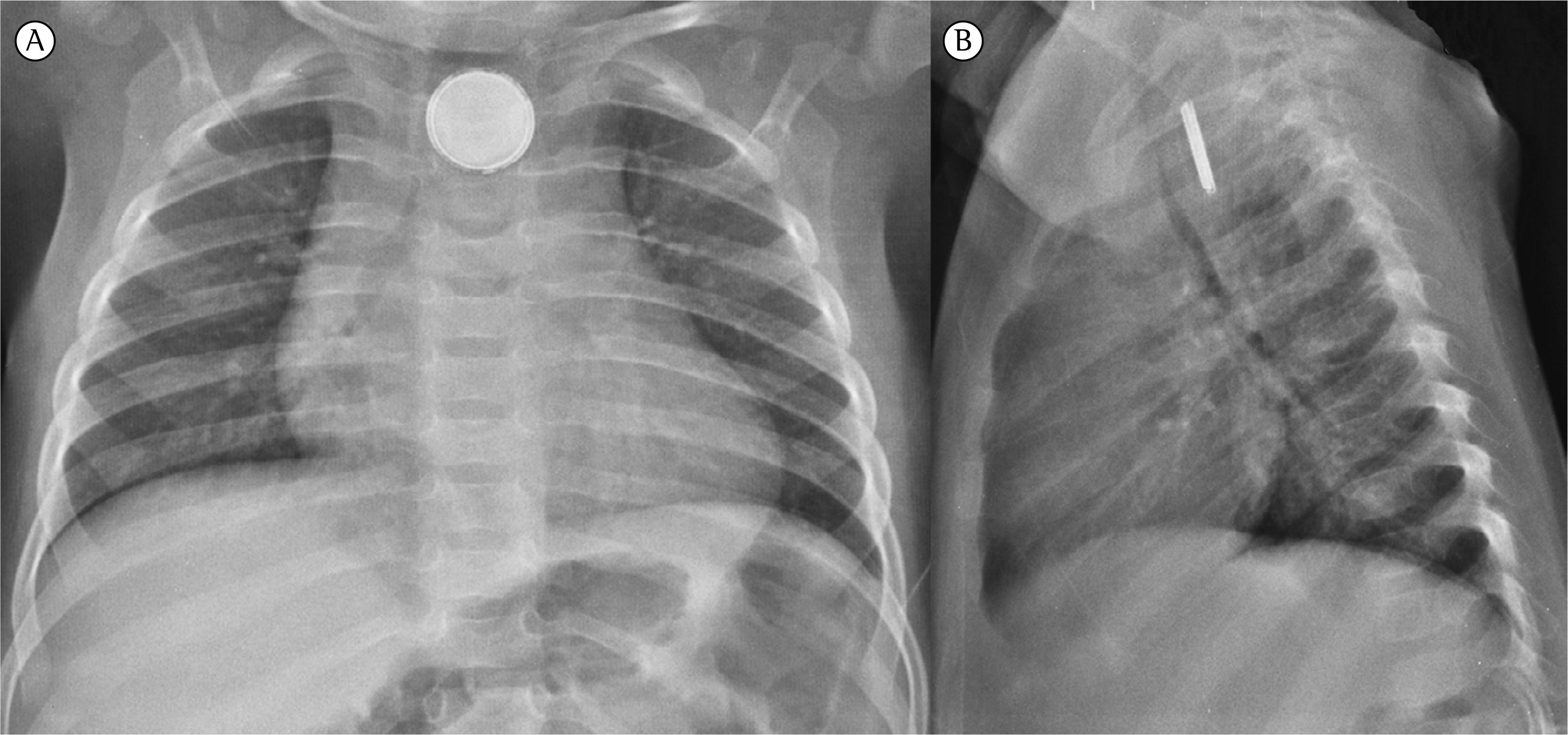
Chest X-ray: Scattered opacities (pneumonia) and a small pneumothorax.
CT Abdomen/Pelvis: Confirmed asplenia (secondary to 2011 GSW/exploratory laparotomy).
Head CT: Ventricle enlargement concerning for obstructive hydrocephalus and diffuse sulcal effacement.
CSF Analysis & Microbiology
Bacterial Meningitis
Opening Pressure: Elevated (Normal is <170 mm H2O).
Color: Cloudy or turbid.
Gram Stain: Positive in 60%–80% of cases before antibiotics; drops to 7%–41% after antibiotics.
Cell Count: Very high (>1000–2000/mm3 WBC); dominated by neutrophils (>80% PMN).
Glucose: Low (<40 mg/dL); CSF/blood glucose ratio is <0.3–0.4.
Maximize your commute with the new Core EM Modular CME Course, featuring the most essential content distilled from our top-rated podcast episodes. This course offers 12 audio-based modules packed with pearls! Information and link below.
Course Highlights:
Credit: 12.5 AMA PRA Category 1 Credits™
Curriculum: Comprehensive coverage of Core Emergency Medicine, with 12 modules spanning from Critical Care to Pediatrics.
Sympathetic Crashing Acute Pulmonary Edema (SCAPE) is characterized by a sudden, massive sympathetic surge leading to intense vasoconstriction and a precipitous rise in afterload.
Pathophysiology: Unlike HFrEF, these patients are often euvolemic or even hypovolemic. The primary issue is fluid maldistribution (fluid shifting from the vasculature into the lungs) due to extreme afterload.
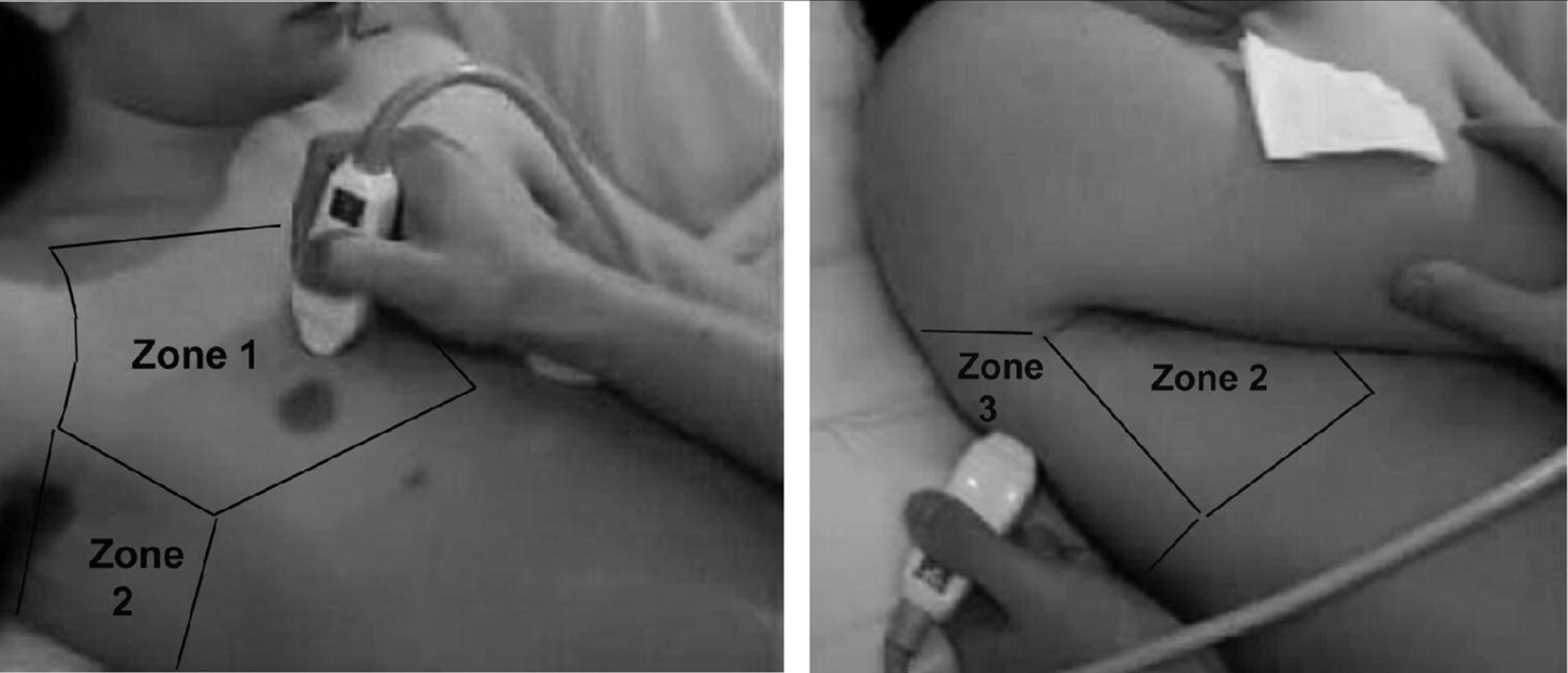
Bedside Diagnosis: POCUS vs. CXR
POCUS is the gold standard for rapid bedside diagnosis.
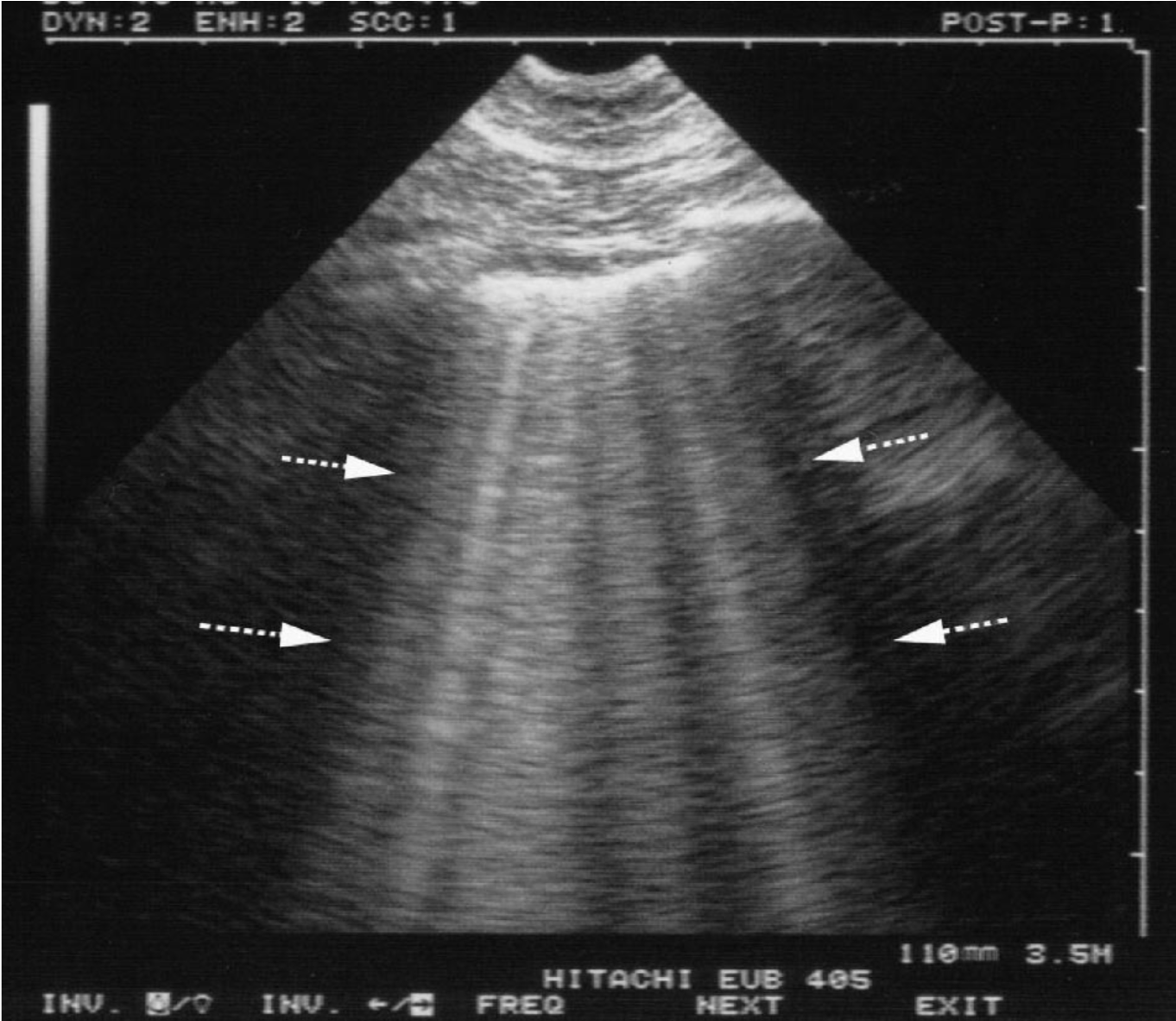
Lung Ultrasound: Look for diffuse B-lines (≥3 in ≥2 bilateral zones).
Cardiac: Assess LV function and check for pericardial effusion.
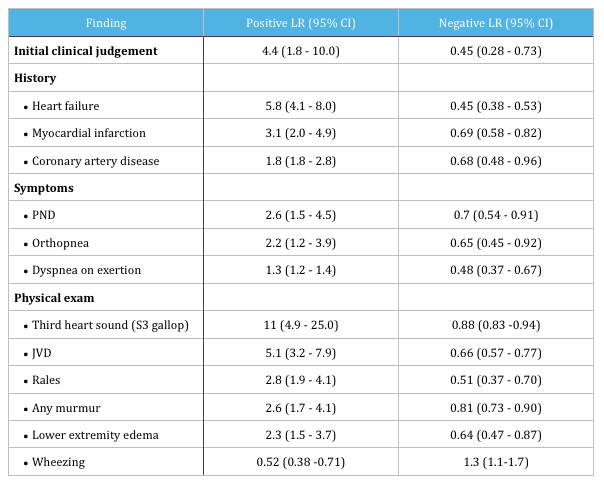
Why not CXR? A meta-analysis shows LUS has a sensitivity of ~88% and specificity of ~90%, whereas CXR sensitivity is only ~73%. Importantly, up to 20% of patients with decompensated HF will have a normal CXR.
Management Strategy
1. NIPPV (CPAP or BiPAP)
Start NIPPV immediately to reduce preload/afterload and recruit alveoli.
Settings: CPAP 5–8 cm H₂O or BiPAP 10/5 cm H₂O. Escalate EPAP quickly but keep pressures to avoid gastric insufflation.
The goal is to drop SBP to < 140–160 mmHg within minutes.
No IV Access: 3–5 SL tabs (0.4 mg each) simultaneously.
IV Bolus: 500–1000 mcg over 2 minutes.
IV Infusion: Start at 100–200 mcg/min; titrate up rapidly (doses > 800 mcg/min may be required).
Safety: ACEP policy supports high-dose NTG as both safe and effective for hypertensive HF. Use a dedicated line/short tubing to prevent adsorption issues.
3. Refractory Hypertension
If SBP remains > 160 mmHg despite NIPPV and aggressive NTG, add a second vasodilator:
Clevidipine: Ultra-short-acting calcium channel blocker (titratable and rapid).
Nicardipine: Effective alternative for rapid BP control.
Enalaprilat: Consider if the above are unavailable.
Troubleshooting & Pitfalls
The “Mask Intolerant” Patient
Hypoxia is the primary driver of agitation. NIPPV is the best sedative. * Pharmacology: If needed, use small doses of benzodiazepines (Midazolam 0.5–1 mg IV).
AVOID Morphine: Data suggests higher rates of adverse events, invasive ventilation, and mortality. A 2022 RCT was halted early due to harm in the morphine arm (43% adverse events vs. 18% with midazolam).
The Role of Diuretics
In SCAPE, diuretics are not first-line.
The problem is redistribution, not volume excess. Diuretics will not help in the first 15–30 minutes and may worsen kidney function in a (relatively) hypovolemic patient.
Delay Diuretics until the patient is stabilized and clear systemic volume overload (edema, weight gain) is confirmed.
Disposition
Admission: Typically requires CCU/ICU for ongoing NIPPV and titration of vasoactive infusions.
Weaning: As BP normalizes and work of breathing improves, infusions and NIPPV can be gradually tapered.
Take-Home Points
Recognize SCAPE: Hyperacute dyspnea + severe HTN. Trust your POCUS (B-lines) over a “clear” CXR.
NIPPV Immediately: Don’t wait. It saves lives and prevents tubes.
High-Dose NTG: Use boluses to “catch up” to the sympathetic surge. Don’t fear the dose.
Avoid Morphine: Use small doses of benzos if the patient is struggling with the mask.
Lasix Later: Prioritize afterload reduction over diuresis in the hyperacute phase.
Maximize your commute with the new Core EM Modular CME Course, featuring the most essential content distilled from our top-rated podcast episodes. This course offers 12 audio-based modules packed with pearls! Information and link below.
Course Highlights:
Credit: 12.5 AMA PRA Category 1 Credits™
Curriculum: Comprehensive coverage of Core Emergency Medicine, with 12 modules spanning from Critical Care to Pediatrics.
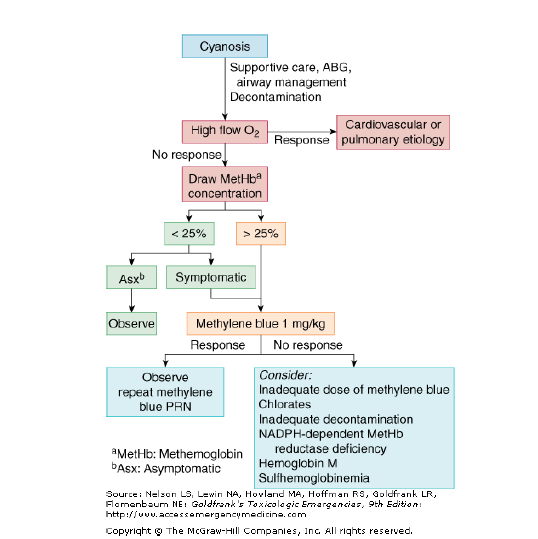
It typically affects infants <1 year of age and is characterized by a sudden, brief, and now resolved episode of one or more of the following:
Cyanosis or pallor
Irregular, absent, or decreased breathing
Marked change in tone (hypertonia or hypotonia)
Altered level of responsiveness
Crucial Caveat: BRUE is a diagnosis of exclusion. If the history and physical exam reveal a specific cause (e.g., reflux, seizure, infection), it is not a BRUE.
Risk Stratification: Low Risk vs. High Risk
Risk stratification is the most important step in management. While only 6-15% of cases meet strict “Low Risk” criteria, identifying these patients allows us to avoid unnecessary invasive testing.
Low Risk Criteria
To be considered Low Risk, the infant must meet ALL of the following:
Age: > 60 days old
Gestational Age: GA > 32 weeks (and Post-Conceptional Age > 45 weeks)
Frequency: This is the first episode
Duration: Lasted < 1 minute
Intervention: No CPR performed by a trained professional
Clinical Picture: Reassuring history and physical exam
Management for Low Risk:
Generally do not require extensive testing or admission.
The Threat: Marburg Virus Disease is from the same family as Ebola and has historically had a reported fatality rate as high as 90%.
The Outbreak (Sept. 2024): Rwanda declared an MVD outbreak. The initial cases involved a miner, his pregnant wife (who fell ill and died after having a baby), and the baby (who also died).
Healthcare Worker Impact: The wife was treated at an epicenter hospital. Eight HCWs were exposed to a nurse who was coding in the ICU; all eight developed symptoms, tested positive within a week, and four of them died.
The Turning Point: The outbreak happened in city referral hospitals where advanced medical interventions (dialysis, mechanical ventilation) were available.
Rapid Therapeutics Access: Within 10 days of identifying Marburg, novel therapies (experimental drugs and monoclonal antibodies) and an experimental vaccine were made available through diplomacy with the US government/CDC and agencies like WHO, Africa CDC, CEPI and more.
The Outcome: This coordinated effort—combining therapeutics, widespread testing, and years of investment in a resilient healthcare system—helped curb the fatality rate down to 23%.
Barriers and Enablers in Outbreak Preparedness
Fragmented Systems: Emergency and surveillance functions often operate in silos, leading to delayed or missed outbreak identification (e.g., inconsistent travel screening at JFK during early COVID-19 vs. African countries).
Solution: Empowering Emergency Departments and the community as the sentinel site can bridge this gap.
Limited Frontline Capacity and Protection: Clinicians are often undertrained and underprotected and are frequently not part of the decision-making for surveillance.
Weak Governance and Accountability: Unclear command structures and lack of feedback discourage early reporting.
Enabler: Strong governance and accountability in Rwanda helped contain the virus.
Dependence on External Programs: Many low-income countries rely on outside sources for vaccines and therapeutics, slowing response.
Solution: Invest in local production (e.g., Rwanda’s pre-outbreak investment in developing its own mRNA vaccines).
Lack of Resource-Smart Innovation: Gaps exist in things like integrating digital triage tools and surveillance systems.
Four Pillars of a Responsive and Equitable Emergency System
Workforce: Invest in pre-service and in-service training, mentorship, and fair compensation to ensure a skilled, protected, and motivated team.
Integration into the Health System: Emergency care (including pre-hospital services) must not operate in silos; it needs to be embedded in national health strategies and linked to surveillance, referral, and financing systems.
Equity in Design and Policy: The system must address the needs and protection of vulnerable groups and work closely with policymakers.
Data: Utilize real-time data and dashboards to provide a feedback loop between clinicians and policymakers, enabling tailored and innovative interventions.
Advice for Clinicians in Global Health Work
Start Small and Build Trust: Meaningful work requires humility and relationship over scale or visibility. Focus on local priorities and sustainable change through long-term partnership, not just presence. Avoid the “savior mindset”.
Be T-Shaped: Be deep in one specialty (e.g., EM) but fluent across other critical areas like policy, finance, and data, as these drive decision-making.
Focus on Knowledge Transfer: True impact means making yourself less essential over time. Prioritize mentorship, co-creation, and sharing leadership opportunities.
Looking Ahead: Global Threats Shaping the Next Decade
The future of EM will be shaped by the convergence of several complex challenges:
Climate and Environmental Crisis: Extreme heat, floods, and vector-borne illnesses will strain emergency systems.
Preparation: Invest in climate-resilient infrastructure for both EDs and the community.
Outbreaks and Biosecurity: Future outbreaks will emerge faster than current systems can handle, coupled with challenges from anti-microbial resistance.
Conflict, Displacement, and Urbanization: Mass migration and overcrowded cities will require new models of emergency care that are mobile, scalable, and inclusive.
Preparation: Building resilient healthcare systems ready for crisis mental health and cross-border coordination.
Digital Tools and AI: These can augment solutions, but investment is needed in data governance and ethical AI that preserves local control and adapts to local capacity.
Definition: Obstruction of pulmonary arteries, usually from a DVT in the proximal lower extremity veins (iliac/femoral), but may be tumor, air, or fat emboli.
Incidence & Mortality: 300,000–370,000 cases/year in the USA, with 60,000–100,000 deaths annually.
Mantra: “Don’t anchor on the obvious. Always risk stratify and resuscitate with precision.”
Risk Factors: Broad, including older age, inherited thrombophilias, malignancy, recent surgery/trauma, travel, smoking, hormonal use, and pregnancy.
Clinical Presentation and Risk Stratification
Presentation: Highly variable, showing up as anything from subtle shortness of breath to collapse.
Acute/Subacute:Dyspnea (most common), pleuritic chest pain, cough, hemoptysis, and syncope. Patients are likely tachycardic, tachypneic, hypoxemic on room air, and may have a low-grade fever.
Chronic: Can mimic acute symptoms or be totally asymptomatic.
Pulmonary Infarction Signs: Pleuritic pain, hemoptysis, and an effusion.
High-Risk Red Flags: Signs of hypotension (systolic blood pressure < 90 mmHg for over 15 minutes), requirement of vasopressors, or signs of shock → activate PERT team immediately.
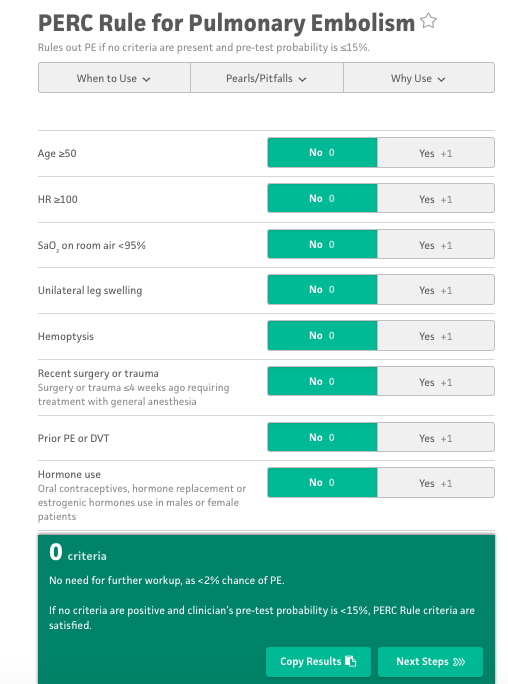
History/Scoring: Ask about prior clots, recent surgeries, hospitalizations, travel. Use Wells/PERC criteria to assess pretest probability.
Labs:
D-dimer: A good test to rule out PE in a patient with low probability. If suspicion is high, proceed directly to imaging.
Troponin/BNP: Act as RV stress gauges. Elevated levels are associated with increased risk of a complicated clinical course (25-40%).
Lactate: Helpful in identifying patients in possible cardiogenic shock.
EKG: Most common finding is sinus tachycardia. Classic RV strain patterns (S1Q3T3, T-wave changes/inversions) are nonspecific.
Imaging:
CXR: Usually normal, but quick and essential to rule out other causes.
CTPA: The usual standard and gold standard for stable patients. High sensitivity (> 95%) and can detect RV enlargement/strain.
V/Q Scan: Option for patients with contraindications to contrast (e.g., severe contrast allergies).
POCUS (Point-of-Care Ultrasound): Useful adjunct for unstable patients.
Bedside Echo: Can show signs of RV strain (enlarged RV, McConnell sign).
Lower Extremity Ultrasound: Can identify a DVT in proximal leg veins.
Treatment & Management
Resuscitation (Reviving the RV):
Oxygenation: Give supplementally as needed (nasal cannula, non-rebreather, high flow).
Intubation:Avoid if possible; positive pressure ventilation can worsen RV dysfunction.
Fluids:Be judicious; even the smallest amount can worsen RV overload.
Vasopressors:Norepinephrine is preferred as first-line for hypotension/shock.
Anticoagulation (Start Immediately):
Initial choice is UFH or LMWH (Lovenox).
Lovenox is preferred for quicker time to therapeutic range, but is contraindicated in renal dysfunction, older age, or need for emergent procedures.
DOACs can be considered for stable, low-risk patients as an outpatient.
Escalation for High-Risk PE
Systemic Thrombolytics: Consider for very sick patients with shock/cardiac arrest (e.g., Alteplase 100 mg over two hours or a bolus in cardiac arrest). High risk of intracranial hemorrhage; weigh risks versus benefits.
PERT Activation: Engage multidisciplinary teams (usually including ICU, CT surgery, and interventional radiology).
Interventions: Consult specialists for catheter-directed thrombolysis or suction embolectomy. Surgical embolectomy can also be considered.
Bridge to Care: Activate the ECMO team early for unstable patients to buy valuable time.
Prognosis & Disposition
Mortality: Low risk < 1%; intermediate 3-15%; high risk 25-65%.
Complications: 3-4% of patients develop Chronic Thromboembolic Pulmonary Hypertension (CTEPH). Others may have long-term RV dysfunction and chronic shortness of breath.
Recurrence: ∼ 30% chance in the next few weeks to months, if not treated correctly.
Disposition:
ICU: All high-risk and some intermediate-high risk patients.
Regular Floor: Intermediate-low risk patients.
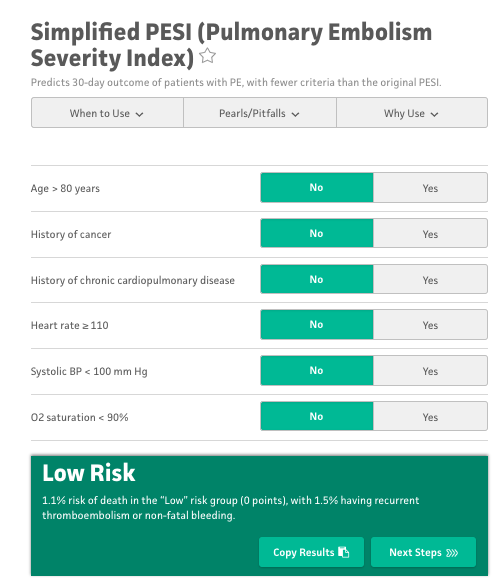
Outpatient Discharge:Low-risk patients can be sent home on anticoagulation. Use PSI or HESTIA scores to risk stratify suitability, typically starting a DOAC.
Shared Decision-Making: Critical to ensure care is safe and consistent with the patient’s wishes.
**Please fill out this quick survey to help us develop additional resources for our listeners: Core EM Survey**
Clinical Evaluation:
Primary Goal: Distinguish benign musculoskeletal pain from serious pathology.
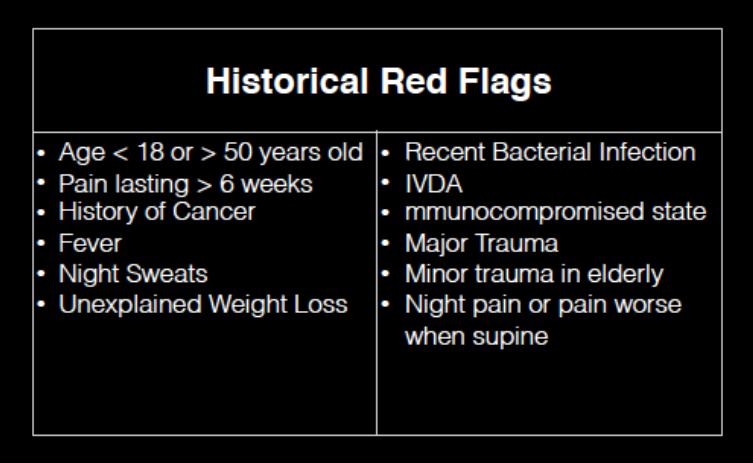
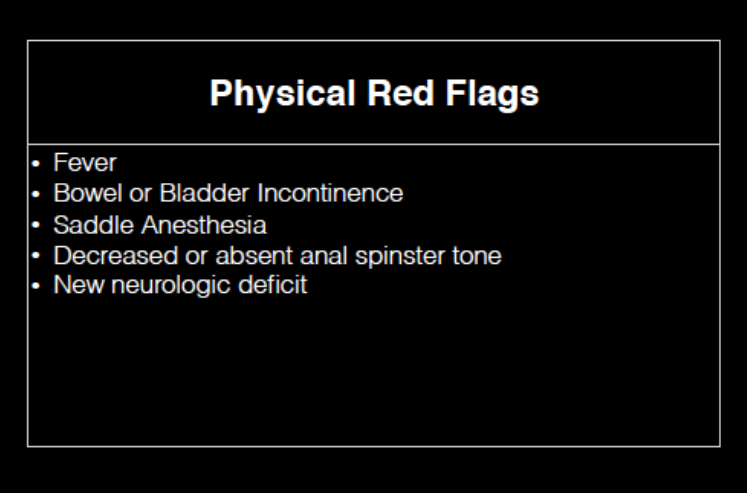
Red Flags: Look for indicators of spinal infection, spinal bleed, or space-occupying lesions (e.g., tumors, large herniated discs).
Assessment: A thorough history and neurological exam (strength testing, gait) is essential.
Additional Tools: Use bedside ultrasound for post-void residual assessment in suspected cauda equina syndrome
Imaging Guidelines:
Routine Imaging: Generally not indicated for young, healthy patients without red flags.
ACEP Recommendations: Avoid lumbar X-rays in patients under 50 without risk factors, as they do not change management and may increase costs and ED time.
Advanced Imaging: Reserve MRI for patients with red flags, neurological deficits, or suspected cauda equina syndrome; CRP may be a part of your calculus when evaluating for infectious causes of back pain
Treatment Options:
Evidence-Based First-Line:
NSAIDs offer modest benefit.
Skeletal muscle relaxants can be used but require caution due to side effects.
Ineffective Therapies:
Acetaminophen shows no benefit for back pain.
Steroids are not recommended for non-radicular pain, with only limited benefit in sciatica.
Topical treatments, lidocaine patches, and opioids are not supported by evidence and may pose additional risks.
Alternative and Experimental Interventions:
Nerve Blocks: Current evidence is limited; more research is needed on trigger point injections and erector spinae plane blocks.
Severe Pain Management:
A single opioid dose (preferably codeine or oral morphine) may be considered to facilitate discharge when necessary.
Use diazepam sparingly for immediate mobilization.
Onsite physical therapy in the ED can be beneficial when available.
Preventing Chronic Pain:
Research Focus: Ongoing studies are evaluating whether duloxetine (Cymbalta) can prevent the transition from acute to chronic back pain.
Non-Pharmacologic Measures: Consider spinal mobilization, physical therapy, acupuncture, and cognitive behavioral therapy (CBT) as adjuncts in management.
Take-Home Points:
Most acute back pain is benign, but watch for red flags like IV drug use, anticoagulation, or neurological symptoms (e.g., weakness, bladder dysfunction) that may indicate serious conditions like spinal infections, bleeds, or cord compression.
Avoid unnecessary lumbar X-rays in young, healthy patients without red flags—MRI is preferred only for those with risk factors, neurological deficits, or suspected cauda equina syndrome.
Use NSAIDs and skeletal muscle relaxants for acute musculoskeletal back pain, as they offer modest benefits. Avoid opioids, acetaminophen, and steroids for non-radicular pain, as they lack evidence.
For severe, uncontrolled pain, consider a single opioid dose (e.g., codeine) or diazepam sparingly
Encourage patients to engage in non-pharmacologic therapies like yoga, massage, or cognitive behavioral therapy to aid recovery and prevent chronic pain.
Historical Context: The conversation around allowing family members in the room during resuscitation events began gaining attention in 1987. Since then, the practice has been increasingly encouraged.
Current Practices in Pediatrics:
Family presence during pediatric resuscitations remains inconsistent, with healthcare provider acceptance ranging from 15% to 85%.
Many subspecialists and consultants still request that families step out, often due to outdated concerns.
Common Concerns & Myths:
Interference in resuscitation → Studies show minimal disruption.
Legal risks → No increased litigation risk has been demonstrated.
Family trauma → Research suggests that presence may help with grieving and reduce PTSD symptoms.
In a randomized controlled trial of 570 relatives, PTSD-related symptoms were significantly higher in family members who were not offered the opportunity to be present during resuscitation.
79% of relatives in the intervention group witnessed CPR compared to 43% in the control group.
Family members who did not witness CPR had a higher likelihood of PTSD symptoms (adjusted OR 1.7, p=0.004).
Anxiety and depression symptoms were also higher in those who did not witness CPR.
Impact on Medical Teams:
The study found no evidence that family presence affected resuscitation success rates, medical team stress levels, or led to legal consequences.
Health professionals’ concerns over interference were largely unfounded.
Guideline Support & Barriers to Implementation
Professional recommendations from pediatric societies support family presence during resuscitations.
Barriers include:
Lack of institutional policies ensuring family inclusion.
Lack of formal training for providers on how to support families during these critical moments.
Final Takeaways
Encouraging institutional policy changes and training providers is key to implementing family presence during codes.
Medical teams should challenge outdated practices and prioritize family-centered care in the emergency department.
Family-witnessed resuscitation does not increase stress, legal risk, or compromise medical care—but it can significantly improve bereavement outcomes.
Use this tool to assess the need for liver transplant evaluation in cases of acetaminophen-induced hepatic failure. Includes criteria for pH, INR, creatinine, and more.
Poison Control Center (available 24/7 for consultation): 1-800-222-1222
References
Goldfrank’s Toxicologic Emergencies, 9th Edition was consulted for information on the pharmacokinetics and clinical presentation of acetaminophen toxicity.
For more details, see: Nelson, L. S., Howland, M. A., Lewin, N. A., Smith, S. W., Goldfrank, L. R., & Hoffman, R. S. (Eds.). (2011). Goldfrank’s toxicologic emergencies (9th ed.). McGraw-Hill Education.
Differentiating between primary headaches (migraine, tension-type, cluster) and secondary causes (e.g., subarachnoid hemorrhage).
The importance of patient history and reevaluation after initial treatment.
Recognizing the unique presentation of cluster headaches and their management implications.
Effective Acute Migraine Treatments:
First-line treatments including anti-dopaminergic medications like metoclopramide (Reglan) and prochlorperazine (Compazine), and parenteral NSAIDs like ketorolac (Toradol).
The limited role of triptans in the ED due to side effects and less efficacy compared to anti-dopaminergics.
The use of nerve blocks (greater occipital nerve block and sphenopalatine ganglion block) as effective treatments without systemic side effects.
Treatments to Avoid or Use with Caution:
Diphenhydramine (Benadryl): Studies show it does not prevent akathisia from anti-dopaminergics nor improve migraine outcomes.
IV Fluids: Routine use is not supported unless the patient shows signs of dehydration.
Magnesium: Conflicting evidence with some studies showing no benefit or even harm.
Managing Refractory Migraines:
Second-line treatments including additional doses of metoclopramide combined with NSAIDs or dihydroergotamine (DHE).
Considering opioids as a last resort when other treatments fail.
The potential use of newer medications like lasmiditan and CGRP antagonists.
Preventing Recurrence of Migraines:
Administering a single dose of dexamethasone (4 mg IV) to reduce the risk of headache recurrence after discharge.
Prescribing NSAIDs or triptans upon discharge for outpatient management.
Recognizing and addressing chronic migraine, and initiating preventive therapies like propranolol when appropriate.
Key Takeaways
Differentiate Primary from Secondary Headaches and Reassess After Treatment:
Use patient history and reevaluation post-treatment to distinguish migraines from more serious conditions, reducing unnecessary imaging and procedures.
First-Line Treatments Are Effective:
Anti-dopaminergic medications and NSAIDs are the mainstay of acute migraine treatment in the ED.
Reserve opioids for cases unresponsive to multiple lines of treatment.
Avoid Unnecessary Interventions:
Diphenhydramine and routine IV fluids do not have proven benefits and can be excluded to streamline care.
Utilize Nerve Blocks for Refractory Cases:
Greater occipital nerve blocks and sphenopalatine ganglion blocks are effective alternatives for patients not responding to medication.
Prevent Recurrence with Dexamethasone and Outpatient Planning:
A single IV dose of dexamethasone can help prevent recurrence.
Provide prescriptions and consider preventive therapies to reduce future ED visits.
ICIs are a relatively new class of oncologic drugs that have revolutionized cancer treatment.
Unlike chemotherapy, ICIs help the immune system develop memory against cancer cells and adapt as the cancer mutates.
Since their release in 2011, ICIs have expanded to 83 indications for 17 different cancers, with approximately 230,000 patients using them.
Mechanism of Action
Cancer cells can evade the immune system by binding to T cell receptors that downregulate the immune response.
ICIs work by blocking these receptors or ligands, preventing the downregulation and allowing T cells to proliferate and attack cancer cells.
Common ICIs
Risks and Toxicities of ICIs
ICIs can lead to autoimmune attacks on healthy cells due to immune system upregulation.
Immune-related adverse effects (irAEs) include colitis, pneumonitis, dermatitis, hepatitis, and endocrine issues (e.g., hypothyroid, hypocortisolemia, hypophysitis).
These toxicities can present as infections, making diagnosis challenging in the emergency room.
Management of ICI Toxicities in the ER
Diagnosis: Look for signs that mimic infections (e.g., cough and fever in pneumonitis).
Diagnostic Imaging in pneumonitis: If CXR is normal but suspicion is high, consider CT scans to differentiate conditions like pneumonitis from other issues such as malignancy-associated pleural effusion or acute pulmonary embolism.
Treatment: The primary treatment for irAEs is steroids (e.g., prednisone 1 mg/kg). Start steroids early and hold the ICI to manage symptoms effectively and increase the likelihood of resuming ICI therapy later.
Consider using antibiotics in combination with steroids if there is uncertainty about whether symptoms are due to infection or ICI toxicity.
Coordinate care with the patient’s oncologist if possible
Disposition Decisions
Patient disposition (admit vs. discharge) should depend on clinical presentation and severity.
Coordination with oncology is crucial; they are often comfortable with starting steroids even if there is a potential infection.
Patients can be discharged if symptoms are mild, but sicker patients with more complex presentations may require admission.
Take-Home Points
ICIs are a new class of cancer drugs that effectively target cancer cells but come with unique immune-related toxicities.
Diagnosing irAEs can be challenging due to symptom overlap with infections.
The cornerstone of treatment is early administration of steroids and temporarily holding the ICI.
Close collaboration with oncology teams is essential for optimal patient management.
The episode focuses on ataxia in children, which can range from self-limiting to life-threatening conditions.
Pediatric emergency medicine specialist shares insights on the topic.
The Case
An 18-month-old boy presented with ataxia, unable to keep his head up, sit, or stand, and began vomiting.
Previously healthy except for recurrent otitis media and viral-induced wheezing.
The decision to take the child to the emergency department (ED) was based on acute symptoms.
Differential Diagnosis
Common causes include acute cerebellar ataxia, drug ingestion, Guillain-Barre syndrome, and basilar migraine.
Less common causes include cerebellitis, encephalitis, brain tumors, and labyrinthitis.
Importance of History and Physical Examination
A detailed history and physical exam are essential in diagnosing ataxia.
Key factors include time course, recent infections, signs of increased intracranial pressure, and toxic exposures.
Look for signs such as bradycardia, hypertension, vomiting, and overall appearance.
Diagnostic Workup
Initial tests include point-of-care glucose and neuroimaging for concerns about trauma or increased intracranial pressure.
MRI is preferred for posterior fossa abnormalities, but non-contrast head CT is commonly used due to accessibility.
Lumbar puncture may be needed if meningismus is present.
Treatment Approach
Treatment depends on the underlying cause:
Acute cerebellar ataxia is self-limiting and typically resolves with time.
Antibiotics are required for meningitis or encephalitis.
Steroids may be useful for cerebellitis and acute disseminated encephalomyelitis (ADEM).
Specialist consultations are necessary for severe diagnoses like intracranial masses.
Outcome of the Case Study
The child had a normal fast T2 MRI and improved during the ED stay.
Diagnosed with a combination of cerebellar ataxia and labyrinthitis.
Received myringotomy tubes and experienced no further neurologic changes or otitis media episodes.
Take-Home Points
Diverse Etiologies: Ataxia in children can have various causes that range from self-limiting to life-threatening
Comprehensive Assessment: History and physical exams guide diagnosis and workup direction, focusing on symptom time course, infections, and toxic exposures.
Physical Examination Clues: Vital signs and appearance offer clues; increased ICP may present with bradycardia, hypertension, and vomiting.
Diagnostic Imaging: Point-of-care glucose testing and neuroimaging are key; MRI is preferred for posterior fossa abnormalities.
Tailored Treatment: Treatment varies by cause; acute cerebellar ataxia typically resolves over time without specific intervention.
Osmotic Diuresis with Renal Water Losses: High glucose, mannitol
Risk Factors:
Patients with impaired thirst response or those unable to access water (e.g., altered or ventilated patients) are at higher risk.
Important to consider underlying conditions affecting thirst mechanisms.
Diagnosis:
Initial assessment includes history, physical examination, and laboratory tests.
Key tests: urine osmolality and urine sodium levels.
Lab errors should be considered if the clinical picture does not match the lab results.
Management Strategies:
Calculate the Free Water Deficit (FWD) to guide treatment.
Administration routes include oral, NGT, G-tube, or IV with D5W for larger deficits.
Safe correction rate is 10-12 mEq/L per day or 0.5 mEq/L per hour to avoid cerebral edema.
Address hypovolemia with isotonic fluids before correcting sodium.
Monitoring and Follow-Up:
Monitor sodium levels every 4-6 hours.
Assess urine output and adjust free water administration as needed.
Admission to ICU for symptomatic patients or those with severe hypernatremia (sodium >160 mEq/L).
Decision to discharge vs admit is a complicated one that factors in symptoms, etiology, degree of hypernatremia, patient preference, access to follow up, etc.
Take Home Points:
Hypernatremia is a serum sodium level over 145 mEq/L, with symptoms ranging from nausea to coma.
It is primarily caused by water loss exceeding intake due to various factors like sweating, vomiting, diarrhea, and renal issues.
Correcting hypernatremia too quickly can lead to cerebral edema, so a safe correction rate is essential.
Initial treatment involves calculating the Free Water Deficit and selecting the appropriate administration route.
Monitor sodium levels frequently and decide on admission or discharge based on symptoms, sodium levels, and patient’s ability to follow up.
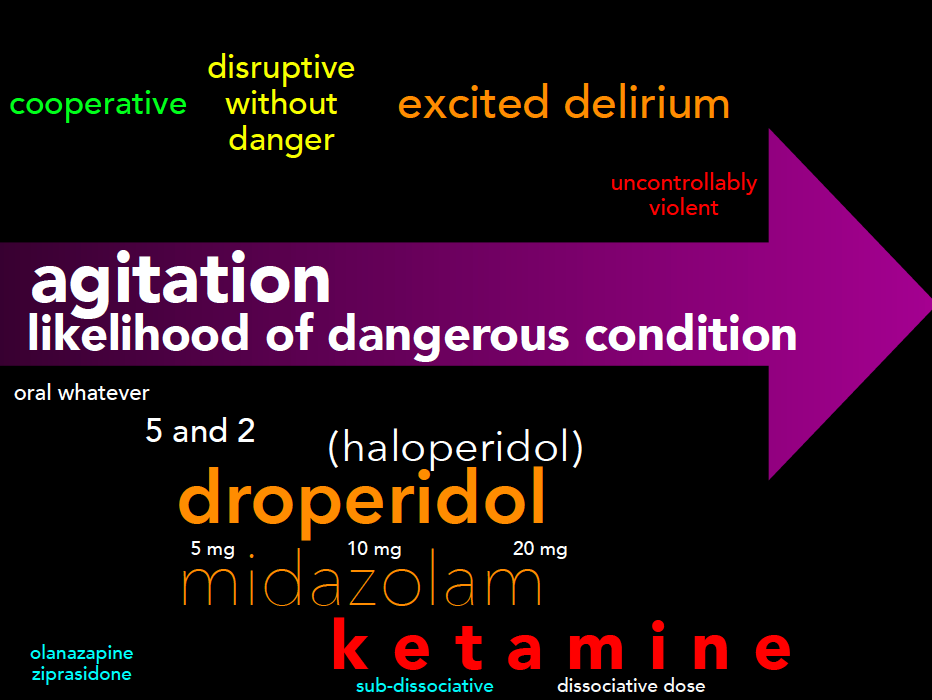
•Definition and Scope: Agitation encompasses behaviors from restlessness to severe altered mental states. It’s a common emergency department presentation, often linked with acute medical or psychiatric emergencies.
•Significance: Patients with agitation are at high risk for morbidity and mortality, necessitating prompt and effective management to prevent harm to themselves and healthcare providers.
A Changing Paradigm in Describing Agitation
•Terminology Shift: Move away from terms like ‘excited delirium’ due to their politicization and stigmatization. Focus on describing agitation by severity and underlying causes.
Agitation as a Multifactorial Process
•Complex Nature: Recognize agitation as a result of various factors, including medical, psychiatric, and environmental influences.
Recognizing Agitation
•Signs and Symptoms: Identify agitation early by monitoring for behaviors such as hostility, pacing, non-compliance, and verbal aggression.
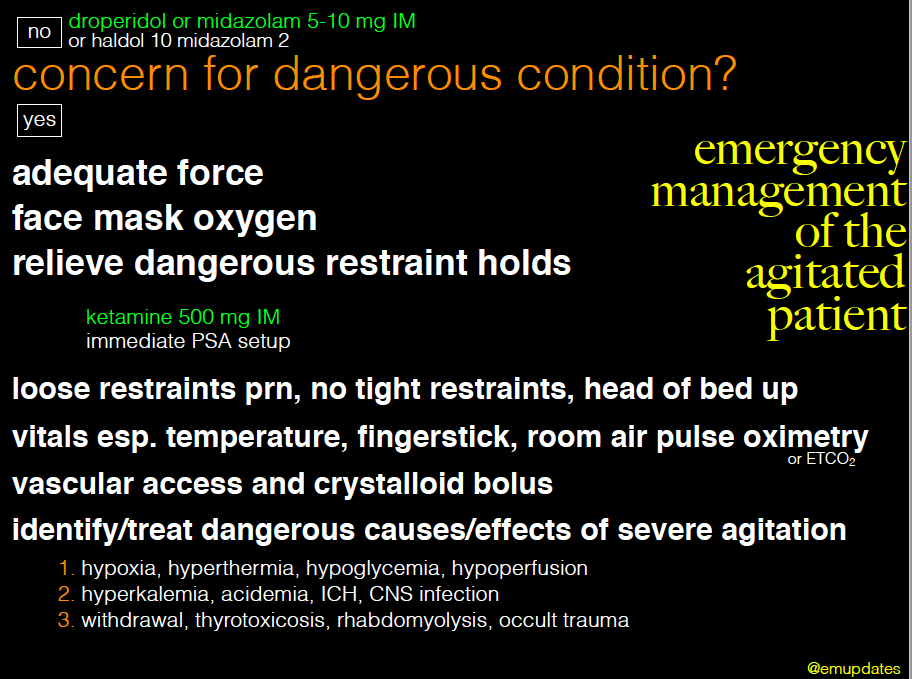
Initial Evaluation
•Severity Assessment: Determine the severity of agitation and prioritize reversible causes and life-threatening conditions.
•Diagnostic Steps: Perform vital signs check, blood glucose levels, ECG, and a targeted medical screening exam.
Life Threats
•Immediate Concerns: Identify and address immediate life threats such as hypoxia, hypoglycemia, trauma, and acute neurological emergencies.
Forming a Differential Prior to Treatment
•Prioritization: Severe agitation requires immediate treatment to facilitate further evaluation and reduce risk of harm.
Physician/Staff Safety
•Safety Measures: Ensure personal and team safety by maintaining a calm environment and preparing for potential violence.
Multimodal Approach
•Self-check In: Physicians should mentally prepare and approach the situation calmly to ensure effective management.
•Verbal De-escalation: Use techniques focused on safety, therapeutic alliance, and patient autonomy to manage agitation non-pharmacologically.
Medication Administration
•Oral/Sublingual Medications: Consider oral medications for less severe cases to maintain patient autonomy and avoid invasive procedures.
•IM or IV Medications: Use intramuscular or intravenous medications for rapid control in severe cases.
Specific Medication Regimens
•PO Regimens:
•Medications: Antipsychotics like Zyprexa (olanzapine) 5-10 mg, benzodiazepines like Ativan (lorazepam) 1-2 mg.
•Benefits: Empower patients with a sense of autonomy, avoid injection-related trauma.
•Pharmacokinetics:
•Olanzapine: Onset in 15-45 minutes, peak effect in 1-2 hours, duration 12-24 hours.
•Lorazepam: Onset in 30-60 minutes, peak effect in 2 hours, duration 6-8 hours.
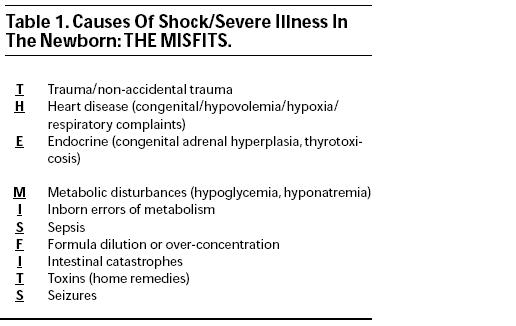
‘T’ in the mnemonic stands for trauma, which includes both accidental and intentional causes.
Considerations for Non-accidental Trauma:
Stresses the importance of considering non-accidental trauma, especially given that it may not always present with obvious external signs.
Anatomical Vulnerabilities:
Highlights specific anatomical considerations for infants who suffer from trauma:
Infants have proportionally larger heads, increasing their susceptibility to high cervical spine (c-spine) injuries.
Their liver and spleen are less protected, making abdominal injuries potentially more severe.
Heart
5 T’s of Cyanotic Congenital Heart Disease: Introduces a mnemonic to help remember key right-sided ductal-dependent lesions:
Truncus Arteriosus: Single vessel serving as both pulmonary and systemic outflow tract.
Transposition of the Great Arteries: The pulmonary artery and aorta are switched, leading to improper circulation.
Tricuspid Atresia: Absence of the tricuspid valve, leading to inadequate development of the right ventricle and pulmonary circulation issues.
Tetralogy of Fallot: Comprises four defects—ventricular septal defect, pulmonary stenosis, right ventricular hypertrophy, and an overriding aorta.
Total Anomalous Pulmonary Venous Connection (TAPVC): Pulmonary veins do not connect to the left atrium but rather to the right heart or veins, causing oxygen-rich blood to mix with oxygen-poor blood.
Other Significant Conditions:
Ebstein’s Anomaly: Malformation of the tricuspid valve affecting right-sided heart function.
Pulmonary Atresia/Stenosis: Incomplete formation or narrowing of the pulmonary valve obstructs blood flow to the lungs.
Left-sided Ductal-Dependent Lesions:
Conditions such as aortic arch abnormalities (coarctation or interrupted arch), critical aortic stenosis, and hypoplastic left heart syndrome are highlighted. These generally present with less obvious cyanosis and more pallor.
Diagnostic and Management Considerations:
Routine prenatal ultrasounds detect most cases, but conditions like coarctation of the aorta and TAPVC might not be apparent until after birth when the ductus arteriosus closes.
Emphasizes the importance of a thorough physical exam: checking for murmurs, assessing hepatosplenomegaly, feeling for femoral pulses, measuring pre- and post-ductal saturations, and taking blood pressures in all four limbs.
Treatment Recommendations:
Early initiation of alprostadil (a prostaglandin) for patients with suspected ductal-dependent lesions to maintain ductal patency.
Preparedness for potential complications from alprostadil treatment, such as apnea and hypotension, which may necessitate intubation and hemodynamic support.
Endocrine
Focuses on acute salt-wasting crisis in undiagnosed Congenital Adrenal Hyperplasia (CAH).
Electrolyte imbalances: ↓Na, ↑K, ↓HCO3, ↓Glu.
Treatment: hydrocortisone (25mg for babies, 50mg for kids, 100mg for adults).
Metabolic
Electrolyte abnormalities such as hypoglycemia (values: <60 in infants, <40 in neonates).
Broad differential.
Rule of 50s for correction: D% x #ml/kg fluid = 50.
Inborn Errors of Metabolism
Major classes include organic acidurias (profound anion gap metabolic acidosis) and urea cycle defects (hyperammonemia)
Recommendation: Draw gas and ammonia level.
Sepsis
Emphasized as a critical condition in the differential diagnosis for ill infants, though placed later in the mnemonic for easier recall.
Presentation and Diagnosis:
Sepsis in infants often presents nonspecifically, making early detection challenging.
Immediate drawing of blood cultures upon suspicion of sepsis.
Initial Treatment:
Prompt initiation of antimicrobials and fluids.
Use of vancomycin for gram-positive and MRSA coverage, a third-generation cephalosporin or pip-tazo for broad bacterial coverage, and acyclovir for HSV. (tailor based on age and institutional guidelines)
Supportive Care:
Highlights the necessity of fluid resuscitation to stabilize the patient.
Formula
Formula-Related Electrolyte Imbalances:
Incorrect mixing of infant formula can cause hypo- or hypernatremia.
Consequences of Electrolyte Imbalances:
Both conditions can lead to severe outcomes including altered mental status, seizures, coma, and potentially death.
Management Strategies:
Treatment varies based on the sodium levels:
Symptomatic hyponatremia is treated with hypertonic saline.
Hypernatremia requires fluid resuscitation.
Intestinal Catastrophe
Specific Conditions:
Malrotation with Midgut Volvulus: Twisting of the intestines that can obstruct blood flow.
Necrotizing Enterocolitis (NEC): Can occur in both full-term and preterm infants, involves inflammation and bacterial infection that can destroy bowel tissue.
Hirschsprung-associated Enterocolitis: Complication of Hirschsprung’s disease involving blockage and infection.
Intussusception: Older infants might only show altered mental status instead of the typical intermittent pain and lethargy.
Symptoms:
Common symptoms include bilious emesis (green vomit) or hematemesis (vomiting blood).
Emergency Response:
Urges early mobilization of pediatric surgery and radiology teams upon suspicion of these conditions.
Toxins
Includes intentional or unintentional ingestion.
One pill killers include: calcium channel blockers (CCB), tricyclic antidepressants (TCA), opiates, sulfonylureas, Class 1 antiarrhythmics, antimalarials, camphor, oil of wintergreen.
Seizures
The second ‘S’ in the mnemonic refers to seizures, which can be triggered by various conditions such as hypoglycemia, sepsis, inborn errors of metabolism, and trauma.
First-Line Treatment:
Actively seizing patients should initially be treated with benzodiazepines.
Second-Line Medications:
Includes fosphenytoin, phenobarbital, levetiracetam (Keppra), and valproic acid.
Management of Reversible Causes:
Urges prompt treatment of any identifiable causes like hypoglycemia or electrolyte imbalances.
Special Consideration:
Notes the possibility of pyridoxine-dependent epilepsy in neonates, recommending pyridoxine (vitamin B6) for intractable seizures unresponsive to multiple antiepileptic drugs (AEDs).
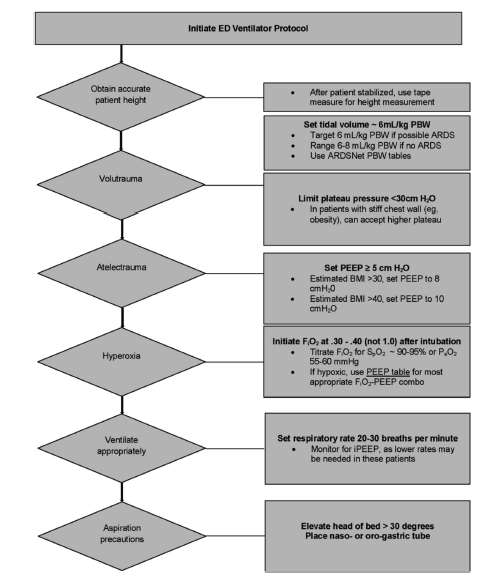
Non-cardiogenic pulmonary edema characterized by acute respiratory failure.
Berlin criteria for diagnosis include acute onset within 7 days, bilateral pulmonary infiltrates on imaging, not fully explained by cardiac failure or fluid overload, and impaired oxygenation with PaO2/FiO2 ratio <300 mmHg, even with positive end-expiratory pressure (PEEP) >5 cm H2O.
Severity based on oxygenation (Berlin criteria):
Mild: PaO2/FiO2 200-300 mmHg
Moderate: PaO2/FiO2 100-200 mmHg
Severe: PaO2/FiO2 <100 mmHg
Epidemiology:
Occurs in up to 23% of mechanically ventilated patients.
Mortality rate of 30-40%, primarily due to multiorgan failure.
Differentiation from Cardiogenic Pulmonary Edema:
Chest CT shows diffuse edema and pleural effusion in cardiogenic edema; patchy edema, dense consolidation in ARDS.
Ultrasound may show diffuse B lines in cardiogenic edema; patchy B lines and normal A lines in ARDS.
Hypothetical case: 21-year-old male with no previous medical history, experiencing a month of progressively worsening numbness, tingling, and weakness. Initially starting in his toes and spreading to his hips, and later involving his hands, the symptoms eventually escalated to the point of immobilization. Despite initially denying drug use, the patient admitted to using 40-60 canisters of nitrous oxide (whippets) every weekend for the last three months.
Background and Recreational Use of Nitrous Oxide
Nitrous oxide, a colorless, odorless gas with anesthetic properties.
Synthesized in the 18th century.
Its initial medical purpose expanded into recreational use due to its euphoric effects.
Resurgence as a recreational drug during the COVID-19 lockdowns.
Accessibility and legal status.
Public Misconceptions and Health Consequences
There are widespread misconceptions about nitrous oxide
Particularly the belief in its safety and lack of long-term health risks.
Contrary to popular belief, frequent use of nitrous oxide can lead to significant, sometimes irreversible, health issues.
Neurological Examination and Diagnosis
Key components of the examination include assessing strength, sensation, cranial nerves, and proprioception, with specific abnormalities such as symmetrically decreased strength in a stocking-glove pattern, upgoing Babinski reflex, and positive Romberg sign being indicative of potential toxicity.
Physical Exam Findings: Upper vs Lower Motor Neuron Lesions
Localize the Lesion- Differential Diagnoses for Extremity Weakness
Localize the Lesion- Differential Diagnoses for Extremity Weakness
Localize the Lesion- Differential Diagnoses for Extremity Weakness
MRI Findings and Subacute Combined Degeneration
The MRI displayed symmetric high signal intensity in the dorsal columns, a diagnostic feature identified as the inverted V sign or inverted rabbit ear sign.
Significance of the Inverted V Sign: This MRI sign is pathognomonic for subacute combined degeneration, indicating it is a distinct marker for this condition.
T2 Weighted Axial Images: The inverted V sign is observed in T2 weighted axial MRI images, which are used to evaluate the presence and extent of demyelination within the spinal cord.
Interpretation of Hyperintense Signals: Hyperintense signals on T2 weighted images generally indicate demyelination, where the protective myelin sheath around nerve fibers is damaged or destroyed.
Anatomical Location: The dorsal columns, located anatomically dorsal (toward the back) within the spinal cord, will appear toward the bottom of the screen in an axial (cross-sectional) view on the MRI.
Demyelination Appearance: Demyelination in the dorsal columns, typically situated in the thoracic spine, manifests as an upside-down V shape on the MRI, correlating with the described inverted V or rabbit ear sign.
Pathophysiology of SCD due to Nitrous Oxide
Nitrous Oxide’s Effect on Vitamin B12: Nitrous oxide inactivates vitamin B12 by oxidizing a cobalt component within the molecule, rendering the vitamin functionally ineffective despite adequate consumption and absorption.
Impact on Methionine Synthase: The oxidation of vitamin B12 by N2O prevents it from activating methionine synthase, an enzyme critical for important biochemical processes.
Folate to Tetrahydrofolate Conversion: Inactive methionine synthase cannot convert folate into tetrahydrofolate, which is necessary for DNA synthesis. This disruption can lead to megaloblastic anemia, a condition associated with N2O-induced subacute combined degeneration.
Conversion of Homocysteine to Methionine: Methionine synthase is also responsible for converting homocysteine to methionine. Methionine is essential for the maintenance of myelin integrity, the protective sheath around nerve fibers.
Demyelination and Neurological Symptoms: The inability to maintain myelin integrity due to disrupted methionine production leads to the demyelination of dorsal columns and peripheral motor/sensory nerves, characteristic of N2O-SCD.
Normal B12 Levels with Functional Deficiency: Blood levels of vitamin B12 can appear normal in individuals affected by N2O exposure, as the issue lies in the vitamin’s inactivation rather than its absence, creating a functional deficiency.
Diagnosis of N2O-SCD: To diagnose N2O-induced SCD, healthcare providers need to check for elevated levels of methylmalonic acid and homocysteine. These substances are typically metabolized with the help of vitamin B12, and their elevated levels indicate a functional deficiency of B12 due to N2O exposure.
Treatment and Management
Lack of Standardized Treatment: There is no universally accepted treatment protocol for N2O induced SCD, but common practices exist based on neurologist recommendations.
B12 Injection Protocol: A common approach involves administering vitamin B12 injections daily or every other day until there is noticeable improvement in symptoms. Once symptoms start to improve, the frequency of injections can be reduced to once a week.
Importance of Abstinence from N2O: For recovery to be possible, it is crucial that the patient completely abstains from using whippets (recreational N2O canisters). Continuing to use N2O can inactivate the administered vitamin B12, undermining the treatment efforts.
Recovery Process: Recovery from N2O induced SCD is typically slow and may not be complete. While remyelination and neurological function can gradually improve, the process is lengthy and may not fully return to baseline.
Recovery Statistics: Approximately 80% of individuals with N2O-SCD experience some improvement after a year of consistent B12 treatment. However, only between 10% and 20% of patients fully recover to their pre-condition baseline.
Risk Factors and Prevalence: The risk of developing SCD correlates with the frequency and quantity of N2O use. About 3.4% of individuals who use whippets will develop SCD, with the risk increasing to 8.5% among those who use more than 100 canisters per session. The case in point involved a patient using 20-40 canisters per session.
Increased Risk with Preexisting Conditions: Individuals who already have a vitamin B12 deficiency are at a greater risk of experiencing SCD symptoms, even with minimal use of whippets. This highlights the importance of understanding individual health conditions and potential vulnerabilities when assessing risk.
Conclusion and Preventive Measures
Providers should be vigilant in screening for nitrous oxide use among patients presenting with unexplained neurological symptoms. The goal is to enhance early detection and treatment of N2O-induced SCD and to educate patients on the potential long-term health consequences of recreational nitrous oxide use.
References
Neurology. Mumenthaler M, Mattle H, Taub E, ed. 4th Edition. Stuttgart: Thieme; 2003. doi:10.1055/b-005-148905
Zayia LC, Tadi P. Neuroanatomy, Motor Neuron. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554616/
Bhattacharyya S.Spinal Cord Disorders: Myelopathy, The American Journal of Medicine, Volume 131, Issue 11, 2018, Pages 1293-1297, ISSN 0002-9343,https://doi.org/10.1016/j.amjmed.2018.03.009.
Garg RK, Malhotra HS, Kumar N. Approach to a case of myeloneuropathy. Ann Indian Acad Neurol. 2016 Apr-Jun;19(2):183-7. doi: 10.4103/0972-2327.182303. PMID: 27293327; PMCID: PMC4888679.
Lim PAC. Transverse Myelitis. Essentials of Physical Medicine and Rehabilitation. 2020:952–9. doi: 10.1016/B978-0-323-54947-9.00162-0. Epub 2019 Apr 17. PMCID: PMC7151963.
Jayarangaiah A, Lui F, Theetha Kariyanna P. Lambert-Eaton Myasthenic Syndrome. [Updated 2023 Oct 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507891/
Nguyen TP, Taylor RS. Guillain-Barre Syndrome. [Updated 2023 Feb 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532254/
Froese DS, Fowler B, Baumgartner MR. Vitamin B12 , folate, and the methionine remethylation cycle-biochemistry, pathways, and regulation. J Inherit Metab Dis. 2019 Jul;42(4):673-685. doi: 10.1002/jimd.12009. Epub 2019 Jan 28. PMID: 30693532.
Guo CJ, S. Kaufman B. Inhalational Anesthetics. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds. Goldfrank’s Toxicologic Emergencies, 11e. McGraw-Hill Education; 2019. Accessed February 27, 2024. https://accessemergencymedicine-mhmedical-com.ezproxy.med.nyu.edu/content.aspx?bookid=2569§ionid=210274345
Lin JP, Gao SY, Lin CC. The Clinical Presentations of Nitrous Oxide Users in an Emergency Department. Toxics. 2022 Feb 26;10(3):112. doi: 10.3390/toxics10030112. PMID: 35324737; PMCID: PMC8950993.
Qudsiya Z, De Jesus O. Subacute Combined Degeneration of the Spinal Cord. [Updated 2023 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559316/
Hemmer B, Glocker FX, Schumacher M, et alSubacute combined degeneration: clinical, electrophysiological, and magnetic resonance imaging findingsJournal of Neurology, Neurosurgery & Psychiatry 1998;65:822-827.
Shah K, Murphy C. Nitrous Oxide Toxicity: Case Files of the Carolinas Medical Center Medical Toxicology Fellowship. J Med Toxicol. 2019 Oct;15(4):299-303. doi: 10.1007/s13181-019-00726-x. Epub 2019 Aug 6. PMID: 31388940; PMCID: PMC6825085.
Kalmoe MC, Janski AM, Zorumski CF, Nagele P, Palanca BJ, Conway CR. Ketamine and nitrous oxide: The evolution of NMDA receptor antagonists as antidepressant agents. J Neurol Sci. 2020 May 15;412:116778. doi: 10.1016/j.jns.2020.116778. Epub 2020 Mar 19. PMID: 32240970.
Defined as vaginal bleeding during early pregnancy (before 20 weeks) with a closed cervical os, no passage of fetal tissue, and IUP on ultrasound
Occurs in 20-25% of all pregnancies.
Initial Assessment and Management
Priority is to assess patient stability, establish good IV access, FAST may be helpful in identifying some ruptured ectopics early
Broad differential diagnosis is crucial to avoid mistaking conditions like ectopic pregnancy for other emergencies.
Importance of a detailed history and physical examination.
Diagnostic Approach
Essential tests include HCG level, urinalysis, and possibly CBC + blood type/Rh status.
Rhogam’s use is well-supported in second and third trimester bleeding; however, data is less robust for first trimester bleeding in preventing sensitization
Importance of interpreting b-HCG with caution and understanding HCG discriminatory zones.
Use of ultrasound imaging, both bedside and formal, to assess the pregnancy’s status.
Patient Counseling and Management
Open and honest communication about the prognosis of threatened abortion.
Addressing psychosocial aspects, including dispelling guilt and myths, and screening for intimate partner violence and mental health issues.
Recommendations against bedrest and certain activities
Lack of evidence supporting restrictions on sexual activity.
Standard pregnancy guidelines: avoiding smoking, alcohol, drug use, and starting prenatal vitamins.
Follow-up and Precautions
Adopting a wait-and-see approach for stable patients, with scheduled follow-ups for ultrasounds and beta-HCG tests.
Educating patients on critical warning signs that require immediate medical attention.
Emphasizing the importance of returning to the hospital if experiencing significant bleeding or other severe symptoms.
Take Home Points
Threatened Abortion is defined as Experiencing abdominal pain and/or vaginal bleeding during early pregnancy (before 20 weeks), characterized by a closed cervical os and no expulsion of fetal tissue. In these cases, it is important to assess patient stability promptly.
Keep your differential broad in these cases. The evaluation will in most cases involve a combination of labs and ultrasound imaging.
Understand that the Rhogam certainly has a role in second and third trimester vaginal bleeding in the Rh-negative patient, and that there is a dearth of good data on its role in the first trimester – it will ultimately be a decision that is made by you, OBGYN, and the patient.
Approach the interpretation of HCG levels with caution and remember that ectopic pregnancies might not adhere to conventional HCG levels.
Established follow up and discharge instructions are crucial. Manage stable patients with a watchful waiting approach, scheduling subsequent visits for continuous ultrasounds and HCG testing. Clearly outline the importance of immediate medical attention for symptoms such as intense bleeding, significant abdominal pain, fever, or feelings of insecurity at home.
Finally, we play an important role wherein we must ensure that the patient is medically stable and psychosocially safe. Here, compassionate communication is crucial when discussing what the diagnosis might entail, alleviate any feelings of blame or shame, and remain vigilant for signs of intimate partner violence or mental health issues. As emergency medicine physicians, it’s crucial for us to approach these cases with a comprehensive mindset.
Similar initial workup for children and adults: checking glucose levels for hypoglycemia and conducting an EKG.
The history and physical exam are crucial.
Dextrose Administration in Children:
Explanation of the ‘rule of 50s’ for determining the appropriate dextrose solution and dosage for children.
ECG Analysis:
Importance of ECG in diagnosing dysrhythmias like long QT syndrome, Brugada syndrome, catecholamine polymorphic V tach, ARVD, ALCAPA, and Wolff-Parkinson-White syndrome.
Younger children’s dependency on heart rate for cardiac output and the risk of arrhythmias in kids with congenital heart disease.
Narrow QRS complexes, Absence of P waves, Tachycardia
Congenital/Acquired
Ventricular Tachycardia
Wide QRS complexes, Tachycardia
Congenital/Acquired
Arrhythmogenic Right Ventricular Dysplasia (ARVD/C)
Epsilon waves, V1-V3 T wave inversions, Right bundle branch block
Congenital
Hypertrophic Cardiomyopathy (HCM)
Left ventricular hypertrophy, Deep Q waves
Congenital
Pulmonary Hypertension
Right ventricular hypertrophy, Right axis deviation
Acquired
Athlete’s Heart
Sinus bradycardia, Voltage criteria for left ventricular hypertrophy
Acquired
Catecholaminergic Polymorphic VT (CPVT)
Bidirectional or polymorphic VT, typically normal at rest
Congenital
Anomalous Origin of Left Coronary Artery from Pulmonary Artery (ALCAPA)
May be normal, signs of ischemia or infarction in severe cases
Congenital
History Taking:
Key aspects include asking about syncope with exertion, syncope after being startled, and syncope after pain or emotional stress.
Prolonged loss of consciousness may indicate seizures, and emotional stress and pain can trigger breath-holding spells.
Breath-Holding Spells:
Clarification of misconceptions about breath-holding spells, discussing their causes and characteristics, like cyanotic and pallid types.
Association with iron deficiency and the fact that most children outgrow these spells by age 8.
Physical Examination and History:
A cardiac exam is vital, with specific signs to look for, like murmurs in hypertrophic cardiomyopathy.
History can help identify the etiology of syncope, such as vasovagal responses or orthostatic hypotension.
Vasovagal Syncope:
Common in kids, especially teenagers, typically presenting with a prodrome of lightheadedness, diaphoresis, and pallor.
Normal glucose and EKG are expected in these cases.
Additional Lab Tests:
Pregnancy tests in reproductive-age women, and checking for less common causes like pulmonary embolism, subarachnoid hemorrhage, and toxic exposures.
Take Home Points:
Immediate assessments for syncope in children should include a FS to evaluate for hypoglycemia and an ECG to evaluate any cardiac rhythm or conduction abnormalities.
Apply the “Rule of 50s” for hypoglycemic patients to suggest which fluids should be used.
Refer to our table for ECG findings to look out for when reviewing ECG tracings for these patients.
Pay particular attention to clues in the history that would suggested HCOM or seizures.
Breath-holding spells usually resolve by eight
HCOM murmurs will increase with Valsalva maneuver
Always keep your differential broad when approaching these patients given the heterogeneity of potential pathology that could lead to this chief complaint
Decision-Making Process: Balancing acute management with long-term treatment strategies.
Take Home Points
Differentiation in AF with RVR Types: It’s essential to distinguish between primary AF with RVR, chronic AF with RVR related to other health issues, and new-onset AF (NOAF) with RVR in critically ill patients, as each type necessitates a unique approach to treatment.
ACLS Guidelines for AF with RVR: The ACLS guidelines provide a treatment framework, particularly recommending immediate synchronized cardioversion for unstable patients. However, these guidelines may have limited effectiveness for chronic AF with RVR patients suffering from underlying critical illnesses.
ECG Diagnosis in AF: Identifying AF on an ECG is crucial, with key indicators being an irregular rhythm without clear P waves and a ventricular rate exceeding 100 bpm. Accurate ECG interpretation guides effective treatment planning.
Special Cases like WPW Syndrome: WPW syndrome and similar conditions require careful treatment consideration, as standard AF treatments can worsen these conditions. Alternatives like procainamide or amiodarone are often more appropriate.
Patient-Centered Management of AF with RVR: Management should account for the patient’s overall health, underlying conditions, the chronicity of AF, and other comorbidities. Drugs like metoprolol and diltiazem offer benefits and risks, demanding personalized treatment plans.
Pathophysiology in Critical AF Patients: Understanding the underlying pathophysiology in critically ill patients is vital. Tachycardia in these cases might be compensatory, necessitating an investigation into causes like myocarditis, dehydration, or GI bleeding.
Systematic Evaluation with TACHIES Mnemonic: The mnemonic TACHIES (Thyrotoxicosis, Alcohol withdrawal, Cardiac issues, Hemorrhage, Intervals [WPW], Embolus, Sepsis) aids in systematically assessing and addressing emergent tachycardia causes in critically ill patients.
Three or more sustained episodes of VF, VT, or appropriate ICD shocks in a 24-hour period
Pathophysiology: Understanding the origin and mechanism
Sympathetic drive/adrenergic surge
Underlying pathology: Sodium channelopathies, infiltrative disease like cardiac sarcoidosis, etc.
RF’s / trigger / population (reversible cause in ~25% of patients)
MI
Electrolyte Derangements (emphasis on potassium and magnesium)
New/worsening heart failure
Catecholamine Surge
Drugs (stimulants, cocaine, amphetamines, etc)
QT Prolongation
Thyrotoxicosis
Clinical Presentation:
Symptoms of VT: spectrum of symptoms – from palpitations to syncope to cardiac arrest
Differentiating VT from other potential ER presentations.
Diagnostics in ER:
Electrocardiogram (ECG): Recognizing VT patterns.
Monomorphic vs polymorphic (Torsades) may change management
Wide QRS
Fusion best
Capture beats
Concordance
AV-dissociation
Lab tests: Potassium, magnesium, troponins, TFTs, etc.
Acute Management in the ER:
Hemodynamically stable vs. unstable V
Unstable = cardioversion
Sedation
Catecholamine surge should be considered
No ideal agent
Etomidate or propofol can be considered
Ketamine may worsen irritability
Pharmacological treatments:
Amiodarone
Class III antiarrhythmic
Most studied in VT storm
First line
Beta Blockers
Propranolol
B1 and B2 activity
Non-pharmacological approaches:
Immediate synchronized cardioversion
IABP / ECMO considered for HD unstable patient
Cath lab if ischemic etiology suspected
Stellate Ganglion Block
Take Home Points
Definition: VT Storm is commonly defined as three or more sustained episodes of ventricular fibrillation, ventricular tachycardia, or appropriate ICD shocks within a 24-hour period.
Varied Presentation: Patients may experience a range of symptoms from palpitations to severe hemodynamic instability.
ECG and Diagnosis: Initial ECG may not show VT; continuous cardiac monitoring or device interrogation may be required for diagnosis.
VT Identification: Look for wide QRS, rate over 100, fusion beats, capture beats, and AV dissociation to identify VT.
Management in Hemodynamic Instability: Cardiovert if the patient shows signs of hemodynamic instability.
Sedation Considerations: Be cautious with sedation, especially with ketamine, as it may worsen cardiac irritability in these already adrenergic state patients.
Medication Choices: Typically, amiodarone and propranolol are used to manage VT Storm.
Cardiology Involvement: Involve cardiology early on, as treatment may extend beyond medications.
2023 study: Of the 145 children with hemolyzed hyperkalemia, 142 (97.9%) had a normal repeat potassium level. Three children (2.1%) had true hyperkalemia: one had known chronic renal failure and was referred to the ED due to concern for electrolyte abnormalities; the other 2 patients had diabetic ketoacidosis (DKA).
Clinical Presentation / eval
Symptomatic vs. Asymptomatic:
“First symptom of hyperkalemia is death”
If severe, ascending muscle weakness → paralysis
Point at which patients experience symptoms depends on chronicity
>7 mEq/L if chronic and can be lower if acute
Hyperkalemia can be a cause of non-specific GI symptoms
EKG Changes:
ECG findings may be the first marker the ER doc gets that something is wrong
Typical changes:
Peaked T-waves, shortened QT
Lengthening of PR interval and QRS duration
Bradycardia / Junctional rhythm
Hyperkalemia can produce bradycardia without other ECG findings
Ones associated with VT/VF/code, death in one study: QRS widening (RR = 4.74), Junctional Rhythm (RR = 7.46), HR <50 (RR = 12.29) while no adverse outcomes with just peaked T waves or PR prolongation (Durfey, 2017)
Don’t be fooled by a normal ECG, may be normal, but it’s also on case report level to have K > 9 and a normal ECG
Series of 127 patient (K 6-9.3), no serious arrhythmia noted, only 46% had ECG changes, (Acker, 1998)
ECG changes are not linear, there is no exact association between K+ levels and ECG changes
ECG changes may be hidden and subtle in patients with underlying inter-ventricular conduction delay (BBBs)
Be suspicious of the patient with LBBB > 160 ms or RBBB > 140 ms
BRASH Syndrome
Synergism between hyperkalemia, renal failure/injury and AV nodal blocking agents -> may produce ECG changes out of proportion to serum potassium levels.
Labs
Chem, VBG, +/- CK if you think muscle breakdown is at play (Tintinalli talks about looking at urine K, but this is not most people’s practice)
Realistically 2 hours to get back chemistry in most settings ≈ eternity
Management in the ER
Discontinue/hold any nephrotoxins or medications in suspected medication-induced hyperkalemia
A. Acute Management Strategies:
Cardiac protection with calcium
1g over 5-10 mins
Lasts 30-60 mins, may have to redose
Dose considerations if on digoxin
AEs: Calciphylaxis and hypercalcemia
Fast pushes can result in hypotension, arrhythmia
Calcium chloride vs calcium gluconate
Caution in patients taking Digoxin
IVF choice – NS vs LR
Caution/Avoid fluid in patients with ESRD/CHF or signs of VOL
Shifting potassium:
insulin/glucose
5 units vs 10 units
5 similar effect, less hypoglycemic episodes (LaRue 2017)
If doing 10 units, start D10W at 50-75 cc/h after amp of d50 but be mindful that anuric patient who missed HD may not have much room for volume
Decrease but about 0.5-1.2 mEq/L
Effect starts 10-20 mins after administration and can last 4-6 hours
Albuterol
10-20 mg over 10 mins (NB: higher dose than for asthma)
Peak effect at 90 mins
Decreases by 0.5 – 1.0 mEq/L alone
With insulin, ~1.2 mEq/L, additive effect
Bicarbonate
Controversy. Useless in hyperkalemic, nonacidotic patient. Useful as drip but takes hours to work, again, volume in anuric patient an issue
May be most useful in patients with renal failure and hyperkalemia 2/2 volume loss
Hypertonic Bicarb is ineffective – More potassium is pulled out of cells due to osmotic shift.
Removal:
Lokelma (Sodium Zirconium cyclosilicate)
Luckily residents have never had to use Kayexalate
Can start working in 1-2 hours of administration
0.37 mEq/L reduction at 4 hours after 10 g
Not a magic bullet in patients who need dialysis
Diuretics
No studies that demonstrate effectiveness in this ED setting
May be effective in patients with normal renal function
If patient not anuric, may be worth using, can give 40 mg, but again, should not be the only attempted method of removing K
Nephron BOMB
Loop Diuretic (160-250 mg IV Lasix or 4-5 mg IV Bymex)
Thiazide (500-1000 mg IV chlorothiazide or 5-10 mg metolazone)
+/- Acetazolamide
+/- Fludrocortisone
May help stimulate the kidneys to secrete potassium
Primarily helpful in patients with mineralocorticoid deficiencies
Dialysis
Involve renal early because it takes a while to call in an HD nurse sometimes
If no access and emergent HD is required → HD catheter placement
Strategies for suspected Brash syndrome
Epinephrine/Levo (if hypotensive/bradycardic)
Calcium gtt
Disposition/wrap up
Many factors at play here – patient preference, access, degree of hyperkalmia, identifiable / corrected cause
Take Home points
Hyperkelamia causes can be put into three categories, pseudohyperkalemia, due to redistribution, and due to total body increase in potassium. Check out the show notes for a more complete list
Hyperkalemia can be difficult to pick up on before the labs come back because it can lurk without symptoms or even ECG changes
If a patient does have ECG changes, they may not follow that linear pattern that is traditionally taught and ECGs can be poorly sensitive. Now, if you do see changes, the ones that are more commonly associated with adverse events are QRS widening, junctional rhythm, and bradycardia
Treatment is a numbers game, calcium for cardiac stabilization can last just 30-60 minutes, insulin will be the fastest way to shift potassium back into cells, but be mindful that 10 units is associated with increased episodes of hypoglycemia whereas 5 units may have the same effect in reducing potassium. And albuterol is at a much higher dose than what is given for asthma
Lokelma is now a pillar of treatment for removal of potassium.
Diuretics with the goal of kiuresis may have a role in the oliguric patient, and increased doses along with other agents may buy time in patients with severe hyperK when HD is not readily available
Involve renal early if you think that the patient will require HD
Consider POCUS, lactate, central venous saturation, and acid-base status
Peripheral Pressors
Can safely be administered peripherally via large bore IVs in proximal upper extremity
Sites: Cephalic or basilic veins
Adverse Events: Low at 1.8% based on meta-analysis
Actions in case of extravasation: Phentolamine injection, nitroglycerin paste
Push-Dose Pressors
Primarily Phenylephrine (peri-intubation, during procedures)
Also Epinephrine for peri-code situations
Doses: Epi – 5-20 mcg every 2-5 min
Take-Home Points
Most used medications are going to be norepinephrine, vasopressin, phenylephrine, and epinephrine.
Consider these medications if there are signs of end-organ dysfunction, there is a considerable delta in baseline BP, systolic is less than 90 and/or MAP is less than 65
Norepinephrine is a good pressor for a lot of the situations that we encounter in the emergency department, such as septic shock, undifferentiated shock and hypovolemic shock.
Vasopressin is commonly the second we reach for in most of these scenarios
Epinephrine will be first for anaphylactic shock and may be the third agent in septic shock
Think about phenylephrine in high-output states (patients with tachydysrhythmias), or with AS, though be cautious in patient with low cardiac output
The benefits outweigh risks for peripheral pressors in situations where you promptly have to increase blood pressure while you work on central access
Push-dose pressures can help you in a peritinbatuion or pericode situation because it is going to be one of the fastest ways we can boost BP while we work on other measures to stabilize the patient
Additional References
Importance of RUSH (Rapid Ultrasound in SHock) exam for diagnosis and treatment planning: https://emcrit.org/rush-exam/
Pain in joint for pediatric patient has a broad differential, including transient synovitis and septic arthritis
Transient synovitis, also known as toxic synovitis, is a common condition affecting kids aged 3-10 and often occurs after a viral infection. It is typically self-limiting and not considered a serious condition.
Septic arthritis is an infection in the joint space, typically affecting only one joint. It is often difficult to diagnose due to the fact that many patients, particularly under the age of 3, may not be able to localize their pain to a specific joint.
Workup
Diagnostic work-up for septic arthritis begins with blood work, which includes a complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and blood cultures. Lyme disease studies may also be necessary since Lyme disease can cause joint pain.
Patients with transient synovitis typically have mild elevation in inflammatory markers, while those with septic arthritis usually show a significant elevation.
Imaging studies, including X-rays, ultrasound to evaluate for a joint effusion, and MRI to assess for associated osteomyelitis, are also part of the diagnostic approach.
The Kocher criteria, developed specifically for septic arthritis of the hip, are a useful tool for clinical decision-making. The criteria include fever above 38.5 C, inability to bear weight, ESR above 40, and a white blood cell count above 12,000.
1 criterion met = 3% probability of septic arthritis
2 criteria met = 40% probability of septic arthritis
3 criteria met = 93% probability of septic arthritis
4 criteria met = 99+% probability of septic arthritis
If septic arthritis is suspected, orthopedics should be consulted immediately. Joint fluid aspiration is necessary for diagnosis and should not be delayed. The fluid should be sent for cell count, gram stain, glucose, culture, and PCR if available.
Septic arthritis is most commonly caused by bacterial infections, with Staph aureus being the most common organism. In school-age children, other bacteria such as Strep pyogenes, Strep pneumoniae, and Haemophilus influenzae should also be considered. In preschool-aged children, K. kingae is also considered. In older children and neonates, the range of potential bacteria varies.
Management
Empiric antibiotic therapy should target the most likely organisms and should not be delayed. Antibiotics may be narrowed once culture results are obtained.
The choice of antibiotics is dependent on the age group, with specific combinations suggested for neonates, children between 1 month and 4 years, and children aged 5 and older.
Cultures are only positive in 50-60% of cases. Synovial fluid PCR studies can help narrow antibiotic treatment.
Take Home Points
Limp in the pediatric population can commonly be transient synovitis but we should always consider septic arthritis
Some clues in the history and physical that would point you towards septic arthritis include fever, refusal to bear weight, and limited range of motion on exam
We are going to have to get labs, including CBC, inflammatory markers, and preoperative labs, along with an XR and possibly an ultrasound
Kocher criteria is one tool that can help us determine if this is a patient that requires a joint tap.
Arthrocentesis is the gold standard for diagnosis, but antibiotics should be started promptly if the diagnosis is suspected.
The choice of antibiotics is dependent upon age group.
Neonates get vanc/cefepime, kids 1-4 yo get vanc / ceftriaxone
Older than 5 yo get vancomycin
Add ceftriaxone to them if patient has sickle cell disease, are immunocompromised, or Lyme or STI are suspected
Always cross check with institutional preferences / guidelines when choosing antibiotics
IV calcium supplementation with 100-300 mg Ca2+ raises serum Ca2+ by 0.5 – 1.5 mEq
For acute but mild symptomatic hypocalcemia: 200-1000mg calcium chloride IV or 1-2g IV calcium gluconate over 2 hours
For severe hypocalcemia: 1g calcium chloride IV or 1-2g IV calcium gluconate IV over 10 minutes repeated q 60 min until symptoms resolve
References:
Cooper MS, Gittoes NJ. Diagnosis and management of hypocalcaemia. BMJ 2008; 336:1298.
Desai TK, Carlson RW, Geheb MA. Prevalence and clinical implications of hypocalcemia in acutely ill patients in a medical intensive care setting. Am J Med 1988; 84:209.
Goltzman, D. Diagnostic approach to hypocalcemia. UpToDate. UpToDate; Jul 17, 2020. Accessed April 29, 2022. https://www.uptodate.com/contents/plantar-fasciitis
Kelly A, Levine MA. Hypocalcemia in the critically ill patient. J Intensive Care Med 2013; 28:166.
Pfenning CL, Slovis CM: Electrolyte Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 125: p 1636-53.
Swaminathan, A. (2016, January 27). Hypocalcemia. CoreEM. Retrieved April 29, 2022, from https://coreem.net/core/hypocalcemia/
Vantour L, Goltzman D. Regulation of calcium homeostasis. In: rimer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 9th ed, Bilezikian JP (Ed), Wiley-Blackwell, Hoboken, NJ 2018. p.163.
Algorithm for Anticoagulated Bleeding Patient in the ED:
Indications for Anticoagulation Reversal:
References:
Baugh CW, Levine M, Cornutt D, et al. Anticoagulant Reversal Strategies in the Emergency Department Setting: Recommendations of a Multidisciplinary Expert Panel. Ann Emerg Med. 2020;76(4):470-485. doi:10.1016/j.annemergmed.2019.09.001
Eikelboom JW, Quinlan DJ, van Ryn J, Weitz JI. Idarucizumab: The Antidote for Reversal of Dabigatran. Circulation. 2015 Dec 22;132(25):2412-22. doi: 10.1161/CIRCULATIONAHA.115.019628. PMID: 26700008.
Fariborz Farsad B, Golpira R, Najafi H, et al. Comparison between Prothrombin Complex Concentrate (PCC) and Fresh Frozen Plasma (FFP) for the Urgent Reversal of Warfarin in Patients with Mechanical Heart Valves in a Tertiary Care Cardiac Center. Iran J Pharm Res. 2015;14(3):877-885.
Fariborz Farsad B, Golpira R, Najafi H, et al. Comparison between Prothrombin Complex Concentrate (PCC) and Fresh Frozen Plasma (FFP) for the Urgent Reversal of Warfarin in Patients with Mechanical Heart Valves in a Tertiary Care Cardiac Center. Iran J Pharm Res. 2015;14(3):877-885.
Palta S, Saroa R, Palta A. Overview of the coagulation system. Indian J Anaesth. 2014;58(5):515-523. doi:10.4103/0019-5049.144643
Siegal DM, Curnutte JT, Connolly SJ, Lu G, Conley PB, Wiens BL, Mathur VS, Castillo J, Bronson MD, Leeds JM, Mar FA, Gold A, Crowther MA. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. N Engl J Med. 2015 Dec 17;373(25):2413-24. doi: 10.1056/NEJMoa1510991. Epub 2015 Nov 11. PMID: 26559317.
Botha A, Jacobs F, Postma C. Retrospective analysis of etiology and comorbid diseases associated with Ludwig’s Angina. Ann Maxillofac Surg 2015; 5:168.
Boscolo-Rizzo P, Da Mosto MC. Submandibular space infection: a potentially lethal infection. Int J Infect Dis 2009; 13:327.
Brook I. Microbiology and principles of antimicrobial therapy for head and neck infections. Infect Dis Clin North Am. 2007 Jun;21(2):355-91, vi. doi: 10.1016/j.idc.2007.03.014. PMID: 17561074.
Chong W, Hijazi M, Abdalrazig M, Patil N. Respect the Floor of the Mouth. J Emerg Med. 2020 Jul;59(1):e27-e29. doi: 10.1016/j.jemermed.2020.04.015. Epub 2020 May 19. PMID: 32439254.
http://www.emdocs.net/ludwigs-angina-2/
Mohamad I, Narayanan MS. “Double Tongue” Appearance in Ludwig’s Angina. N Engl J Med 2019; 381:163.
Saifeldeen K, Evans R. Ludwig’s angina. Emerg Med J. 2004 Mar;21(2):242-3. doi: 10.1136/emj.2003.012336. PMID: 14988363; PMCID: PMC1726306.
Wolfe MM, Davis JW, Parks SN. Is surgical airway necessary for airway management in deep neck infections and Ludwig angina? J Crit Care. 2011 Feb;26(1):11-4. doi: 10.1016/j.jcrc.2010.02.016. PMID: 20537506.
Bense L, Lewander R, Eklund G, et al. Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest 1993; 103:433.
Bense L, Wiman LG, Hedenstierna G. Onset of symptoms in spontaneous pneumothorax: correlations to physical activity. Eur J Respir Dis 1987; 71:181.
Brown SGA, Ball EL, Perrin K, Asha SE, Braithwaite I, Egerton-Warburton D, Jones PG, Keijzers G, Kinnear FB, Kwan BCH, Lam KV, Lee YCG, Nowitz M, Read CA, Simpson G, Smith JA, Summers QA, Weatherall M, Beasley R; PSP Investigators. Conservative versus Interventional Treatment for Spontaneous Pneumothorax. N Engl J Med. 2020 Jan 30;382(5):405-415. doi: 10.1056/NEJMoa1910775. PMID: 31995686.
Chardoli M, Hasan-Ghaliaee T, Akbari H, Rahimi-Movaghar V. Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma. Chin J Traumatol 2013; 16:351.
Chan KK, Joo DA, McRae AD, et al. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst Rev 2020; 7:CD013031.
Ebrahimi A, Yousefifard M, Mohammad Kazemi H, et al. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Meta-Analysis. Tanaffos 2014; 13:29.
Gobbel Jr WG, Rhea Jr WG, Nelson IA, Daniel RA. Spontaneous pneumothorax. J Thorac Cardiovasc Surg 1963; 46:331.
Lesur O, Delorme N, Fromaget JM, et al. Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest 1990; 98:341.
Lichtenstein DA, Mezière G, Lascols N, et al. Ultrasound diagnosis of occult pneumothorax. Crit Care Med 2005; 33:1231.
Melton LJ 3rd, Hepper NG, Offord KP. Influence of height on the risk of spontaneous pneumothorax. Mayo Clin Proc 1981; 56:678.
Ohata M, Suzuki H. Pathogenesis of spontaneous pneumothorax. With special reference to the ultrastructure of emphysematous bullae. Chest 1980; 77:771.
Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med 2000; 342:868.
EKG Findings in de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. doi: 10.1016/0002-8703(82)90480-x. PMID: 6121481.
Table 1 in de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. doi: 10.1016/0002-8703(82)90480-x. PMID: 6121481.
REFERENCES:
de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. doi: 10.1016/0002-8703(82)90480-x. PMID: 6121481.
Lee, M., & Chen, C. (2015). Myocardial Bridging: An Up-to-Date Review. Journal of Invasive Cardiology, 27(11), 521–528.
Lin AN, Lin S, Gokhroo R, Misra D. Cocaine-induced pseudo-Wellens’ syndrome: a Wellens’ phenocopy. BMJ Case Rep. 2017 Dec 14;2017:bcr2017222835. doi: 10.1136/bcr-2017-222835. PMID: 29246935; PMCID: PMC5753703.
Rhinehardt, J., Brady, W. J., Perron, A. D., & Mattu, A. (2002). Electrocardiographic manifestations of Wellens’ syndrome. The American Journal of Emergency Medicine, 20(7), 638–643. https://doi.org/10.1053/ajem.2002.34800
Non-contrast head CT showing SAH (Case courtesy of Dr. David Cuete, Radiopaedia.org, rID: 22770)
Hunt-Hess grade and mortality (from Lantigua et al. 2015.)
Hunt-Hess grade
Mortality (%)
1. Mild Headache
3.5
2. Severe headache or cranial nerve deficit
3.2
3. Confusion, lethargy, or lateralized weakness
9.4
4. Stupor
23.6
5. Coma
70.5
Ottawa Subarachnoid Hemorrhage Rule, and appropriate population for rule application (from Perry et al. 2017)
Apply to patients who are:
Alert
≥ 15 years old
Have new, severe, atraumatic headache that reached maximum intensity within 1 hour of osnet
Do not apply to patients who have:
New neurologic deficits
Previous diagnosis of intracranial aneurysm, SAH, or brain tumor
History of similar headaches (≥ 3 episodes over ≥ 6 months)
SAH cannot be ruled out if the patient meets any of the following criteria:
Age ≥ 40
Symptom of neck pain or stiffness
Witnessed loss of consciousness
Onset during exertion
“Thunderclap headache” (defined as instantly peaking pain)
Limited neck flexion on examination (defined as inability to touch chin to chest or raise head 3 cm off the bed if supine)
___________________________
Special Thanks To:
Dr. Mark Iscoe, MD (Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health, NYC Health + Hospitals/ Bellevue)
___________________________
References:
Bellolio MF, Hess EP, Gilani WI, et al. External validation of the Ottawa subarachnoid hemorrhage clinical decision rule in patients with acute headache. Am J Emerg Med. 2015;33(2):244-9.
Carstairs SD, Tanen DA, Duncan TD, et al. Computed tomographic angiography for the evaluation of aneurysmal subarachnoid hemorrhage. Acad Emerg Med. 2006;13(5):486-492.
Connolly ES, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43(6):1711-1737.
Czuczman AD, Thomas LE, Boulanger AB, et al. Interpreting red blood cells in lumbar puncture: distinguishing true subarachnoid hemorrhage from traumatic tap. Acad Emerg Med. 2013;20(3):247-256.
Dugas C, Jamal Z, Bollu PC. Xanthochromia. [Updated 2020 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526048/
Goldstein JN, Camargo CA, Pelletier AJ, Edlow JA. Headache in United States emergency departments: demographics, work-up and frequency of pathological diagnoses. Cephalalgia. 2006;26(6):684-90.
Kumar A, Niknam K, Lumba-brown A, et al. Practice Variation in the Diagnosis of Aneurysmal Subarachnoid Hemorrhage: A Survey of US and Canadian Emergency Medicine Physicians. Neurocrit Care. 2019.
Lantigua H, Ortega-Gutierrez S, Schmidt JM, et al. Subarachnoid hemorrhage: who dies, and why? Crit Care. 2015;19:309.
Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389(10069):655-666.
Mayer PL, Awad IA, Todor R, et al. Misdiagnosis of symptomatic cerebral aneurysm. Prevalence and correlation with outcome at four institutions. Stroke. 1996;27(9):1558-63.
Meurer WJ, Walsh B, Vilke GM, Coyne CJ. Clinical guidelines for the emergency department evaluation of subarachnoid hemorrhage. J Emerg Med. 2016;50(4):696-701.
Perry JJ, Spacek A, Forbes M, et al. Is the combination of negative computed tomography result and negative lumbar puncture result sufficient to rule out subarachnoid hemorrhage? Ann Emerg Med. 2008;51(6):707-713
Perry JJ, Stiell IG, Sivilotti MLA, et al. High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study. BMJ. 2010;341:c5204.
Perry JJ, Stiell IG, Sivilotti MLA, et al. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ. 2011;343(jul18 1):d4277-d4277.
Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA. 2013;310(12):1248-55.
Perry JJ, Sivilotti MLA, Sutherland J, et al. Validation of the Ottawa Subarachnoid Hemorrhage Rule in patients with acute headache. CMAJ. 2017;189(45):E1379-E1385.
Vermeulen MJ, Schull MJ. Missed diagnosis of subarachnoid hemorrhage in the emergency department. Stroke. 2007;38(4):1216-21.
Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health, NYC Health + Hospitals/ Bellevue
New York City Poison Control Center
References:
Christian MR, et al. Do rapid comprehensive urine drug screens change clinical management in children? Clin Toxicol (Phila). 2017;57:977-980.
Grunbaum AM, Rainey PM (2019). Chapter 7: Laboratory Principles. In Goldfrank’s toxicologic emergencies. New York, NY: McGraw-Hill Education.
Moeller K, Kissack J, Atayee R, Lee K. Clinical Interpretation of Urine Drug Tests: What Clinicians Need to Know About Urine Drug Screens. Mayo Clinic Proceedings Review. Volume 92, Issue 5, p774-796, May 1, 2017. https://www.mayoclinicproceedings.org/article/S0025-6196(16)30825-4/fulltext
Congratulations to a wonderful group of physicians. It is a pleasure to recognize your great accomplishments in the presence of your friends, families, loved ones and the residents and faculty who have learned so much from and with you. I would first like to recognize those of you who are members of the Gold Humanism Honor Society.
There are a remarkable number of awardees in our graduating class of 2020.
CLASS OF 2020
Joe Bennett (R)
Max Berger (R)
Ashley Miller (R)
Leigh Nesheiwat (S)
Kristen Ng (R)
Emily Unks (S)
AND
Arie Francis (R)
Nisha Narayanan (S)
FUTURE PGY-4
Elena Dimiceli (S)
Kamini Doobay (S)
Mark Iscoe (R)
FUTURE PGY-3
Stasha O’Callaghan (S)
Nicholus Warstadt (S)
FUTURE PGY-1
Aaron Bola (S)
Alison (Ali) Graebner (S)
Aron Siegelson (S)
Melissa Socarras (S)
Sarah Spiegel (S)
Thomas Sullivan (S)
Christy Williams (S)
GOLD HUMANISM CORE VALUES
Integrity, Excellence, Compassion, Altruism, Respect, Empathy, Service
These are the values you want as a doctor for yourself or a loved one,
to have outstanding listening skills with patients
to be at your side during a medical emergency,
to have exceptional interest in service to the community,
to have the highest standards of professionalism
to integrate a humanistic approach in patient care.
These values are what brought all of you to NYU-Bellevue and that you have honed throughout your training. The remainder of this talk shows how all of you have been successful and demonstrated these values some of you were elected to the Gold Humanism—all of you have achieved humanistic success.
Your personal efforts in the face of uncertainty of the evolution of the pandemic, the inadequate supplies, the hospital and governmental problematic decisions are remarkable. In our country, the President did not mourn the loss of more than a 100,000 human beings and the needs of society. Nor did he provide the leadership and moral support that the country desperately needed to optimally handle this unprecedented crisis. You, in contrast, demonstrate unflappable commitment to address and overcome obstacles to care for your patients, assist your peers, educate and care for your families and friends, while also caring for yourselves. This is a tribute to your humanism. You created essential ways to help patients who were isolated from families and friends during the critical phases of COVID-19. You utilized new tools to communicate your sorrow, your compassion and love, to maintain essential humanistic traditions of medicine while you could not talk, touch or utilize other essential skills to the fullest extent of a physician.
When you recognized that all your knowledge of the social determinants of medicine was playing out as COVID-19 assaulted the poorest in our country, the people of color, the people with essential jobs without personal protective equipment, the people crowded in apartments and subways and buses, you spoke up and acted with appreciation and understanding of these disparities. You recognized that our system of using medicine to correct the societal social institutionally entrenched disparities was inadequate. George Floyd’s death, and that of Breonna Taylor and innumerable others document the racism in America that destroys a part of us each and every day and by extension reinforces and normalizes white privilege. The ever increasing body of video evidence of the horrors of systemic racism is indisputable. You recognized that the American system of criminalization of social determinants is unacceptable. You spoke up and demonstrated that you saw our blind spots on policing and race. You protested to demand change in America.
Change for equity and justice must occur throughout our society. “Black Lives Matter” will only be realized when the social determinants are truly addressed through changes that impact every vulnerable person. We must recognize that person, institutional and societal failures will not be corrected by medicalizing or criminalizing of socially determined inequities. Racism is systemic. Today you are seeking to create essential changes in medicine that will only occur when all the workplaces and governmental sites across the country, are enriched to allow a full representation of all the voices of all the people.
You are leaders in the response to COVID-19 and the fight against racism. You will not only be remembered for having been present, but particularly for how you have responded. Thank you for your courage, creativity, resiliency and ability to transition and advance under duress. It was a privilege to watch you demonstrate the importance of your core values and the impact that your training here at NYU/Bellevue has had on your ability to integrate them into your practice.
You are truly individuals of immense potential, ideal for advancing our world. How you keep these values and grow them in the next developmental stage of your careers will be critical. Each of you will contribute according to your talent, resources and priorities whether in clinical practice, academics, advocacy or public health. Always in every encounter with patients and their families “Be the change that you wish to see in the world” Mahatma Ghandi.
Infectious workup if suspected: cultures, grain stains
Imaging:
CXR: 20% will be normal. May see tumour, cavity, effusion, infiltrate, PTX. Early pulmonary hemorrhage may present as infiltrate
CT: only for stable patients! May see bronchiectasis, cavitary lesions, acinar nodules, tumours
CTA: bronchial arteries, aneurysms, PE
ECHO: identify valvular abnormalities, signs of PE, aortic aneurysm
Bronchoscopy:
Not often performed in ED, but therapeutic & diagnostic
Allows direct visualization of tumours, foreign bodies, granulomas, infiltration, as well as local therapy (vasoconstrictive agents, stent/ balloon tamponade, electrocautery, procoagulants)
2 x suction, preoxygenation, patient positioned upright, >8Fr ETT to facilitate suctioning/ bronch
If bleeding side can be identified, consider “selective intubation” into nonbleeding lung to minimize further aspiration of blood and to provide ventilation
Life threat = asphyxiation, not exsanguination. ~Only 150cc anatomic dead space in major airways
2 x large bore IVs
MTP prn vs volume resuscitation
“Bad lung down” in lateral position: theoretical belief to minimize reflux of blood into normal lung
Correct coagulopathy
Consider nebulized TXA for nonmassive hemoptysis (500mg w/ NS per neb)
Double-blind, randomized controlled trial in 2018
Nebulized TXA (500mg TID) vs placebo (normal saline) in hemodynamically stable adult patients admitted with mild hemoptysis (<200 mL/ 24hr) and no respiratory instability
Additional exclusion criteria included those with renal failure, hepatic failure, or coagulopathy
Assessed mortality and hemoptysis recurrence rate at 30 days and 1 year
25 patients randomized to receive TXA nebs, 22 randomized to receive normal saline nebs
Results:
Resolution of hemoptysis within 5 days of admission was significantly higher in TXA-treated patients than placebo patients (96% vs 50%; P < 0.0005)
Mean hospital length of stay was shorter for TXA group (5.7 +- 2.5 days vs 7.8 +- 4.6 days; P = 0.046)
Fewer patients in TXA group required invasive procedures to control bleeding vs placebo group (0% vs 18.2%; P = 0.041)
No side effects were noticed in either group
Antibiotics if infectious
Bronchoscopy: local therapy (vasoconstrictive agents, stent/ balloon tamponade, electrocautery, procoagulants)
Rigid bronch for unstable patients to evacuate clots vs fiberoptic bronch for stable patients
Bronchial artery embolization (call IR early!)
May require lobectomy or pneumonectomy (consult thoracic surgery)
DISPOSITION:
Low threshold for higher level of care: only mild, hemodynamically stable hemoptysis on floor
Discharge: only if certain regarding etiology in healthy, hemodynamically stable patients with scant, resolved hemoptysis, no coagulopathy, and reassuring workup
Ensure patients have reliable follow up and avoid smoking. Strict return precautions!
REFERENCES:
Kiraly A, Pang P, Cheema N. Hemoptysis. In: Schaider J, Barkin R, Hayden S, Wolfe R, Barkin A, Shayne P, Rosen P. Rosen and Barkin’s 5-Minute Emergency Medicine Consult. 5th Edition. Philadelphia, PA: Wolters Kluwer; 2015; 504-505.
Nickson, C. Haemoptysis. Life in the Fastlane. [litfl.com/haemoptysis/]. Updated April 9, 2019. Retrieved February 10, 2020.
Wand O, Guber E, Guber A, Schochet GE, Israeli-Shani L, Shitrit D. Inhaled Tranexamic Acid for Hemoptysis Treatment: A Randomized Controlled Trial. Chest. December 2018; 154(6): 1379-1384.
Young WF. Hemoptysis. In: Cline, David,eds. Tintinalli’s Emergency Medicine Manual. 7th Edition. New York : McGraw-Hill Medical; 2011; 473-476.
See Dr. Newman-Toker demonstrate the HINTS exam here
Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009 Nov;40(11):3504-10
Mortality due to loss of airway more so than hemorrhage
Mechanism
MVCs with cervical hyperextension, flexion, rotation during rapid deceleration, direct impact
Strangulation: hanging, choking, clothesline injury (see section on strangulation in this chapter)
Direct blows: assault, sports, falls
Initial Management/Primary Survey
Airway
Evaluate for airway distress (stridor, hoarseness, dysphonia, dyspnea) or impending airway compromise
Early aggressive airway control: low threshold for intubation if unconscious patient, evidence of airway compromise including voice change, dyspnea, neurological changes, or pulmonary edema
Assume a difficult airway
Breathing
Supplemental oxygen
Assess for bilateral breath sounds
Can use bedside US to evaluate for pneumothorax or hemothorax
Circulation
Assess for open wounds, bleeding, hemorrhage
IV access
Disability
Maintain C-spine immobilization
Calculate GCS
Look for seatbelt sign
Secondary Survey
Evaluate for specific signs of vascular, laryngotracheal, pharyngoesophageal, and cervical spinal injuries with inspection, palpation, and auscultation
Perform extremely thorough exam to evaluate for any concomitant injuries (e.g. stab wounds, gunshot wounds, intoxications/ ingestions, etc.)
Types of Injuries
Vascular injury
Overview
Carotid arteries (internal, external, common carotid) and vertebral arteries injured
Mortality rate ~60% for symptomatic blunt cerebral vascular injury
Mechanism
Hyperextension and lateral rotation of the neck, direct blunt force, strangulation, seat belt injuries, and chiropractic manipulation
Morbidity due to intimal dissections, thromboses, pseudoaneurysms, fistulas, and transections
Clinical Features
Most patients are asymptomatic and do not develop focal neurological deficits for days
if Horner’s syndrome, suspect disruption of thoracic sympathetic chain (wraps around carotid artery)
specific screening criteria are used to detect blunt cerebrovascular injury in asymptomatic patients (see below)
Tintinalli 2016
Diagnostic Testing
Gold standard for blunt cerebral vascular injury = MDCTA (multidetector four-vessel CT angiography)
<80% sensitive but 97% specific
Also images aerodigestive tracts and C-spine (unlike angiography)
Followed by Digital Subtraction Angiography (DSA) for positive results or high suspicion
Angiography is invasive, expensive, resource-intensive, and carries a high contrast load
Management
Antithrombotics vs. interventional repair based on BCVI grading system
Given delayed symptoms, consider monitoring patients who are asymptomatic on arrival
Serial exams for worsening dyspnea, dysphonia, stridor, drooling, bruits, focal neuro deficits
Only discharge after ruling out airway threat, neurological deficit, vascular injury, or suicidal/ homicidal ideation
Monitor asymptomatic patients on home anticoagulation in ED for at least 6 hours from trauma to rule out delayed neck hematoma
Social work and/or psychiatry for patients in whom you suspect suicide risk or domestric violence, look for other signs of self harm
Take Home Points
Aggressive early airway management for unconscious patient, evidence of airway compromise including voice change, dyspnea, neurological changes, or pulmonary edema
Victims of blunt cerebral vascular injury may present completely asymptomatic but develop delayed neurological symptoms; close observation and monitoring is recommended especially for patients on home anticoagulation
Remember to evaluate for concomitant injuries
Psychiatric evaluation for all attempted suicides
References
Bromberg, William. et al. Blunt Cerebrovascular Injury Practice Management Guidelines: The Eastern Association for the Surgery of Trauma. J Trauma. 68 (2): 471-7, Feb 2010.
Cothren CC, Moore EE, Biffl WL, et al. Anticoagulation is the gold standard therapy for blunt carotid injuries to reduce stroke rate. Arch Surg. 2004;139:540–545; discussion 545–546.
Joshua AA. Neck Trauma, Blunt, Anterior. In: Schaider J, Barkin R, Hayden S, Wolfe R, Barkin A, Shayne P, Rosen P. Rosen and Barkin’s 5-Minute Emergency Medicine Consult. 5th Edition. Philadelphia, PA: Wolters Kluwer; 2015; 738-739.
Tintinalli, J., Stapczynski, J. Stephan, editor, Ma, O. John, editor, Yealy, Donald M., editor, Meckler, Garth D., editor, & Cline, David, editor. (2018). Tintinalli’s emergency medicine : A comprehensive study guide (9th ed.).
Walls, R., Hockberger, Robert S., editor, & Gausche-Hill, Marianne, editor. (2018). Rosen’s emergency medicine : Concepts and clinical practice (Ninth ed.).
Advanced trauma life support. (2018). 10th ed. Chicago, IL: American College of Surgeons.
As of Oct 15, vaping has been associated with acute lung injury in over 1400 people
33 deaths have been confirmed in 24 states
70+% of those with VALI are young men
A large number of patients are requiring ICU/ intubation/ ECMO
4 main ingredients in solvent
+/- Flavor additives
+/- Nicotine or THC (Tetrahydrocannabinol)
Propylene Glycol (PG)
Vegetable Glycerin (VG)
CDC definition of VALI (Vaping Associated Lung Injury)
Using an e-cigarette (“vaping”) or dabbing* in 90 days prior to symptom onset AND
Pulmonary infiltrate, such as opacities, on plain film chest radiograph or ground-glass opacities on chest CT AND
Absence of pulmonary infection on initial work-up.
No evidence in the medical record of alternative plausible diagnoses (e.g., cardiac, rheumatologic, or neoplastic process).
*Dabbing allows the user to ingest a high concentration of THC. Butane Hash Oil (BHO), an oil or wax-like substance extracted from the marijuana plant, is placed on a “nail” attached to a specialized glass bong called a “rig.” A blow torch is used to heat the wax, which produces a vapor that can then be inhaled to supposedly produce an instantaneous effect.
Pathophysiology
At present, no single compound or ingredient has emerged as the cause, and there may be more than one cause
The only common thread among the cases is that ALL patients reported using e-cig or vaping products
Leading potential toxins:
Vaping products containing THC concentrates: most cases are linked to THC concentrates that were either purchased on the street or from other informal sources (meaning not from a dispensary)
Vitamin E acetate: nutritional supplement safe when ingested or applied to the skin (but likely not when inhaled) has been found in nearly all product samples of NY state cases of suspected VALI
vitamin E acetate is NOT an approved additive at least by NYS Medical Marijuana program
Other potential toxins:
IT CANNOT BE UNDERSTATED that a small percentage of persons w/ VALI have reported exclusive use of nicotine-containing vape products, such as JUUL; as such, we must consider the potential toxicity of standard e-liquid or vape juice
Flavor additives, that exists as chemical aldehydes: irritating and potentially damaging to lung tissue
PG/VG: shown not only to break down to formaldehyde which is a known carcinogen, but also to produce lipoid pneumonia in rat lungs
Some devices are easily manipulated to increase the capacity to produce vapor; increasing these settings may impact heating temperature, metabolic breakdown, and release of microscopic metal particles
Lungs are multifunctional, including serving as an immune organ: lungs cleave proteins of all of the bacteria, viruses and other pathogens we are exposed to and inhale daily
human studies on those that are chronic e-cig users or vapers have revealed that these products are shifting the balance of proteases and antiproteases in our lungs such that the proteases are destroying native lung tissue similar to how traditional cigarettes cause COPD
Many potential reactions:
NEJM article in references: details four radiographic phenotypes essentially reflecting different pathologic changes
Long-term Effects
Long term effects are unknown (some pts have required home oxygen on discharge)
Risk for recurrence or relapse, especially if repeat exposure
Presentation
95% of pts have had pulmonary sxs (cough, cp, dyspnea)
77% of pts have had GI sxs (abd pain, n/v/d)
85% of pts w/ constitutional sxs (f/c, weight loss)
57% w/ hypoxia (O2 < 95%)
Unfortunately auscultation has been unreliable and poorly sensitive
Workup
There is no specific test or marker for dx, so VALI is still considered a dx of exclusion
Labs:
CBC
ESR/CRP (93% w/ elevated ESR)
LFTs (50% w/ transaminitis)
ABG: hypoxia
Imaging:
CXR: typically shows bilateral infiltrates, although not always and there have even been some cases w/ unremarkable chest XR (so high degree of clinical suspicion in any person p/w hypoxia)
CT: ground glass opacities, typically bilaterally
Management
Dispo:
96% of cases required hospitalization
Any pt w/ hypoxia, respiratory distress, or comorbidities
Outpatient only if: no hypoxia or respiratory distress, reliable followup within 48h and good social support (keep in mind that some patients w/ mild symptoms of first presentation deteriorated rapidly within 48h)
Empiric treatments for pneumonia inc abx, antivirals
Steroids (methylpred 60mg q6h, based on how index cases in Illinois were managed)
Case reports have documented improvement
Mechanism: blunting of inflammatory response
Aggressive supportive care
Special Thanks To:
Dr. Larissa Laskowski, DO
Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health, NYC Health + Hospitals/ Bellevue
Carlos WG, Crotty Alexander LE, Gross JE, Dela Cruz CS, Keller JM, Pasnick SP, Jamil S. Vaping-associated Pulmonary Illness (VAPI). Public Health Information Series. Am J Respir Crit Care Med Vol. 200, 13-15, 2019. www.atsjournals.org/doi/pdf/10.1164/rccm.2007P13
Henry TS, Kanne JP, Kilgerman SJ. Images of Vaping-Associated Lung Disease — Correspondence. N Engl J Med. 2019 Oct 10; 381;15.
Siegel DA, Jatlaoui TC, Koumans EH, et al. Update: Interim Guidance for Health Care Providers Evaluating and Caring for Patients with Suspected E-cigarette, or Vaping, Product Use Associated Lung Injury — United States, October 2019. MMWR Morb Mortal Wkly Rep 2019;68:919–927. DOI: http://dx.doi.org/10.15585/mmwr.mm6841e3external icon.
Bacteria enters the joint by hematogenous spread due to absence of basement membrane in synovial space from invasive procedures, contiguous infection (e.g. osteomyelitis, cellulitis), or direct inoculation (e.g. plant thorns, nails)
WBCs migrate into joint → acute inflammatory process → synovial hyperplasia, prevents new cartilage from forming, pressure necrosis on surrounding joint, purulent effusion
Why do we care?
irreversible loss of function in up to 10% & mortality rate as high as 11%
Cartilage destruction can occur in a matter of hours
Complications include bacteremia, sepsis, and endocarditis
Etiology
Risk factors: extremes of age, RA, DJD, IVDA, endocarditis, GC, immunosuppression, trauma, or prosthesis
Consider mycobacterial & fungal in more indolent courses
Presentation
Typically a single, warm, erythematous, tender joint (#1: knee (50% of cases) → hip, shoulder, ankle)
*Any joint can be involved!
IVDA can involve sacroiliac, costochondral, & sternoclavicular joints
Classic teaching: very painful with ROM, but this is not always present!
Joint usually held in position of maximum joint volume
Prosthetic joints may have less pain than expected for a septic joint given changed anatomy and disrupted nerve endings
In 10-20% of cases, can see polyarticular involvement
GC typically monoarticular but commonly polyarticular
Often have fever & separate infection as well (only see fever in ~60% of cases)
Diagnostics
Arthrocentesis:
Gold standard
Tap joint even if acceptable ROM: septic joints can have normal motion so it does not exclude the diagnosis!
Use ultrasound if possible
Relative contraindications: overlying cellulitis (risk of seeding joint) or severe coagulopathies (weigh risk of creation or worsening of iatrogenic hemarthrosis)
Keep in mind that a “dry tap” may occur due to incorrect needle placement, absent/ minimal joint effusion, ort mechanical obstruction
Note: talk to ortho colleagues if prosthesis present prior to performing arthrocentesis
Ortho team may want to perform the arthrocentesis themselves because scar tissue formation and altered anatomic relationships make the procedure more challenging
Usually want to perform washout in OR plus/ minus antibiotic spacer
Send fluid for protein, glucose, cell count with differential, gram stain, culture, and crystals
Often see decreased glucose and elevated protein
The presence of crystals does not rule out septic arthritis
No clear number of synovial WBCs to define septic arthritis, but in general: >30 to 50K/ mm3 synovial WBCs with PMN predominance (>75%) seen in septic arthritis
A 2011 meta-analysis suggests +LRs of 4.7 (95% CI = 2.5 to 8.5) and +LR of 13.2 (95% CI = 3.6 to 51.1) for a sWBC count of >50L × 109 or >100K, respectively
Use the synovial WBC count plus the whole clinical picture to rule in or out the diagnosis of septic arthritis (do not use the synovial WBC in isolation)
Different threshold for prosthetic joints: WBC > 1100 or >64% PMNs = septic arthritis
Gram stains only identify causative organisms 1/3 of the time
Culture negative arthrocentesis can be seen in cases where abx have been given prior to arthrocentesis, or in TB/ brucella/ nocardia/ other indolent organisms like fungi
Labs:
No studies have demonstrated an acceptable sensitivity or overall diagnostic accuracy of peripheral WBC count for SA, but usually see leukocytosis with left shift
ESR and CRP are reasonably sensitive but there is no cutoff that significantly increases or decreases the pretest probability
UA, urine cultures, blood cultures: send even if no fever
Blood cultures are positive in 50-70% of nonGC SA
If GC suspected, do GC NAAT from throat/ rectal/ urethral/ cervical discharge
Imaging:
XRs: effusion, baseline status of joint, contiguous osteomyelitis, fractures, foreign body
US: effusion
CT, MRI: not really used in ED
Differential
Viral arthritis
RA
gout/ pseudogout
HIV associated arthritis
Reactive arthritis
Lyme
Osteo
Septic bursitis
Trauma
Treatment
Septic arthritis is an orthopedic emergency!
Needs IV abx + often washout of the joint
Hold abx as much as possible prior to tap unless pt is unstable or tap cannot be performed easily
Initiate empiric IV antibiotic therapy prior to definitive cultures based
Transition to organism-specific antibiotic therapy once culture sensitivities result
Start empiric abx based on gram stain if available (in non-=GC SA, grain stain is positive in 50% of cases), age group, & risk factors
Admit all patients with suspected septic arthritis until SA is ruled out, abx, monitoring, likely operative intervention
Take-Home Points
Patients may present with either a single affected joint or polyarticular; they may or may not have a fever
Have a high index of suspicion for SA, and a low threshold to tap: pts do not necessarily present w/ “classic” findings and it is difficult to distinguish SA from crystal arthropathy
ESR, CRP, serum WBC are not definitive diagnostic tools for septic arthritis
There is no exact cutoff for synovial WBCs for diagnosis: use whole clinical picture & keep 50K in mind for native joints, and >1100 for prostheses
Treat with empiric abx after tap then narrow accordingly, & admit all patients with septic arthritis
Involve your ortho colleagues early especially for prosthesis
Jones D, Clements C. Physical exam and bloodwork do not adequately differentiate infectious from inflammatory arthritis. In: Mattu A, Chanmugam A, Swadron S, Woolridge D, Winters M. Avoiding Common Errors in the Emergency Department. 2nd Edition. Philadelphia, PA: Wolters Kluwer; 2017; 412-414.
Kazzi A, Zaghrini E. Septic Arthritis. In: Schaider J, Barkin R, Hayden S, Wolfe R, Barkin A, Shayne P, Rosen P. Rosen and Barkin’s 5-Minute Emergency Medicine Consult. 5th Edition. Philadelphia, PA: Wolters Kluwer; 2015; 102-103.
Osmon D, Berbari E, Berendt A, Lew D, Zimmerli W, Steckelberg J, Rao N, Hanssen A, Wilson W.
Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America, Clinical Infectious Diseases, Volume 56, Issue 1, 1 January 2013, Pages e1–e25, https://doi.org/10.1093/cid/cis803
Mlynarek C, Sullivan A. Arthrocentesis Tips. In: Mattu A, Chanmugam A, Swadron S, Woolridge D, Winters M. Avoiding Common Errors in the Emergency Department. 2nd Edition. Philadelphia, PA: Wolters Kluwer; 2017; 684-686.
Purcell D, Terry B, Sharp B. Joint Arthrocentesis. In: Purcell D, Chinai S, Allen B, Davenport M. Emergency Orthopedics Handbook. 1st Edition. Cham, Switzerland: Springer; 2019; 87-104.
The most common type of seizure in children under 5 years of age
Occur in 2-5% of children
In children with a fever, aged 6 months to 5 years of age, and without a CNS infection
Risk Factors
4 times more likely to have a febrile seizure if parent had one
Also increase in risk if siblings or nieces / nephews had one
Common associated infections
Human Herpesvirus 6
Human Herpesvirus 7
Influenza A & B
Simple Febrile Seizure
Generalized tonic-clonic activity lasting less than 15 minutes in a child 6 months to 5 years of age
Complex Febrile Seizure
Lasts longer than 15 minutes, occurs in a child outside of this age range, are focal, or that recur within a 24-hour period.
Diagnostics / Workup
Gather thorough history and perform thorough physical exam
Most cases will not require labs, imaging or EEG
If e/o meningitis, perform LP
AAP suggests considering LP in:
Children 6-12 months who are not immunized for H flu type B or strep pneumo
Children who had been on antibiotics
For complex seizures, clinician may have a lower threshold for obtaining labs
Hyponatremia is more common in this group than in the general population.
LPs are more commonly done by providers, but these are low yield with one study showing bacterial meningitis being diagnosed in just 0.9% (Kimia 2010), all of whom did not have a normal exam or negative cultures.
Neuroimaging is also exceedingly low yield if the patient returns to baseline (Teng 2006)
One study that showed that the duration of complex febrile seizure, being greater than 30 minutes, was associated with a higher incidence of bacterial meningitis. (Chin 2005)
Of they have history and exam concerning for meningitis, they should get an LP
If they look dehydrated or edematous, you would have more of a reason to get a chemistry
Treatment
Benzodiazepine if seizure lasted for >5 minutes, either IV or IN
Supportive care
Tylenol or motrin if febrile
Fluids if signs of dehydration
Antipyretics “around the clock”
A majority of data show no benefit in preventing recurrence of seizure
One study (Murata 2018) found that giving tylenol q6h at 10 mg/kg for the first 24 hours following the initial seizure decreased the rate of recurrence when compared to children who did not receive antipyretics.
NNT here was 7
Questionable whether we can generalize these findings from a single ED in Japan.
No role for antiepileptics
Prognosis
High rate of recurrence (~1/3) within 1 year of initial seizure
Risk increases for
Younger age at which they had initial seizure
Lower temperature at which they had seizure
If initial febrile seizure was prolonged, more likely that the next will be prolonged
1-2% develop epilepsy for simple febrile seizure, slightly above risk of general population
5-10% develop epilepsy for complex febrile seizure
Follow up with PMD
Generally, peds neuro follow up is not necessary
References
Chin RF, Neville BG, Scott RC. Meningitis is a common cause of convulsive status epilepticus with fever. Arch Dis Child. 2005;90(1):66-9.
Kimia A, Ben-Joseph EP, Rudloe T, Capraro A, Sarco D, Hummel D, et al. Yield of lumbar puncture among children who present with their first complex febrile seizure. Pediatrics. 2010;126(1):62-9.
Murata S, Okasora K, Tanabe T, Ogino M, Yamazaki S, Oba C, et al. Acetaminophen and Febrile Seizure Recurrences During the Same Fever Episode. Pediatrics. 2018;142(5).
Patel N, Ram D, Swiderska N, Mewasingh LD, Newton RW, Offringa M. Febrile seizures. BMJ. 2015;351:h4240.
Pavlidou E, Panteliadis C. Prognostic factors for subsequent epilepsy in children with febrile seizures. Epilepsia. 2013;54(12):2101-7.
Stapczynski, J. S., & Tintinalli, J. E. (2016). Tintinalli’s emergency medicine: A comprehensive study guide, 8th Edition. New York: McGraw-Hill Education.
Subcommittee on Febrile S, American Academy of P. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011;127(2):389-94.
Teng D, Dayan P, Tyler S, Hauser WA, Chan S, Leary L, et al. Risk of intracranial pathologic conditions requiring emergency intervention after a first complex febrile seizure episode among children. Pediatrics. 2006;117(2):304-8.
Warden CR, Zibulewsky J, Mace S, Gold C, Gausche-Hill M. Evaluation and management of febrile seizures in the out-of-hospital and emergency department settings. Ann Emerg Med. 2003;41(2):215-22.
A special thanks to our editors:
Michael A. Mojica, MD
Director, Pediatric Emergency Medicine Fellowship Bellevue Hospital Center
Christie M. Gutierrez, MD
Pediatric Emergency Medicine Fellow Columbia University Medical Center Morgan Stanley Children’s Hospital New York Presbyterian
Endemic in Northeast, Upper Midwest, northwest California
80% to 90% in summer months
Pathophysiology
Ixodes tick (deer tick) has a 3-stage life cycle (larvae, nymph, adult) & takes 1 blood meal per stage
Deer tick feeds on an infected wild animal (infected with spirochete Borrelia burgodrferi) then bites humans
On humans, they typically move until they encounter resistance (e.g. hairline, waistband, elastic, skin fold). It takes 24-48 hrs for B. Burgdorferi to move from the tick to the host
Pathogenesis: organism induced local inflammation, cytokine release, autoimmunity
No person to person transmission
Clinical Presentation
Stage 1: Early
Symptom onset few days to a month after tick bite
Erythema migrans rash: bulls eye rash seen in more than 90% of patients with Lyme disease (Irregular expanding annular lesion(s))
LP when meningeal signs (CSF: pleocytosis, elevated protein, CSF spirochete ABs). LP function is more to rule out other etiologies of meningitis rather than diagnose Lyme meningitis given that lyme PCR and lyme Ab index are not very accurate.
Serological Testing
Serological testing is not always warranted because of the very high incidence of false positive results
Serologies are not useful in acute phase (<30 days of infection) because they are negative; it takes several weeks to develop enough antibodies for either test below (ELISA or Western Blot)
Acute Lyme is a clinical diagnosis and does not need laboratory testing, especially in endemic areas such as NY
If pretest probability is high (symptoms consistent with Lyme + epidemiological background), say patients with CN palsy, meningitis, carditis, or migratory large joint arthritis, then serologies can be very helpful
Do not test if patients in endemic areas with potential tick exposure present with EM — just treat with antibiotics
Do not test if patients in endemic areas present with no history of tick exposure or only nonspecific symptoms
Test if you have high suspicion of lyme without EM
PCR is highly specific and sensitive but not available for routine use. There are two tests you need to use together:
1) ELISA: this detects antibodies to lyme bacteria (borrelia burgdorferi) in your blood, BUT it can’t distinguish between borrelia and similar bacteria (even sometimes normal flora that lives in you). In addition, IgM response takes 1-2 weeks while IgG response takes 2-4 weeks.
If ELISA is positive or equivocal, then you move onto the:
2) Western blot test: this looks for antibodies not to the whole organism, but to the basic building blocks of the lyme bacteria — the individual proteins, BUT many types of bacteria use the same building blocks. So the CDC says that the Western Blot test must detect IgG antibodies to 5 out of the 10 proteins.
Two-tiered testing has sensitivity between 70-100% and specificity ~95% in late stages
Interpretation of Lyme serologies should be done by an ID specialist because they can be confusing and can lead to wrong conclusions if unfamiliar with them
NYC is an endemic region where 5% of the population can have a positive without symptoms!
If somebody who HAD Lyme disease but successfully treated it with doxycycline tested themselves years later, they could still have the antibodies and therefore it would look like they still had Lyme disease (despite being cured)
Positive serology or previous Lyme disease not ensure protective immunity
Other tests:
Arthrocentesis for acute arthritis: elevated cryoglobulin
XRs: may show soft tissue, cartilaginous, osseous changes
Remember that doxycycline covers anaplasmosis and lyme but not babesiosis, which requires Atovaquone
Rheumatic fever (usually presents with erythema marginatum rash, valvular involvement rather than heart block, TM joint arthritis)
Viral meningitis
Septic arthritis
Syphilis
Parvovirus B19
Infectious endocarditis
Juvenile rheumatoid arthritis
Reiter syndrome
Brown recluse spider bite
Fibromyalgia
Chronic fatigue syndrome
Treatment
Remove tick: disinfect site then with blunt instrument, grasp tick proximal to skin and pull upward with gentle constant traction. Mouthparts will release after about a minute. If residual mouthparts are left in skin, leave them alone to avoid infection (they will extrude from skin naturally over time). Since ticks that have not attached or are moving on the skin cannot transmit Lyme, they can just be brushed off.
NS IVF bolus, supportive care
Cardiac monitoring, temporary pacemaker for heart block
Beware Jarisch Herxheimer reaction: worsening of sx a few hours after treatment initiated
Aspirin for cardiac involvement, NSAIDs for arthralgias/ arthritis
Prophylaxis:
Per the IDSA, give a single dose of 200 mg PO doxycycline to patients who meet all of the following criteria:
Deer tick has been attached for 36 hours or more (the rationale for time of attachment relates to the fact that the spirochetes live in the tick’s gut so they need a long time to multiply and travel to the salivary glands (event that’s triggered by a blood meal) and later overcome the salivary gland (which only a few do) and finally reach the patient’ skin
Prophylaxis can be provided within 72 hours of tick removal
Local rate of B. Burgdorferi infection in ticks exceeds 20% (in the northeast USA, the prevalence of infected ticks is between 15-20%)
Doxycycline can be used (children >8 years old, non-pregnant females)
A 2001 study examined doxycycline vs placebo prophylaxis. A single dose of 200 mg of oral doxycycline or placebo was given to persons presenting within 72 hours of removal of an I scapularis tick. One of 235 persons in the doxycycline group developed erythema migrans (EM) versus 8 of 247 in the placebo group, for treatment efficacy of 87% (95% CI, 25%–98%; P<0.04) (9).
Reasonable alternative strategy: monitor for EM or other signs of infection then initiate treatment if they develop Lyme disease (excellent outcomes in patients treated during early EM stage of disease)
Antibiotics:
Antibiotics can speed resolution of arthritis and cardiac conduction delays, but not necessarily facial palsy
Doxycycline has the best bioavailability and CNS penetration
Always check with your ID colleagues to determine appropriate duration of treatment in more serious cases of Lyme disease
Stage 1:
Amoxicillin (500 mg PO TID) or cefuroxime (500 mg PO BID) or doxycycline (100 mg PO BID; > 8 years old & not pregnant) x 21 days; azithromycin (500 mg PO qday x 14-21 days)
IV therapy in pregnant patients
Stage 2:
PO antibiotics for isolated Bell palsy and mild involvement
Amoxicillin with probenecid (500 mg PO TID) x 30 days or doxycycline (100 mg PO BID; > 8 years old & not pregnant) x 10-21 days
IV ceftriaxone (2 g IV qday) x 14-21 days, or penicillin G (20-24 million units IV q4-6h x 14-28 days) for meningitis, carditis, severe arthritis
Stage 3:
Penicillin G (20-24 million units IV q4-6h) x 14-21 days or ceftriaxone (2 g IV qday x 14-28 days)
Dispotition
Admit unstable or sick patients, those with meningoencephalitis, & carditis (telemetry/ ICU admission)
DC patients treated with PO therapy
Future prevention strategies: wear long pants & shirts, light-colored clothing (easier to spot crawling ticks), tuck pants into socks, DEET spray, clothing impregnated with permethrin
Hilton E, DeVoti J,, Benach JL, Halluska ML, White DJ, Paxton H, Dumler JS. Seroprevalence and seroconversion for tick-borne diseases in a high-risk population in the northeast United States. Am J Med. 1999 Apr;106(4):404-9.
Hu LT. Lyme Disease. Ann Intern Med. 2016;164:ITC65-ITC80. Doi: 10.7326/AITC201605030
Lee, M. Lyme Disease. Rosen and Barkin’s 5-Minute Emergency Medicine Consult. 2015; 664-665.
Nadelman RB, Nowakowski J, Fish D et al., Tick Bite Study Group. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med. 2001;345:79-84.
Sanders, L. (2009). Every patient tells a story: Medical mysteries and the art of diagnosis.
A special thanks to our Infectious Diseases Editor:
In 2017, there were 219 million cases and 435,000 people deaths from malaria
Five species: Falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi.
Falciparum, Vivax and Knowlesi can be fatal
History of recent travel to Africa (69% of cases in US), particularly to west-Africa should raise suspicion for malaria
Clinical Manifestations
Average incubation period for Falciparum is 12 days
95% will develop symptoms within 1 month
Clinical findings with high likelihood ratios include periodic fevers, jaundice, splenomegaly, pallor.
Can also have vomiting, headache, chills, abdominal pain, cough, and diarrhea
Severe malaria has a mortality of 5% to 30%, even with therapy
Diagnostic criteria for severe malaria:
Ashley 2018
Most common manifestations of severe malaria affect the brain, lungs, and kidneys
Patients with cerebral malaria can present encephalopathic or comatose, some severe enough to exhibit extensor posturing, or seizures
Can have acute lung injury with a quarter of these patients progressing to ARDS
Can have AKI from ATN and resultant acidosis
Labs may be unremarkable but watch for anemia and thrombocytopenia
Hgb <5 has an OR = 4.9 for death
Severe thrombocytopenia has an OR = 2.8
Anemia + Thrombocytopenia has an OR = 13.8 (Lampah 2015, PMID 25170106)
Watch for hypoglycemia
Be mindful of co-infection with salmonella and HIV
Obtain BCx, cover with ceftriaxone
Diagnosis
Blood smear
Thick smear to increase sensitivity for detecting parasites
Thin smear for quantifying parasitemia and species
The first smear is positive in over 90% of cases, but if suspicion is high, it has to be repeated BID for 2-3 days for proper exclusion of malaria (CDC 2019)
Management
For uncomplicated, non-severe cases, most patients with falciparum should be admitted, especially those with no prior exposure to malaria parasites
Important to note that when they take this, ensure they take with milk or food containing fat to enhance absorption
Severe Malaria
Resuscitative efforts directed at affected organ
Can deteriorate rapidly
Initiate IV Artesunate if high level of suspicion
Requires call to CDC: CDC Malaria Hotline: (770) 488-7788 or (855) 856-4713 (toll-free) Monday–Friday 9am–5pm EST – (770) 488-7100 after hours, weekends, and holidays
Benzodiazepines for seizures
Be judicious with fluids as this can precipitate pulmonary edema and cerebral edema
This is going to be a diagnosis that is mainly made through a thorough history, and pay particular attention to those with recent travel to West-Africa
The incubation period for falciparum is 12 days, but there is a range of weeks and we should consider Malaria when consistent symptoms develop within 1 month of travel to an endemic area
Typical signs and symptoms for uncomplicated malaria are periodic fevers, jaundice, pallor
Be mindful of end organ involvement, such as cerebral edema, ATN, and pulmonary edema; these cases are considered to be severe and treated differently than uncomplicated malaria
Uncomplicated cases should get Malarone or Coartem
Severe cases require IV Artesunate
Be judicious with your fluid resuscitation as this can harm our patients
References
Centers for Disease Control and Prevention. CDC Parasites – Malaria. 2019 https://www.cdc.gov/parasites/malaria/index.html (7 July 2019, date last accessed)
Ashley EA, Pyae Phyo A, Woodrow CJ. Malaria. Lancet. 2018;391(10130):1608-21.
Hanson JP, Lam SW, Mohanty S, Alam S, Pattnaik R, Mahanta KC, et al. Fluid resuscitation of adults with severe falciparum malaria: effects on Acid-base status, renal function, and extravascular lung water. Crit Care Med. 2013;41(4):972-81.
Lampah DA, Yeo TW, Malloy M, Kenangalem E, Douglas NM, Ronaldo D, et al. Severe malarial thrombocytopenia: a risk factor for mortality in Papua, Indonesia. J Infect Dis. 2015;211(4):623-34.
Lokken KL, Stull-Lane AR, Poels K, Tsolis RM. Malaria Parasite-Mediated Alteration of Macrophage Function and Increased Iron Availability Predispose to Disseminated Nontyphoidal Salmonella Infection. Infect Immun. 2018;86(9).
Maitland K, Kiguli S, Opoka RO, Engoru C, Olupot-Olupot P, Akech SO, et al. Mortality after fluid bolus in African children with severe infection. N Engl J Med. 2011;364(26):2483-95.
Park SE, Pak GD, Aaby P, Adu-Sarkodie Y, Ali M, Aseffa A, et al. The Relationship Between Invasive Nontyphoidal Salmonella Disease, Other Bacterial Bloodstream Infections, and Malaria in Sub-Saharan Africa. Clin Infect Dis. 2016;62 Suppl 1:S23-31.
Tintanelli, Judith E., et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. Eighth edition. New York: McGraw-Hill Education, 2016: p.1070-1077
World Health Organization. Guidelines for the treatment of malaria. Third edition
The most common infection seen in pediatrics and the most common reason these kids receive antibiotics
The release of the PCV (pneumococcal conjugate vaccine), or Prevnar vaccine, has made a big difference since its release in 2000 (Marom 2014)
This, along with more stringent criteria for what we are calling AOM, has led to a significant decrease in the number of cases seen since then
29% reduction in AOM caused by all pneumococcal serotypes among children who received PCV7 before 24 months of age
The peak incidence is between 6 and 18 months of age
Risk factors: winter season, genetic predisposition, day care, low socioeconomic status, males, reduced duration of or no breast feeding, and exposure to tobacco smoke.
The predominant organisms: Streptococcus pneumoniae, non-typable Haemophilus influenzae (NTHi), and Moraxella catarrhalis.
Prevalence rates of infections due to Streptococcus pneumoniae are declining due to widespread use of the Prevnar vaccine while the proportion of Moraxella and NTHi infection increases with NTHi now the most common causative bacterium
Strep pneumo is associated with more severe illness, like worse fevers, otalgia and also increased incidence of complications like mastoiditis.
Diagnosis
The diagnosis of acute otitis media is a clinical one without a gold standard in the ED (tympanocentesis)
Ear pain (+LR 3.0-7.3), or in the preverbal child, ear-tugging or rubbing is going to be the most common symptom but far from universally present in children. Parents may also report fevers, excessive crying, decreased activity, and difficulty sleeping.
Challenging especially in the younger patient, whose symptoms may be non-specific and exam is difficult
Important to keep in mind that otitis media with effusion, which does not require antibiotics, can masquerade as AOM
AAP: Diagnosis of Acute Otitis Media (2013)*
In 2013, the AAP came out with a paper to help guide the diagnosis of AOM
Moderate-Severe bulging of the tympanic membrane or new-onset otorrhea not due to acute otitis externa (grade B)
The presence of bulging is a specific sign and will help us distinguish between AOM and OME, the latter has opacification of the tympanic membrane or air-fluid level without bulging (Shaikh 2012, with algorithm)
Bulging of the TM is the most important feature and one systematic review found that its presence had an adjusted LR of 51 (Rothman 2003)
Classic triad is bulging along with impaired mobility and redness or cloudiness of TM
Mild bulging of the tympanic membrane AND (grade C)
Recent onset (48hrs) Ear pain (verbal child) Holding, tugging, rubbing of the ear (non-verbal child) OR
Intense erythema of the tympanic membrane
* The diagnosis should not be made in the absence of a middle ear effusion (grade B)
Treatment Options
A strategy of “watchful waiting” in which children with acute otitis media are not immediately treated with antibiotic therapy, has been endorsed by the American Academy of Pediatrics.
Who gets antibiotics?
Depends on age, temperature, duration of otalgia, laterality / otorrhea, and access to follow up
Get’s antibiotics:
<6 months: Treat
6 months to 2 years: Treat
Exception, AAP permits initial observation: unilateral AOM with mild symptoms (mild ear pain, <48h, T <102.2)
But know that there is a high rate of treatment failure (Hoberman 2013)
>2: Treat
Unless they have mild symptoms and it’s unilateral, you can observe for 48-72 hours
Why do we give antibiotics?
Demonstrated reduction in pain, TM perforations, contralateral episodes of AOM
They are no walk in the park, with increased adverse events (vomiting, diarrhea, rash)
Two well-designed clinical trials (2011) randomized approximately 600 children meeting strict diagnostic criteria for acute otitis media to receive Augmentin or placebo. These studies demonstrated a significant reduction in symptom burden and clinical failures in those who received antibiotics.
The authors conclude that those patients with a clear diagnosis of acute otitis media would benefit from antibiotic therapy
AAP AOM Treatment Algorithm
Antibiotic Selection
High-dose amoxicillin in most (for now)
Amoxicillin should not be used if the patient has received Amoxicillin in the past 30 days, has concomitant purulent conjunctivitis (likely H flu) or is allergic to penicillin.
beta lactamase resistant antibiotic should be used.
Amoxicillin clavulanate or 2nd or 3rd generation cephalosporins (including intramuscular ceftriaxone).
Patients with a history of type 1 hypersensitivity reactions to penicillin should be treated macrolides.
Studies on duration of therapy have shown better results with 10-day duration in children younger than 2 years and suggest improved efficacy in those 2-5 years.
For patients older than 5 years, shorter course therapy (5-7 days) can be utilized.
Pain Control
Motrin and APAP may have benefit with otalgia reduction
Other
Decongestants and antihistamines have been shown to not benefit patients in terms of duration of symptoms or complication rate. Not surprisingly, these agents increase the side-effects experienced by patients.
Follow up
If you chose to observe, let the parents know to return to ED or f/u with their provider in 48-72 hours if they symptoms do not improve. Providing a prescription to parents with clear instructions on when to fill it is also an acceptable option. Strict return precautions should be given if patient develops meningismus or facial nerve palsy.
If antibiotics were initiated, and there isn’t improvement in 2-3 days, the diagnosis of AOM should be revisited and, if still suspected, we have to consider that the causative bug is resistant to the prescribed antibiotic.
These patients should RTED or f/u with their pediatrician for escalation of care
Amoxicillin → Augmentin
Augmentin → Ceftriaxone IM
Macrolide → no clear antimicrobial agent, consult pediatric ENT
If antibiotics are initiated with resolution of symptoms, the patient should f/u in 2-3 months to ensure resolution of the middle ear effusion and ensure that there is no associated conductive hearing loss
References:
Coker TR, Chan LS, Newberry SJ, Limbos MA, Suttorp MJ, Shekelle PG, et al. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review. JAMA. 2010;304(19):2161-9.
Hoberman A, Ruohola A, Shaikh N, Tahtinen PA, Paradise JL. Acute otitis media in children younger than 2 years. JAMA Pediatr. 2013;167(12):1171-2.
Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-99.
Marom T, Tan A, Wilkinson GS, Pierson KS, Freeman JL, Chonmaitree T. Trends in otitis media-related health care use in the United States, 2001-2011. JAMA Pediatr. 2014;168(1):68-75.
Rothman R, Owens T, Simel DL. Does this child have acute otitis media? JAMA. 2003;290(12):1633-40.
Shaikh N, Hoberman A, Rockette HE, Kurs-Lasky M. Development of an algorithm for the diagnosis of otitis media. Acad Pediatr. 2012;12(3):214-8.
Venekamp RP, Sanders S, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2013(1):CD000219.
See our core article on the topic by Dr. Deborah Levine and Dr. Michael Mojica here
A special thanks to our editors:
Michael A. Mojica, MD
Director, Pediatric Emergency Medicine Fellowship Bellevue Hospital Center
Christie M. Gutierrez, MD
Pediatric Emergency Medicine Fellow Columbia University Medical Center Morgan Stanley Children’s Hospital New York Presbyterian
Acute stress fractures are typically not detected on the standard 3 views; therefore, repeat XRs 10-14d after onset of sx (may see radiolucent reabsorption gap around fracture)
For more complex mid foot trauma, consider CT to r/o Lisfranc
Treatment:
Consider classification of fracture, patient demographics & activity level when deciding on treatment
Tertiary care centers that have access to Orthopedics/Podiatry services
Consider consultation for “true” Jones fractures, as some cases may be operatively managed acutely and/or for expedited follow-up to be arranged
If working in community/rural locations: other than patients that present with “open” injuries, concerns for compartment syndrome (almost never), and “high-end”/professional athletes, there are generally no other circumstances that would require expedited transfer to a tertiary care center for immediate further evaluation.
Less favorable outcomes associated with certain patient factors: female gender, DM, obesity
Surgical:
Different modalities of surgery:
Intramedullary screw
Bone graft
Closed reduction and fixation with K-wire
ORIF (all +/- need for bone graft)
Surgery likely recommended for displacement >10 degrees of plantar angulation or 3-4 mm of translation in any plane
Indications for OR:
Neck and shaft fractures with >10 degrees plantar angulation or 3mm of displacement in any plane with insufficient closed reduction
Avulsion fractures (zone one) with >3 mm of displacement or comminuted
Zone two fractures: displaced zone two fractures require operative management. For acute non displaced Jones fractures, consider early intramedullary screw fixation in athletes (studies have shown return to sport ~ 8 weeks, weight bearing within 1-2 weeks)
Zone three fractures (diaphyseal stress fractures) in athletes
Nonoperative:
All non displaced fifth metatarsal fractures can be treated non operatively
Non displaced zone 1 fractures: protected weight bearing/ symptomatic care in short leg walking cast, air-boot, posterior splint, or compression wrap/ rigid shoe until discomfort subsides
Zone 2 and 3 fractures are more complex because they often result in prolonged healing time and potential for delayed/ nonunion
Acute zone 2 fractures: nonweightbearing in short leg cast for 6-8 weeks
Acute zone 3 fractures: nonweightbearing in short leg cast for up to 20 weeks
With respect to athletes: repeat fracture after surgical treatment of Jones fracture can occur after healing and screw removal; thus it is recommended that the screw be left in until the end of the athlete’s career
References:
Bowes J, Buckley R. Fifth metatarsal fractures and current treatment. World J Orthop. 2016;7(12):793–800. Published 2016 Dec 18. doi:10.5312/wjo.v7.i12.793
Petrisor BA, Ekrol I, Court-Brown C. The epidemiology of metatarsal fractures. Foot Ankle Int. 2006 Mar; 27(3): 172-4.
Tham W, Sng S, Lum YM, Chee YH. A Look Back in Time: Sir Robert Jones, ‘Father of Modern Orthopaedics’. Malays Orthop J. 2014;8(3):37–41. doi:10.5704/MOJ.1411.009
Thomas JL, Davis BC. Three-wire fixation technique for displaced fifth metatarsal base fractures. J Foot Ankle Surg. 2011;50:776–779.
______________________
LISFRANC SHOW NOTES:
Intro:
Can’t miss diagnoses: needs stat ortho
20% miss rate
Can be dislocation, fracture, fracture dislocation, or ligamentous injury
Jacques Lisfranc in Napoleonic Wars: performed transmetatarsal amputation for midfoot gangrene
Anatomy:
Lisfranc ligament: 3 ligaments that run from the base of the second metatarsal to the medial cuneiform bone. Helps attach the forefoot to the midfoot bones
If ligament complex gets disrupted, can end up with chronic deformity and disability
Injury definitions:
Dislocation: widening between base of 1st and 2nd metatarsal, or between cuneiforms
Fracture dislocation: associated fracture, most commonly at the base of the proximal second metatarsal
Physical Exam:
Pain and swelling in midfoot
Pain elicited with passive abduction and pronation of the midfoot while holding heel steady
Plantar ecchymosis
r/o compartment syndrome
Feel for DP pulse!
Diagnosis:
XRs: AP, lateral, oblique, stress views with weight bearing
Watch out for “fleck sign”
Consider CT if pt cannot bear weight, or even if XR negative and high suspicion
Debriefing after a clinical case in the ED is a way to have an interprofessional, reflective conversation with a focus on improving for the next patient. We can debrief routine cases, challenging cases, or even cases that go well.
Follow a structure when leading a debrief.
The prebrief sets ground rules and informs the team that the debrief is optional and will only take 3-5 minutes.
Introduce names and roles
Then give a one-liner about what happened in the case, followed by a plus/ delta: address what went well and why, then how to improve
Finally, wrap up with take home points
Pitfalls to watch out for in clinical debriefing include:
Avoid siloing or alienating any learners. Learn from all your colleagues on your team- it’s less about medicine and more about interprofessional and systems issues
Don’t pick on individual performance. It’s not about shaming- it’s about improving patient care
Avoid “guess what I’m thinking” questions; ask real questions
Proceed with caution in order to dampen or avoid psychological trauma and second victim syndrome. The learner may ask “was this my fault?”; we never want a learner to feel this way. Ask, what systems supported or did not support you today? Talk about what happened. Avoid shame and blame.
Have the right values and do it for the right reasons.
Dr. Shannon McNamara completed residency in Emergency Medicine at Temple University hospital and fellowship in Medical Simulation at Mount Sinai St. Lukes-Roosevelt. She now is the Director of the Simulation Division in the NYU Department of Emergency Medicine. She’s thrilled to have somehow made a career out of teaching people to talk about their feelings using big computers shaped like people.
Dr. Jessica Leifer attended NYU for medical school and completed her residency training in emergency medicine at Mount Sinai St. Luke’s-Roosevelt. She completed a fellowship in medical simulation at the Mount Sinai Hospital. She is now simulation faculty in the NYU department of Emergency Medicine. Her academic interests include using simulation for patient safety, operations, and improving teamwork.
Croup is a viral infection starts in the nasal and pharyngeal mucosa but spreads to the larynx and trachea
Subglottic narrowing from inflammation
Dynamic obstruction
Barking cough
Inspiratory stridor
Causes:
Parainfluenza virus (most common)
Rhinovirus
Enterovirus
RSV
Rarely: Influenza, Measles
Age range: 6 months to 36 months
Seasonal component with high prevalence in fall and early winter
Differential
Bacterial tracheitis
Acute epiglottitis
Inhaled FB
Retropharyngeal abscess
Anaphylaxis
Presentation & Diagnosis
Classically a prodrome of nonspecific symptoms for 1-3 days with low grade fevers, congestion, runny nose.
Symptoms reach peak severity on the 4th day
“Steeple sign” on Xray (subglottic narrowing) present in only 50% of patients with croup
Assess air entry, skin color, level of consciousness, for tachypnea, if there are retractions / nasal flaring (if present at rest or with agitation) & coughing
Occasional barking cough, but no stridor at rest and mild to no retractions
Tx: Single dose of dex
Has been shown to improve severity and duration of symptoms
Route is not particularly important, whether it’s PO, IV or IM
Chosen route should aim to minimize agitation in the patient that might worsen their condition
May be managed at with supportive care
Humidifiers (NB: there isn’t good evidence supporting the use of humidifiers)
Antipyretics
PO fluids
Moderate Group
May have stridor at rest, mild-moderate retractions but no AMS and will not be in distress.
Tx: Dex + Racemic Epinephrine
Racemic epinpehrine will start to work in about 10 minutes
Effects last for more than an hour
Severe group
Receives the same initial therapy as the moderate group with dex and race epi
Pts with worrisome signs: stridor at rest, marked retraction, cyanosis and/or lethargy
Heliox (a combinations of 70-80% helium + 20-30% oxygen) may be attempted
There is limited evidence to support the role of heliox in croup,
NB: Pt may require higher levels of oxygen than the 20-30% mixture may provide
Intubation
Anticipate edema narrowing the airway
Consider starting with a tube that is 0.5 to 1 mm smaller than size typically used
Disposition:
Patients without stridor at rest or respiratory distress can be generally discharged from the ED
If epinephrine is given, patients should be monitored for 2-4 hours for reemergence of symptoms as the medication wears off
Take Home Points
Croup usually affects children within the age range of 6 months to 36 months with the most common cause being parainfluenza virus
Given the symptom overlap, we must consider more concerning diagnoses, including bacterial tracheitis, in these patients, especially if they are ill appearing or traditional therapies are ineffective
All patients benefit from a one-time dose of dexamethasone and, if racemic epinephrine is given, the patient should be observed for at least 3 hours
If intubation is required, anticipate a narrowed airway
Rash with dysuria should raise concern for SJS with associated urethritis
Dysuria present in a majority of cases
SJS is a mucocutaneous reaction caused by Type IV hypersensitivity
Cytotoxic t-lymphocytes apoptose keratinocytes → blistering, bullae formation, and sloughing of the detached skin
Disease spectrum
SJS = <10% TBSA
TEN = >30% TBSA
SJS/ TEN Overlap = 10-30% TBSA
Incidence is estimated at around 9 per 1 million people in the US
Mortality is 10% for SJS and 30-50% for TEN
Mainly 2/2 sepsis and end organ dysfunction.
SJS can occur even without a precipitating medication
Infection can set it off especially in patients with risk factors including HIV, lupus, underlying malignancy, and genetic factors
SATAN for the most common drugs
Sulfa, Allopurinol, Tetracyclines, Anticonvulsants, and NSAIDS
Anti-epileptics include carbamazepine, lamictal, phenobarb, and phenytoin
Can have a curious course
Hypersensitivity reaction can develop while taking medication, or even one to four weeks after exposure
In pediatric population, mycoplasma pneumonia and herpes simplex have been identified as precipitating infections
Patients often have a prodrome 1-3 days prior to the skin lesions appearing
May complain of fever, myalgias, headaches, URI symptoms, and malaise
Rash may be the sole complaint
Starts as dark purple or erythematous lesions with purpuric centers that progress to bullae
Skin surrounding the lesions detaches from the dermis with just light pressure (Nikolsky Sign)
Up to 95% of patients will have mucous membrane lesions
~85% will have conjunctival lesions
Symptoms: Burning or itching eyes, a cough or sore throat, pain with eating, pain with urinating or defecating
Source: JAMA Dermatol. 2017
Differential Diagnosis: SSSS, autoimmune bullous diseases, bullous fixed drug eruption, erythema multiforme, thermal burns, phototoxic reactions, and TSS
SJS is a clinical diagnosis
Basic workup: CBC, chemistry panel, LFTs, and a UA
Treatment
Supportive care
IV fluid repletion guided by TBSA affected, as well as electrolyte, protein, and energy supplementation
Consider protecting airway if significant oral mucosal involvement
Stop the offending agent (if there is one)
Advanced wound care and pain control
Consults: Derm to do a biopsy, +/- ophthalmology, gyn / urology to prevent strictures or contractures
Consider transferring to a burn center
Dispo:
Low threshold for ICU admission
SCORTEN ( max of 7 points)
1 point each for
Age over 40
Current cancer
>30% body surface area affected
HR >120
BUN >28
Glucose >240
Bicarb <20
Score of 2 points or higher should -> ICU
Take Home Points
SJS may begin like the flu, with lesions appearing 1-3 days after the prodrome starts
Have to have a high suspicion for SJS because it is deadly. It’s a clinical diagnosis — derm biopsy is supportive
A thorough history and physical exam are key. Remember the characteristic rash and bullae, and always look in the mouth and eyes. Ask about dysuria, sore throat, and eye irritation, as well as preceding medications or infections. Think SATAN!
Prompt supportive care focused on ABCs and IVF repletion are critical. These patients can get sick really fast, so consider an ICU or burn unit.
References:
Barrett W. Quick Consult: Symptoms: Rash, Dysuria, and Mouth Sores. Emergency Medicine News. 41(4): 15-16, April 2019.
Bivins H, Comes J. Stevens-Johnson Syndrome. Rosen and Barkin’s 5-Minute Emergency Medicine Consult. 2015; 1076-1077.
Gerull R, Nelle M, Schaible T. Toxic epidermal necrolysis and Stevens-Johnson syndrome: A review. Crit Care Med. 2011; 39:1521-1532.
Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T. Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clin Rev Allergy Immunol. 2018;54(1):147-76.
McNeil, D. (2019). Measles Cases Surpass 700 as Outbreak Continues Unabated. [online] Nytimes.com. Available at: https://www.nytimes.com/2019/04/29/health/measles-outbreak-cdc.html [Accessed 6 May 2019].
Mustafa SS, Ostrov D, Yerly D. Severe Cutaneous Adverse Drug Reactions: Presentation, Risk Factors, and Management. Curr Allergy Asthma Rep. 2018;18(4):26.
CDC Measles for Health Care Providers. https://www.cdc.gov/measles/hcp/index.html#lab.
Gladwin M, Trattler B. Orthomyxo and Paramyxoviridae. In: Clinical Microbiology Made Ridiculously Simple. 4th ed. Miami, FL: MedMaster, Inc; 2009: 240-243.
Hussey G, Klein M. A Randomized, Controlled Trial of Vitamin A in Children with Severe Measles. N Engl J Med. 1990; 323: 160-164.doi: 10.1056/NEJM199007193230304.
Nir, Sarah Mailin and Gold, Michael. “An Outbreak Spreads Fear: Of Measles, of Ultra-Orthodox Jews, of Anti-Semitism.” New York Times [New York City] 03/29/2019. https://www.nytimes.com/2019/03/29/nyregion/measles-jewish-community.html
A massive thanks to:
Shweta Iyer, MD: NYU Langone 3rd year Pediatric Emergency Medicine Fellow.
Jennifer Lighter, MD: Assistant Professor of Pediatric Infectious Diseases, NYU School of Medicine.
Michael Mojica, MD: Associate Professor of Pediatric Emergency Medicine, NYU Langone Medical Center.
Michael Phillips, MD: Chief Hospital Epidemiologist, NYU Langone Medical Center.
May have mild deformity or decreased functionality and strength in hand grip after this injury
Emergent evaluation if:
Open fracture
Neurovascular compromise
Follow up:
Refer to hand specialist
Within 1 week if fractures of 4thand 5thmetacarpals with angulation
3 to 5 days if the 2ndand 3rd metacarpalsare affected
Immobilized for three to four weeks in splint
Healing may take up to six weeks
Take Home Points:
This is one of the most common fractures we will see as emergency physicians
When evaluating these patients, ensure that this are no other more severe, life-threatening injuries, and pay particular attention to the skin exam so that you do not miss a fight-bite
Reductions may be required if there is significant angulation, which is guided by the 20, 30, 40 rule
Finally, emergent specialist evaluation is indicated if there is an open fracture or evidence of neurovascular compromise
Moran GJ, Talan, DA; Pneumonia, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 76: p 978-89.
Haran JP et al. Macrolide resistance in cases of community-acquired bacterial pneumonia in the emergency department. J Emerg Med 2018. PMID: 29789175
Mandell LA et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44(Suppl 2):S27–72. PMID: 17278083
Arnold FW et al. A worldwide perspective of atypical pathogens in community-acquired pneumonia. AmJ Respir Crit Care Med 2007;175:1086–93. PMID: 17332485
Cauda equina syndrome is a rare emergency with devastating consequences
Early recognition is paramount as the presence of bladder dysfunction portends bad functional outcomes
The presence of bilateral lower extremity weakness or sensory changes should alert clinicians to the diagnosis. Saddle anesthesia (or change in sensation) and any bladder/bowel changes in function should also raise suspicion for the disorder
MRI is the diagnostic modality of choice though CT myelogram can be performed if necessary
Prompt surgical consultation is mandatory for all patients with cauda equina syndrome regardless of symptoms at presentation
Perron AD, Huff JS: Spinal Cord Disorders, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 106: p 1419-30.
References
Lavy C et al. Cauda Equina Syndrome. BMJ 2009; 338: PMID: 19336488
Todd NV. Cauda equina syndrome: the timing of surgery probably does influence outcome. Br J Neurosurg 2005;19:301-6 PMID: 16455534
Sadeghirad B et al. Corticosteroids for treatment of sore throat: systematic review and meta-analysis of randomised trials BMJ 2017; 358 :j3887. PMID: 28931508
Teleb MS et al. Stroke vision, aphasia, neglect (VAN) assessment – a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. J Neurointervent Surg 2017; 9(2): 122-6. PMID: 26891627
While peds traumas and severe traumas are uncommon, stay cool and collected – you’ve run many resuscitations in the past and resuscitating a kid is no different. You’ve got this
When it comes to access, think 1, 2 IO. 2 shots at a peripheral line and if you don’t get it, go to IO
Tachycardia should be assumed to be compensated shock until proven otherwise. Don’t write tachycardia off as anxiety
Failed airway approach – place an 18 gauge catheter into the neck – hopefully through the cricothyroid membrane and bag through that. If you still have difficult getting an airway from above, consider a retrograde intubation over a wire
The PERC risk stratifies low risk PE patients (~10%) to a level low enough (1.9%) as to obviate the need for additional testing.
Age-adjusted D-dimers are ready for use and it doesn’t matter if your assay uses FEU (cutoff 500) or DDU (cutoff 250). For FEU use an upper limit of 10 X age and for DDU use an upper limit of 5 X age.
For now, subsegmental PEs should continue to routinely be anticoagulated even in the absence of a DVT. Keep an eye out for more research on this area.
Although outpatient management of select PE patients (using sPESI or Hestia criteria) may be standard practice, the evidence wasn’t strong enough for ACEP to give it’s support
Patients with DVT can be started on a NOAC and discharged from the ED
ACEP Clinical Policies Subcommittee. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Suspected Acute Venous Thromboembolic Disease. Ann Emerg Med 2018; 71(5): e59-109. PMID: 29681319
Jaconelli T, Eragat M, Crane S. Can an age-adjusted D-dimer level be adopted in managing venous thromboembolism in the emergency department? A retrospective cohort study. European journal of emergency medicine : official journal of the Eur Soc Emerg Med. 2017. PMID: 28079562
Freund Y et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial. JAMA 2018; 319(6): 559-66. PMID: 29450523
In patients with tachypnea, hyperpnea, AMS and clear lungs
In the presence of an anion gap metabolic acidosis with a respiratory alkalosis
Treat salicylate toxicity by alkalinizing the blood and urine to increase excretion
Avoid intubation until absolutely necessary. If you do have to intubate, minimize apneic time and consider awake intubation and nake sure your ventilator settings match the patient’s necessary high minute ventilation
Think about chronic salicylate toxicity in unexplained altered mental status, tachypnea or metabolic acidosis in elderly
Know indications for hemodialysis in salicylate toxic patients
In patients with neck pain, consider Ludwig’s angina particularly if they have any swelling, fever, truisms or respiratory difficulty. Consider early airway management and get your consultants involved early for operative management
Endocarditis is a tricky diagnosis and will often be subtle. Any patient with a prosthetic valve and a fever has endocarditis until proven otherwise. Suspect it in any patient with fever and a murmur, get lots of cultures and remember that TEE is the gold standard but, TTE is highly specific
Finally, penetrating neck trauma. Patients with hard signs – airway compromise, ongoing brisk bleeding, an expanding/pulsatile hematoma, neurologic compromise, shock or hematemesis should go directly to the OR and don’t probe the wounds!
Hard Signs in Penetrating Neck Injury (Sperry 2013)
Management Algorithm for Penetrating Neck Injury (Sperry 2013)
Ben-Israel T et al. Clinical predictors for testicular torsion as seen in the pediatric ED. Am J Emerg Med 2010; 28:786-789.
Sidler D et al. A 25-year review of the acute scrotum in children. S Afr Med J. 1997;87(12) 1696-8. PMID:
Mellick LB. Torsion of the testicle: It is time to stopping tossing the dice. Pediatric Emer Care 2012; 28: 80-6. PMID:
Ban KM, Easter JS: Selected Urologic Problems; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 99: p 1326-1356.
In patients with APE, give high-dose nitro to decrease after load and preload quickly. 400-500 mcg/min for the first 4-5 minutes is my standard approach
Consider DSI to facilitate pre-oxygenation. Ketamine is your go to drug here
A NCHCT performed within 6 hours of symptom onset is extremely sensitive for ruling out SAH but, nothing is 100%. If you’ve got a high-risk patient, you should still consider LP
Patients with caustic ingestions can have rapidly deteriorating airways. Prepare early and be ready to take over the airway at a moments notice
Pollack et al. Idarucizumab for dabigitran reversal – full cohort analysis. NEJM 2017; 377(5): 431-41. PMID: 28693366
Matsue Y et al. Time-to-Furosemide Treatment and Mortality in Patients Hospitalized with Acute Heart Failure J Am Coll Cardiol 2017; 69(25): 3042-51. PMID: 28641794
Summary: Based on the limited available evidence, it’s unlikely orthostatic vital sign measurement can be used to determine which patients have volume loss and which do not. The baseline prevalence of orthostatic vital signs is common and patients will not always develop orthostatic vital signs in response to volume loss. Therefore, there will both be patients who are orthostatic by numbers without volume loss and there will be patients with volume loss who are not orthostatic by numbers. Symptoms, with the exception of inability to stand to have orthostatics performed, are not useful either.
Bottom Line: Based on the low overall sensitivity of orthostatic vital sign measurements, they should not be used to influence clinical decision making.
Skinner JE et al. Orthostatic heart rate and blood pressure in adolescents: reference ranges. J Child Neuro 2010; 25(10): 1210-5. PMID: 20197269
Stewart JM. Transient orthostatic hypotension is common in adolescents. J Pediatr 2002; 140: 418-24. PMID: 12006955
Ooi WL et al. Patterns of orthostatic blood pressure change and the clinical correlates in a frail, elderly population. JAMA 1997; 277: 1299-1304. PMID: 9109468
Aronow WS et al. Prevalence of postural hypotension in elderly patients in a long-term health care facility. Am J Cardiology 1988; 62(4): 336-7. PMID: 3135742 Witting MD et al. Defining the positive tilt test: a study of healthy adults with moderate acute blood loss. Ann Emerg Med 1994; 23(6): 1320-3. PMID: 8198307
McGee S et al. The rational clinical examination. Is this patient hypovolemic. JAMA 1999; 281(11): 1022-9. PMID: 10086438
Johnson DR et al. Dehydration and orthostatic vital signs in women with hyper emesis gravidarum. Acad Emerg Med 1995; 2(8): 692-7. PMID: 7584747
DiMuzio J, Deschler, DG. Emergency department management of foreign bodies of the external ear canal in children. Otol Neurotol. 2002; 23(4):473-5. PMID: 12170148
Leffler S et al. Chemical immobilization and killing of intra-aural roaches: an in-vitro comparative study. Ann Emerg Med. 1993; 22(12):1795-8. PMID: 8239097
Obirikorang C et al. Total Lymphocyte Count as a Surrogate Marker for CD4 Count in Resource-Limited. BMC Infectious Diseases Journal 2012; 12 (128): 1 – 5. PMID: 22676809
1. When seeing patients with AMS, think of the 5 broad categories of pathologies – VS abnormalities, toxic-metabolic, infectious causes, CNS abnormalities and, lastly as a diagnosis of exclusion – psychiatric issues
2. In kids with AMS, think of zebra diagnoses and toxic ingestions and remember that primary psychosis is rare
3. Patients with ALL are susceptible to developing hyperleukocytosis. If the WBC is > 100K, think about getting hematology on the line to initiate chemo induction and leukopheresis
4. Always think about electrolyte disorders, particularly hypoNa in patients with global AMS. Remember to treat severe hypoNa w/ hypertonic saline and, to correct slowly as to avoid ODS
Development of a systematic approach is essential to rapidly assessing the wide diversity of trauma patients and minimizes missed injures
Prepare with whatever information is available before the patient arrives and remember to get a good handoff from the pre-hospital team
Complete the primary survey (ABCDEs) and address immediate life threats
Round out your assessment with a good medical history and remember to complete a comprehensive head-to-toe exam
Read More
Shlamovitz GZ, et al. Poor test characteristics for the digital rectal examination in trauma patients. Ann Emerg Med. 2007;50(1):25-33, 33.e1. PMID: 17391807
Air embolism is a rare but potentially fatal complication of central line placement and some surgical procedures and of course of as the result of barotrauma.
Recognizing the signs and symptoms of air embolism can be tricky because it will look like any other ischemic process. Consider air embolism if you have a patient that rapidly decompensates after placement of a central line, the most likely culprit for those of us in the ED.
Treatment should focus on supportive cares. Give supplemental O2, IV fluids and hemodynamic support and consider hyperbarics and cardiopulmonary bypass for the super sick patient.
SBP is a difficult diagnosis to make because presentations are variable. Consider a diagnostic paracentesis in all patients presenting to the ED with ascites from cirrhosis
An ascites PMN count > 250 cells/mm3 is diagnostic of SBP but treatment should be considered in any patient with ascites and abdominal pain or fever
Treatment of SBP is with a 3rd generation cephalosporin with the addition of albumin infusion in any patient meeting AASLD criteria (Cr > 1.0 mg/dL, BUN > 30 mg/dL or Total bilirubin > 4 mg/dL)
Read More
Oyama LC: Disorders of the liver and biliary tract, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 90: p 1186-1205.
Non-specific viral syndromes are usually just that, a viral syndrome but, be cautious as a number of more serious ailments can present similarly. This includes tick borne illnesses, acute HIV and carbon monoxide
Doxycycline is safe in kids. The dental staining seen with tetracycline is specific to that drug, not the class. If doxy is the best drug for the disease, use it.
Lots of meds can lead to a myasthenia gravis exacerbation. Carefully review meds before prescribing for interactions
Suspect a toxic alcohol in any patient with a large osmol gap or a large anion gap metabolic acidosis and consider treating these patients empirically.
Fomepizole is the critical antidote for toxic alcohol ingestions but, patients are likely going to require dialysis as well.
Call your local poison control center if you suspect a toxic alcohol ingestion to help guide management.
Keep IIH and CVST on the differential for patient’s coming in with a subacute headache, particularly if they have visual or neuro symptoms.
Consider an ocular ultrasound! It’s quick, shockingly easy to do, and can help point you toward a diagnosis you may have otherwise overlooked. I have made it my practice now to include a quick look in the physical exam of my patients with a concerning sounding headache or a headache with neurologic symptoms.
Consider IIH particularly in an overweight female of child bearing age with a subacute headache, but remember patients outside that demographic can have IIH as well.
Consider CVST in a patient with a thrombophilic process like cancer, pregnancy or the use of OCPs or androgens or in a patient with a recent facial infection like sinusitis or cellulitis.
Think about flexor tenosynovitis in a patient with atraumatic finger pain. They may have any combination of these signs:
Tenderness along the course of the flexor tendon
Symmetrical swelling of the finger – often called the sausage digit
Pain on passive extension of the finger and
Patient holds the finger in a flex position at rest for increased comfort
Give antibiotics to cover staph, strep and possibly gram negatives.
Get your surgeon to see the patient, while we can get the antibiotics started, these patients need admission and may require surgical intervention.
Infographic
by Dr. Y. Jay Lin
Read More
Mailhot T, Lyn ET: Hand; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 50: p 534-571
In patients with shortness of breath and clear lungs, consider metabolic acidosis with respiratory alkalis as a potential cause
Suspect MALA in any patient on metformin who presents with abdominal pain, nausea and vomiting and/or AMS
Patients with MALA will have a low pH, a high-anion gap metabolic acidosis and high lactate levels
Call your tox consultant to assist with management which will focus on fluid resuscitation with isotonic bicarbonate and dialysis
Read More
Bosse GM. Antidiabetics and Hypoglycemics. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e New York, NY: McGraw-Hill; 2015. Link Accessed October 31, 2017
SBP is a difficult diagnosis to make clinically. While patients may have the triad of fever, abdominal pain and increasing ascites, they are far more likely to only have 1 or 2 of these symptoms
In patients admitted to the hospital with ascites, consider performing a diagnostic paracentesis on all patients as limited literature shows an association with decreased mortality and, the procedure is simple and low risk
Once you get the fluid, focus on the cell count: WBC > 500 or PMN > 250 should prompt treatment with a 3rd generation cephalosporin and albumin infusion
Gaetano et al. The benefit of paracentesis on hospitalized adults with cirrhosis and ascites. Journal of Gastroenterology and Hepatology 2016. PMID: 26642977
Up to 50% of true knee dislocations will spontaneously reduce prior to arrival. Be suspicious of a dislocation in any patient who describes the joint moving out of place or if they have significant swelling, joint effusion or ecchymosis despite normal X-rays
In all patients with suspected dislocation, perform a neurovascular exam immediately as popliteal artery injury is common. If they’ve got an absent DP or PT pulse, reduce immediately and get a CT angiogram as quickly as possible to assess for popliteal injuries
If distal pulses are intact, you can either do ABIs and if normal, observe and repeat them or get a CTA. If the ABI is abnormal or the patient had an absent or decreased pulse at any point, get the CTA
Ranson’s Criteria for Pancreatitis-Associated Mortality (Rosen’s)
Take Home Points
Pancreatitis is diagnosed by a combination of clinical features (epigastric pain with radiation to back, nausea/vomiting etc) and diagnostic tests (lipsae 3x normal, CT scan)
A RUQ US should be performed looking for gallstones as this finding significantly alters management
The focus of management is on supportive care. IV fluids, while central to therapy, should be given judiciously and titrated to end organ perfusion
Patients will mild pancreatitis who are tolerating oral intake and can reliably follow up, can be discharged home
Read More
Hemphill RR, Santen SA: Disorders of the Pancreas; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 91: p 1205-1226
The most common bites and stings you will see are by bees and ants. These can present as a local reaction, toxic reaction, anaphylaxis or delayed reaction. For all of these, treat with local wound care and epinephrine for any systemic symptoms.
The brown recluse spider is found in the Midwest and presents as local pain and swelling but carries the risk of a necrotic ulcer
The black widow spider is found all around the US and presents with either localized or generalized muscle cramping, localized sweating and potentially tachycardia and hypertension. Treatment is symptom management with analgesics and benzos.
The bark scorpion usually presents with localized pain and swelling, but particularly in children, may present with a serious systemic presentation including jerking muscle movements, cranial nerve dysfunction, hypersalivation, ataxia and opsoclonus, which is the rapid, involuntary movement of the eyes in all directions. Treatment is supportive cares, but remember to call your poison center to ask about antivenin.
Tachycardia in peds patients at discharge was associated with more revisits but not with more critical interventions. If your workup is reassuring, isolated tachycardia in and of itself shouldn’t change your disposition.
Supplemental O2 is not necessary in the management of AMI patients with an O2 sat > 90% and, may be harmful
Until further study and prospective validation has been performed, we’re not going to recommend embracing the Canadian decision instrument on predicting dysrhythmias after a syncopal event.
Finally, our agreement on what cardiac standstill is isn’t great. We need a unified definition going forward to teach our trainees and for the purposes of research.
Gaspari R et al. Emergency Department Point-Of-Care Ultrasound in Out-Of-Hospital and in-ED Cardiac Arrest. Resuscitation 2016; 109: 33 – 39. PMID: 27693280
References
Wilson PM et al. Is Tachycardia at Discharge from the Pediatric Emergency Department a Cause for Concern? A Nonconcurrent Cohort Study.Ann Emerg Med. 2017. PMID: 28238501
Hofmann R et al. Oxygen Therapy in Suspected Acute Myocardial Infarction. NEJM 2017. PMID: 28844200
Thiruganasambandamoorthy V et al. Predicting short-term risk of arrhythmia among patients with syncope: the Canadian syncope arrhythmia risk score. Acad Emerg Med 2017. PMID: 28791782
Hu K et al. Variability in Interpretation of Cardiac Standstill Among Physician Sonographers. Ann Emerg Med 2017. PMID: 28870394
Cholangitis is an acute bacterial infection of the bile ducts resulting from common bile duct obstruction and is potentially life-threatening (mortality 5-10%, acute bacterial infection of the bile ducts
Diagnosis is based on clinical findings and while imaging can be supportive, it is frequently non-diagnostic. Look for RUQ tenderness with peritoneal signs and fever
A normal ultrasound does not rule out acute cholangitis
Treatment focuses on supportive care, broad spectrum antibiotics and consultation with a provider that can provide biliary tract decompression (IR, gastroenterology or general surgery)
Acute cholecystitis is an inflammation of the gallbladder and is a clinical diagnosis. Imaging can be helpful but US and CT can both have false negatives.
Lab tests are insensitive and non-specific and, as such, they can neither rule in or rule out the diagnosis.
Treatment focuses on fluid resuscitation when indicated, supportive care, antibiotics and surgical consultation for cholecystectomy
Although uncommon, be aware that patients can develop gangrene, necrosis and perforation as well as frank sepsis and require aggressive resuscitation
Oyama LC: Disorders of the liver and biliary tract, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 90: p 1186-1205.
Leschka S et al. Chapter 5.1: Acute abdominal pain: diagnostic strategies In: Schwartz DT: Emergency Radiology: Case Studies. New York, NY: McGraw-Hill, 2008.
Menu Y, Vuillerme MP. Chapter 5.5: Non-traumatic Abdominal Emergencies: Imaging and Intervention in Acute Biliary Conditions In: Schwartz DT: Emergency Radiology: Case Studies. New York, NY: McGraw-Hill, 2008.
Consider the diagnosis in all patients with nutritional deficiencies, not just alcoholics.
Look for ophthalmoplegia, ataxia and confusion in patients that have risk factors for thiamine deficiency.
Don’t think that it can’t be Wernicke’s because the triad isn’t complete; any two of the components (dietary deficiency, oculomotor abnormalities, cerebellar dysfunction or altered mental status) makes the diagnosis.
Treat Wernicke’s with an initial dose of 500 mg of thiamine IV and admit for continued parenteral therapy.
Chronic drinkers and even just acutely intoxicated patients are at risk of many medical emergencies including life threatening trauma, infections, metabolic derangements and tox exposures. Don’t dismiss them as “just drunk”
Undress these patients and perform a thorough head to toe examination, focusing on looking for e/o trauma and infection. Get as much history as you can and be sure to ask about their drinking habits and etoh w/d hx to risk stratify them in your brain
Always check FS glucose and replete glucose as needed.
Consider giving your chronic intoxicated patients thiamine injections semi-regularly to prevent WE, and look for e/o the triad in your patients as it can be easily overlooked and deadly if missed!
Suspect preeclampsia in any pregnant women presenting with epigastric/RUQ pain, severe or persistent headache, visual disturbances, nausea or vomiting, shortness of breath, increased edema or weight gain
Evaluate for preeclampsia by looking at the blood pressure, urine for protein and obtaining a panel to evaluate for HELLP syndrome
Severe preeclampsia and eclampsia are treated with bolus and infusion of MgSO4
Emergency delivery is the “cure” for preeclampsia and eclampsia. Consult obstetrics early for an evaluation for delivery
Don’t forget to consider preeclampsia and eclampsia in the immediate postpartum period
Bed up head elevated position for intubation may reduce intubation related complications.
Patients who are hypotensive or at risk of hypotension should be aggressively resuscitation prior to intubation with fluids and liberal use of pressors
Shock patients would be intubated with decreased induction agent dose, preferably ketamine, and increased paralytic dose.
Swaminathan A, Mallemat H. Rocuronium Should Be the Default Paralytic in Rapid Sequence Intubation. Ann Emerg Med 2017. PMID: 28601274
Khandelwal N et al. Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Anesth Analg 2016; 122(4): 1101-7. PMID: 26866753
Airway management is paramount, expect a challenging intubation and consider controlling the airway early
When controlling the airway, consider an awake approach and fiberoptics if available. Always be prepared for the can’t intubate, can’t oxygenate scenario with a double set up.
If the patient has urticaria and pruritus, the process is likely histamine mediated and will respond to typical anaphylaxis treatment
Finally, observe the patient for progression of swelling and don’t forget to stop the inciting medication
Always perform a full pre-PSA evaluation including an airway assessment. Time of last meal shouldn’t delay your sedation based on the best available evidence.
Always do a complete setup including consideration of different agents, dosage calculations, preparation of airway equipment and reversal agents.
PSA serious adverse events are rare but you still must be prepared for them. Careful agent selection and dosing can help prevent issues but, know your outs.
If apnea develops, do some basic maneuvers before you reach for the BVM or laryngoscope. Remember OOPS as in “oops, my patient went apneic.” Oxygen on, pull the mandible forward and sit the patient up. This fixes most issues
Bellolio MF et al. Incidence of adverse events in adults undergoing procedural sedation in the emergency department: a systematic review and meta-analysis. Acad Emerg Med 2016; 23: 119-34. PMID: 26801209
Stevens DL et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis 2014; 59(2): e10-52. PMID: 24973422
McCollough M, Sharieff GQ: Genitourinary and Renal Tract Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 174: p 2205-2223.
Davis JE, Silverman MA. Urologic Procedures; in Roberts JR: Roberts and Hedges’ Clinical Procedures in Emergency Medicine, ed 6. 2014, (Ch) 55: p 1113-1154
Govier FE et al. Oral terbutaline for the treatment of priapism. J Urol 1994;151: 878-9. PMID: 8126815
Priyadarshi S. Oral terbutaline in the management of pharmacologically induced prolonged erection. Int J Impot Res. 2004;16:424-426. PMID: 14999218
Appelboam A et al. Postural Modification to the Standard Valsalva Manoeuvre for Emergency Treatment of Supraventricular Tachycardias (REVERT): A Randomised Controlled Trial. Lancet 2015. PMID: 26314489
Be prepared to intubate early, the patency of the airway can decline quickly and without warning. If there is any concern for burns to face/neck or smoke inhalation, consider taking control of the airway early.
Review the rule of 9s and the parkland formula to direct your large volume fluid resus. Remember the parkland formula directs you to use 4 mL x %TBSA x weight (kg). Half in the first 8 hours and the second half over the next 16 hours. Given the large volume here it’s probably best to use LR or another balanced solution.
Do a thorough trauma eval to make sure you don’t miss any other injuries and be sure to watch for developing compartment syndrome
And last, consider the need to treat for CO and/or cyanide poisoning. Poor cardiac function, cardiac arrest or a high lactate can be clues to cyanide poisoning and just start 100% O2 while you wait for a co-ox, since CO tox is pretty likely.
Parvizi D et al. The potential impact of wrong TBSA estimations on fluid resuscitation in patients suffering from burns: things to keep in mind. Burns 2014; 40: 241-5. PMID: 24050977
Hettiaratchy S, Dziewulski P. ABC of Burns: Introduction. BMJ 2004; 328: 1366-8. PMID: 15178618
Hettiaratchy S, Papini R. ABC of Burns: Initial Management of a Major Burn: I – Overview. BMJ 2004; 328: 1555-7. PMID: 15217876
Hettiaratchy S, Papini R. ABC of Burns: Initial Management of a Major Burn II – Assessment and Resuscitation . BMJ 2004; 329: 101-3. PMID: 15242917
The step-by-step approach to managing febrile infants is a reliable decision instrument to identify patients at low risk for invasive bacterial infections. Caution in the group of patients 22-28 days of age.
The LOV-ED study shows an association between employing a lung-protective ventilation strategy in the ED and decreased complications from mechanical ventilation. Best available evidence says that we should embrace this approach in the ED.
Cooling to 33 degrees is no better than cooling to 36 degrees. However, shooting 36 degrees is more difficult than we may have thought. We have to continue to be vigilant about maintaining patients in the target temperature range and avoiding fever.
Gomez B et al. Validation of the Step-by-Step Approach in the Management of Young Febrile Infants. Pediatrics. 2016 Aug. PMID: 27382134
Fuller BM et al. Lung-Protective Ventilation Initiated in the Emergency Department (LOV-ED): A Quasi-Experimental, Before-After Trial. Ann Emerg Med 2017. PMID: 28259481
Bray JE et al. Changing target temperature from 33oC to 36oC in the ICU management of out-of-hospital cardiac arrest: a before and after study. Resuscitation 2017; 113: 39-43. PMID: 28159575
Nuito I et al. Time to cardioversion for acute atrial fibrillation and thromboembolic complications. JAMA 2014; 312(6): 647-9. PMID: 25117135
Stiell IG et al. Association of the Ottawa aggressive protocol with rapid discharge of emergency department patients with recent-onset atrial fibrillation and flutter. Can J Emerg Med 2010; 12(3): 181-91. PMID: 20522282
Stiell IG et al. Outcomes for Emergency Department Patients with Recent-Onset Atrial Fibrillation and Flutter Treated in Canadian Hospitals. Ann Emerg Med 2017. PMID: 28110987
MetHb –emia occurs as a results of various medications including amyl nitrite, dapsone, nitroprusside, phenazopyridine, sodium nitrite and topical anesthetics like benzocaine
Patients will present with cyanosis, short of breath, fatigue, dizziness, weakness and ultimately CNS depression and death at higher concentrations.
If you have a cyanotic/hypoxic patient that does not respond to supplemental oxygen, be concerned for MetHb and send a co-oximetry panel.
If the level is <25% and the patient is asymptomatic you can observe, but if the level is >25% or the patient is symptomatic, you will treat with the antidote methylene blue given as a bolus of 1-2 mg/kg over 5 minutes
And as always, make sure to call your local poison center to get your toxicologists involved. They can help with dosing, and they are also an important player of the public health component in cases such as these, to make sure this is an isolated incident and we don’t have a repeat of the 11 blue men situation.
Price DP. Chapter 127. Methemoglobin Inducers. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e New York, NY: McGraw-Hill; 2011. Accessed April 19, 2017.
CO poisoning happens most often from common are accidental exposures from faulty home heaters, camp stoves and indoor use of gas powered generators, structure fires and intentional exposure like in suicide attempts.
Patients with a mild exposure will present with symptoms like headache, nausea, vomiting, dizziness, vision blurring, palpitations, confusion or myalgias. More severe exposures may produce Altered mental status. seizures, coma, dysrythmias, myocardial ischemia, metabolic acidosis, syncope and vital sign abnormalities including hypotension and, eventually, cardiac arrest.
To help distinguish the vague symptoms of a patient who may have chronic exposure ask about things like whether symptoms improve in different environments or whether they have sick pets, as human viral illness generally don’t affect our dogs and cats.
If you’re concerned about CO send a co-ox panel. City dwellers may have a baseline carboxyhemoglobin of 1-2% and smokers around 6-10% but others should really have no carboxyhemoglobin.
Treatment is supplemental O2 which can be stopped when symptoms improve. For severe symptoms and for pregnant patients, consider hyperbarics to prevent long term sequelae and to protect the fetus. As always, consider discussing the case with your local poison center to help decide whether a patient warrants transfer for hyperbarics.
Nelson LS, Hoffman RS: Inhaled Toxins, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 159: p 2036-2045.
Tomaszewski C. Chapter 125. Carbon Monoxide. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e New York, NY: McGraw-Hill; 2011. Accessed April 19, 2017.
Schwartz DR, Kaufman B. Local Anesthetics. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e New York, NY: McGraw-Hill; 2015. Link
Neal JM et al, American Society of Regional Anesthesia and Pain Medicine. American Society of Regional Anesthesia and Pain Medicine checklist for managing local anesthetic systemic toxicity: 2012 version. Reg Anesth Pain Med 2012;37:16–8. PMID: 22189574
Cao D et al. Intravenous lipid emulsion in the emergency department: a systematic review. J Emerg Med 2015; 48(3): 387-97. PMID: 25534900
Attia J et al. Does this adult patient have acute meningitis. JAMA 1999; 281(2): 175-81. PMID: 10411200
Brouwer MC et al. Corticosteroids for acute bacterial meningitis (review). Cochrane Database Syst Rev 2015. PMID: 26362566
Cooper DD, Seupaul RA. Is adjunctive dexamethasone beneficial in patients with bacterial meningitis? Ann Emerg Med 2012; 59(3): 225-6. PMID: 22088494
de Gans J et al. Dexamethasone in adults with bacterial meningitis. NEJM 2012; 347(20): 1549-57. PMID: 12432041
Hasbun R et al. Computed tomography of the head before lumbar puncture in adults with suspected meningitis. NEJM 2001; 345(24): 1727-34. PMID: 11742046
Sakushima K et al. Diagnostic accuracy of cerebrospinal fluid lactate for differentiating bacterial meningitis from aseptic meningitis: a meta-analysis. J Infection 2011; 62: 255-62. PMID: 21382412
Tunkel AR et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis 2004; 39: 1267-84. PMID: 15494903
On any dialysis patient, make sure to do a good assessment of their access site. If it’s a fistula, assess for a thrill, for any warmth/induration/erythema and make sure they have distal sensation and perfusion. If it’s a catheter, evaluate for any signs of infection—so warmth, erythema or discharge.
Bleeding is a big concern. If the patient is bleeding from their access, start with direct pressure to the bleeding site, then move on to topical thrombotic agents and if needed throw a figure 8 stitch with a 5-0 proline on a non-cutting needle.
Peritoneal dialysis patients are at risk for bacterial peritonitis. In a PD patient that appears infected, get a peritoneal fluid sample and start antibiotics
Dialysis patients are susceptible to dialysis disequilibrium syndrome which can present as altered mental status, focal neurological deficits or even frank coma or seizures after dialysis. Make sure to consider a broad differential in these patients and start with a solute load such as an amp or two of D50 while starting your work up.
Sinusitis is a clinical diagnosis. Patients typically present with purulent nasal discharge and facial pain or other URI symptoms.
The vast majority of patients with acute rhino sinusitis will be viral in nature and will not benefit from antibiotics
Patients with prolonged symptoms, more than 7-10 days, without improvement or continued fevers past 2-3 days should be considered for antibiotic treatment as should those who are immunocompromised.
Show Notes
Melio FR, Berge LR. Upper Respiratory Tract Infections, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 75: p 965-79.
The first step is managing epistaxis is solid pressure. This means holding a tight pinch just distal to the nasal bones and hold, without peaking, for at least 5 minutes. This will stop a good deal of the bleeding.
If you need to do more, start by soaking gauze in either oxymetazoline or epinephrine, mix in some lidocaine to help with anesthesia, pack the nare with that and add on some compression. Hope fully this stops the bleeding enough that you can see a good bleeder and perform cautery.
Third line of treatment would be to try some soaked gauze, but this time with TXA. Can’t hurt to try!
And then last resort is of course packing. Here make sure the patient is anesthetized with some lidocaine, lubricate the packing well and apply horizonally, no vertically as we are often tempted.
Zahed R et al. A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med 2013; 31: 1389-92. PMID: 23911102
When looking at a tachy rhythm that isn’t sinus tach, quickly differentiate by determining if the QRS complexes is narrow or wide and then determine if the rhythm is regular or irregular. This approach quickly drops the rhythm into 1 of 4 boxes and makes rhythm determination much easier
Each of those 4 categories has a small set of rhythms included. Narrow and irregular – AF, Aflutter with variable block or MFAT. Narrow and regular – SVT or Aflutter. Wide and irregular – Torsades, VF, AF with aberrancy or a BBB. Wide and regular – VTach, SVT with aberrancy or SVT with a BBB.
If you see wide and regular, the top 3 diagnoses are VT, VT and VT. Assuming VT and treating for that will almost never send you astray
The POKER trial examined the difference between propofol and ketofol when it comes to adverse respiratory events. They found no significant difference between the groups. Given the increased risk of medication errors using two medication instead of one, you may want to avoid the mixture.
Ketorolac has an analgesic ceiling effect lower than you may have thought. When comparing IV doses of 10mg, 15mg and 30mg they found no difference in analgesic effect. Given the risks of side effects may increase with higher doses, you may want to stick to the lower 10mg dose.
Propofol or Ketofol for Procedural Sedation and Analgesia in Emergency Medicine-The POKER Study: A Randomized Double-Blind Clinical Trial. PubMed ID: 27460905
Comparison of Intravenous Ketorolac at Three Single-Dose Regimens for Treating Acute Pain in the Emergency Department: A Randomized Controlled Trial. PubMed ID: 27993418
An Rh negative woman can become alloimmunized to Rh antigen if exposed to blood from an Rh positive fetus. Theoretically, this alloimmunization can occur even in early pregnancy
While anti-D immune globulin has clearly been shown to be beneficial in preventing alloimmunization in 2nd and 3rd trimester pregnancy, there is no evidence supporting use specifically in the 1st trimester
Despite the absence of evidence, RhoGam administration has become routine in many places. At this time, it’s advisable to follow local practice patterns regarding which patients should be given RhoGam.
References
ACOG Practice Bulletin. Prevention of Rh D Alloimmunization. Int J Gynaecol Obstet 1999; 66(1): 63-70. PMID: 10458556 Recommendations reaffirmed in 2016
Hahn SA et al. Clinical Policy: Critical Issues in the Initial Ealuation and Management of Patients Presenting to the Emergency Department in Early Pregnancy. Ann Emerg Med 2012; 60(3): 381-419. PMID: 22921048
Hannafin B et al. Do Rh-Negative Women with First Trimester Spontaneous Abortions Need Rh Immune Globulin. Am J Emerg Med 2006; 24: 487-9. PMID: 16787810
Visscher RD, Visscher HC. Do Rh-Negative Women with an Early Spontaneous Abortion Need Rh Immune Prophylaxis? Am J Obstet Gynecol 1972; 113(2): 158-65. PMID: 4623673
If you have a patient with a cord prolapse, elevate the presenting part to take pressure off the cord, place the patient in trendelenburg and fill the bladder. Then, redline it to the OR for a c-section.
Nuchal cord is common but likely not too dangerous. Just gently unwrap the umbilical cord and the fetus should be just fine
Shoulder dystocia isn’t common but it’s a true emergency as the fetus can suffer severe hypoxia or death. You’ve got a bout 5 minutes to deliver. Immediately call for help from OB, place a foley catheter to drain the bladder and place the mom’s legs so that her knees are pressed into her chest. This helps to open up the pelvis and give more room for the shoulder to be delivered. If that doesn’t work, you can try the wood’s screw maneuver or place the mom on all 4s. If you’ve got an OR ready, pushing the head back in is also an option but only if you have an OR available
If you get a heads up from EMS on an incoming trauma, take the lead time you get to clearly delineate everyone’s roles to help ensure the resuscitation runs smoothly.
In the severe TBI patient, the key is in preventing secondary injury to the brain. We do this by guarding against hypoxia, hypercarbia, hypotension and aspiration. Max your pre-ox, get the ETT in quickly to prevent oxygenation and ventilation issues and keep the head up if possible
Hypotension is rarely seen in isolated head trauma. If the patient is or becomes hypotensive, reassess for any sources of hemorrhagic shock that may have been missed and consider whether the meds you gave may have caused the problem.
Hypertension is much more common and despite extensive research, we haven’t shown that dropping the patient to normal levels is beneficial. Keeping the SBP < 180 seems reasonable but check your local protocol as well.
If the patient’s ICP spikes or your concerned about herniation, administer mannitol or hypertonic saline and get your neurosurgeon to the bedside since the patient is gonna need decompression
Finally, make sure to reverse any anticoagulant the patient may have on board as this will hopefully prevent hematoma expansion.
Wang X et al. Ketamine does not increase intracranial pressure compared with opioids: meta-analysis of randomized controlled trials. J Anesth 2014; 28(6): 821-7. PMID: 24859931
Zeiler FA et al. The ketamine effect on ICP in traumatic brain injury. Neurocrit Care 2014; 21(1): 163-73. PMID: 24515638
Edlow JA. Managing nontraumatic acute back pain. Ann Emerg Med 2015; 66: 148-53. PMID: 25578887
Goldberg H et al. Oral steroids for acute radiculopathy due to a herniated lumbar disk: a randomized clinical trial. JAMA 2015; 313 (19): 1915-23. PMID: 25988461
Friedman BW et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA 2015; 314 (15): 1572-80. PMID: 26501533
Get a detailed history to tease out whether the patient had a seizure or a syncopal event. Regardless, get an EKG on 1st time seizures in case it was actually syncope.
BZDs are first line therapy for seizure termination. If you don’t have IV access, go with 10 mg of midazolam or 2-4 mg of lorazepam IM
Always review the 5 main categories for causes of seizures in order to make sure you’re not missing anything. Those categories once again are vital sign abnormalities, CNS infections, toxic/metabolic issues, CNS space occupying lesions including masses and bleeds and finally epilepsy.
In patients with a first time seizure without a particular cause and return to baseline neurologic status, there’s unlikely to be any benefit to a NCHCT or to starting an AED. Scheduling close follow up with a neurologist is very reasonable. The key is to do a thorough examination and make sure you’re not missing a subtle abnormality.
Finally, in status epilepticus hit the patient with 2-3 hefty doses of BZDs and if the seizure is still ongoing, strongly consider moving to propofol and intubation in order to rapidly control the seizure activity.
Huff SJ et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Seizures. Ann Emerg Med 2014; 43(5): 605-25. PMID: 15111920
Don’t rush to the airway. In most situations, you have some time so resuscitate before you intubate. Give blood products and get the BP up a bit to give yourself a little better physiologic situation in which to intubate.
Start your massive transfusion immediately if the patient is shocked. There’s always a delay in getting products but the earlier you start, the shorter the delay.
Include US in your primary survey. Your E-FAST should start with the cardiac window, then go to the lungs and then, finally, the abdomen. This order focuses on finding pathology you can fix immediately.
If the patient is shocked and peri-arrest or recently lost vitals, open the chest and look for a fixable injury. Start with opening the pericardium to relieve tamponade, identify and repair cardiac wounds and cross clamp the aorta.
In a patient with significant head and neck trauma, EACH step of the airway management can be more difficulty. BVM may be hard, LMA may be hard, RSI may be hard, so don’t be afraid to ask for help early.
Decide whether the patient has an actual obstruction of their airway. If they are obstructed above the larynx, don’t bother with your usual airway maneuvers, go directly to the surgical airway.
When you do attempt RSI, have double suction and multiple airway techniques set up. This is the time to have your friend standing at your side, scalpel in hand and ready to move directly down the difficult airway algorithm if trouble arises.
Finally, consider keeping the patient awake and preserving their own respiratory drive as it may give you more time to secure the airway.
Giradis M et al. Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 316(15):1583-1589. 2016. PMID: 27706466
Meyhoff CS et al. PROXI Trial Group. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009; 302(14):1543-1550. PMID: 19826023
Stub D et al. AVOID Investigators. Air versus oxygen in ST-segment-elevation myocardial infarction. Circulation. 2015;131(24):2143-2150. PMID: 26002889
CRASH-2 trial collaborators. Effects of tanexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a ransomised placebo-controlled trial. Lancet 2010; 376: 23-32. PMID: 20554319
Guerriero C et al. Cost-effectiveness analysis of administering tranexamic acid to bleeding trauma patients using evidence from the CRASH-2 trial. PLoS One 2011; 6(5): e18987. PMID: 21559279
Ker K et al. Avoidable mortality from giving tranexamic acid to bleeding trauma patients: an estimation based on WHO mortality data, a systematic literature review and data from the CRASH-2 trial. BMC Emerg Med 2012; 12:3. PMID: 22380715
Morrison JJ et al. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) Study. Arch Surg 2012; 147 (2): 113-9. PMID: 22006852
A Lisfranc injury is a midfoot injury that results in displacement of one or more of the metatarsal bones from tarsus.
XR will show widening of the space between the 1st and 2nd metatarsals. Getting contralateral XR may help you identify this.
Even if you don’t see that widening on the XR, the patient could still have a Lisfranc injury. If they cannot walk due to pain, get a weight bearing XR or CT scan to look further.
Once the injury is identified, the patient must be strict non-weightbearing. Place them in a posterior splint and get orthopedics involved either in the ED or for prompt follow up as the patient will probably need surgery.
Foot Bones (Google Images)
Normal Foot X-ray Series (Case courtesy of Dr Andrew Dixon, Radiopaedia.org. From the case rID: 36688)
Lisfranc Injury AP X-ray (Radiopaedia Image #1: Case courtesy of Dr Alexandra Stanislavsky, Radiopaedia.org. From the case rID: 10919)
Cavallaro F et al. Diagnostic accuracy of passive leg raising for prediction of fluid responsiveness in adults: systemic review and meta-analysis of clinical studies. Intensive Care Med. 2010:36(9):1475-83. PMID: 20502865.
Cecconi M et al. Fluid challenges in intensive care: the FENICE study: A global inception cohort study. Intensive Care Med. 2015:41(9):1529-37. PMID: 26162676.
Landesberg G et al. Diastolic dysfunction and mortality in severe sepsis and septic shock. Eur Heart J. 2012:33(7):895-903. PMID: 21911341.
Lee CV et al. Development of a fluid resuscitation protocol using inferior vena cava and lung ultrasound. J Crit Care. 2016:31(1):96-100. PMID: 26475100.
GERD pain can mimic or co-exist with the more deadly causes of chest pain. Be sure to consider all the serious causes of chest pain, get an EKG and maybe a chest XR while you go about symptom management.
Respond to a treatment doesn’t prove a diagnosis. GERD pain may get better with nitro and ACS pain may get better with a GI cocktail. Keep an open mind while seeing these patients.
Standard treatment for GERD includes an antacid and H2 blocker and maybe a PPI. Keep in mind that a PPI takes a while to work, so be sure to give something faster acting in the ED
And last, for these patients, take those few extra minutes for some counseling on lifestyle modifications. All medications come with side effects, so be sure to address things like diet, smoking and weight loss while you have a captive audience.
Respect the UGIB. These patients can bleed a lot. Even if they’re not actively hemorrhagic in front of you, realize that they can open up at any time and decompensate
Get your consultants on board early. A skilled endoscopist is your friend as they can get control of bleeding. Don’t forget IR for TIPS in variceal bleeds and general surgery in bleeding ulcers.
Activate your massive transfusion protocol if the patient is unstable and give the patient PRBCs, FFP and platelets as indicated. Reverse any anticoagulants as well.
Give all patients with confirmed or suspected variceal bleeding antibiotics – typically, ceftriaxone. This intervention saves lives and decreases morbidity.
Baclofen withdrawal is a rare complication of intrathecal baclofen pumps. It’s presentation mimics sepsis and alcohol withdrawal and is characterized by hemodynamic instability, hyperthermia, increased spasticity, confusion, altered mental status and seizures. Patients can develop rhabdo from the spasticity and, eventually, can develop multi system organ dysfunction.
Treating baclofen withdrawal with oral baclofen is unlikely to work even at large oral doses because only a tiny amount gets into the CSF where it needs to act for withdrawal to be treated
Baclofen withdrawal can be emergently treated with increasing benzodiazepine doses, propofol infusions and baclofen administered via a lumbar puncture. Ultimately, these patients all need consultation with either neurosurgery or interventional pain management to interrogate the device and surgically correct the issue.
Chidester S, Smith S. Baclofen pump complications. The NYS Poison Centers Toxicology Letter 2011; 16(4): 1-12. Link
Ross J et al. Acute Intrathecal Baclofen Withdrawal: A Brief Review of Treatment Options. Neurocrit Care. 2011;14(1):103-108. PMID: 20717751
Stetkarova I et al. Procedure- and device-related complications of intrathecal baclofen administration for management of adult muscle hypertonia: a review. Neurorehabil Neural Repair. 2010;24(7):609-619. PMID: 20233964
Shirley KW et al. Intrathecal baclofen overdose and withdrawal. Pediatr Emerg Care. 2006;22(4):258-261. PMID: 16651918
Most COPD exacerbations are caused by infectious etiologies. While these can be viral, there’s also a decent chance it was caused by an overgrowth of bacteria that chronically colonize these patients.
Strong evidence from systematic reviews demonstrates that antibiotic use reduces in-hospital mortality and decreases treatment failure
The GOLD group recommends antibiotics be given to patients who have increased dyspnea, increased sputum volume and increased sputum purulence or require non-invasive or invasive ventilation for their exacerbation.
Finally, a short course of antibiotics – either ampicillin, doxycycline or azithromycin is adequate for management.
Berg RMG, Plovsing RR. The hardships of being a Sith Lord: implications of the biopsychosocial model in a space opera. Adv Physiol Educ 2016; 40: 234-6. PMID: 27105743
Johannes M et al. Antibiotics in Addition to Systemic Corticosteroids for Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Am J Resp Crit Care Med 2010; 181(2): 150-7. PMID: 19875685
Quon BS et al. Contemporary management of acute exacerbations of COPD: a systematic review and metaanalysis. Chest 2008; 133:756-66. PMID: 18321904
Ram FS et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2006:CD004403 PMID: 16625602
Rothberg MB et al. Antibiotic Therapy and Treatment Failure in Patients Hospitalized for Acute Exacerbations of Chronic Obstructive Pulmonary Disease. JAMA 2010; 303(20): 2035-2042 PMID: 20501925
Vollenweider DJ et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2012: CD010257 PMID: 23235687
Hiccups, or singultus, are caused by a reflex arc involving the vagus nerve, CNS and phrenic nerve. If you remember the path of these nerves, you can remember that possible bad pathologies that could cause a patient to present with prolonged hiccups.
Physical maneuvers are the first line for solving the hiccups. Try things that will interrupt respiration or stimulate the vagus nerve. We like the modified valsalva in which the patient blows on a syringe, because it’s pretty easy to get the patient to do.
Last, medication options for hiccups include antipsychotics, anticonvulsants, muscle relaxers and dopamine agonist. Generally, we start with chlorpromazine 25-50 mg PO or IM.
Read More
Steger M et al. Systemic review: the pathogenesis and pharmacological treatment of hiccups. Aliment Pharmacol Ther 2015; 42(9):1037-50. PMID 26307025
Keep esophageal rupture on your differential for deadly causes of chest, epigastric or back pain. We don’t see it often, but it’s a real thing.
Boerhaave Syndrome is the spontaneous rupture of the esophagus that is caused by a sudden increase in intraesophageal pressure, as seen in forceful vomiting. So, if the patient presents with the right symptoms and any vomiting in their history, keep this diagnosis in mind. Other causes you might see, though less common, are childbirth, seizure, prolonged coughing or laughing, or weightlifting.
ED management is essentially ABCs and broad spectrum antibiotics, and maybe even antifungals.
As soon as you make this diagnosis, get you CT surgeon on board as the length of time to definitive treatment is directly related to mortality.
Brady W et al. Electrocardiographic ST-segment elevation: the diagnosis of acute myocardial infarction by morphologic analysis of the ST segment. Acad Emerg Med 2001;8:961–7. PMID: 11581081
Bischof JE et al. ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis. Am J Emerg Med 2015 PMID: 26542793
Fromm C, et al. Diltiazem vs. Metoprolol in the Management of Atrial Fibrillation or Flutter with Rapid Ventricular Rate in the Emergency Department. J Emerg Med. 2015 Apr 22. PMID 25913166
Driver BE et al. Discharge glucose is not associated with short-term adverse outcomes in emergency department patients with moderate to severe hyperglycemia. Ann Emerg Med 2016. PMID: 27353284
In cardiac arrest, the most important interventions are to deliver electricity quickly when it’s indicated and to administer good high-quality compressions with minimal interruptions to maximize your compression fraction.
Medications like epinephrine and amiodarone have never been shown to improve good neurologic outcomes in the ACLS recommended doses. Don’t focus on them.
Consider pre-charging your defibrillator to minimize pauses in CPR and maximize your chance for ROSC
Finally, remember that as Emergency Physicians, we are specialists in the resuscitation of cardiac arrests. ACLS is just a starting point. Push your understanding of taking care of these patients so you can deliver the best care possible
Driver BE et al. Use of esmolol after failure of standard cardiopulmonary resuscitation to treat patients with refractory ventricular fibrillation. Resuscitation 2014; 85(10): 1337-41. PMID: 25033747
Hypokalemia has a wide variety of presentations ranging from generalized weakness, to paralysis, to cardiac arrhythmia or cardiac arrest.
When you discover hypokalemia, be sure to check and EKG. Think about underlying causes of hypokalemia, because it is rarely a solo event.
Treat with oral potassium supplementation of 40-60 orally every 4-6 hours for mild hypokalemia and 10-20 mEq/hour IV for severe or symptomatic hypokalemia.
DKA should be suspected in any patient with altered mental status and hyperglycemia. Get a VBG (ABG not necessary) to confirm the diagnosis.
Hypokalemia kills in DKA. Aggresively replete potassium and consider holding insulin, which drops serum potassium, until K is greater than 3.5
The insulin bolus isn’t necessary and appears to cause more episodes of hypokalemia. Just start insulin as an infusion at 0.14 units/kg
Be vigilant about cerebral edema. Any change or deterioration in mental status should prompt treatment and evaluation. Mannitol in the euvolemic, normotensive patient and 3% hypertonic saline in the hypotensive/hypovolemic patient
Finally, don’t forge to always hunt down the underlying cause of the DKA. Infection and non-compliance is the most common so liberally administer broad spectrum antibiotics if you’ve got even a hint of infection brewing
Aurora S et al. Prevalence of hypokalemia in ED patients with diabetic ketoacidosis. Am J Emerg Med 2012; 30: 481-4. PMID: 21316179
Boyd JC et al. Relationship of potassium and magnesium concentrations in serum to cardiac arrhythmias. Clin Chem 1984; 30(5): 754-7. PMID: 6713638
Duhon B et al. Intravenous sodium bicarbonate therapy in severely acidotic diabetic ketoacidosis. Ann Pharmacother 2013; 47: 970-5. PMID: 23737516
Fagan MJ et al. Initial fluid resuscitation for patients with diabetic ketoacidosis: how dry arethey? Clin Ped 2008; 47(9): 851-6. PMID:
Goyal N et al. Utility of Initial Bolus insulin in the treatment of diabetic ketoacidosis. J Emerg Med 2010; 38(4): 422-7. PMID: 18514472
Green SM et al. Failure of adjunctive bicarbonate to improve outcome in severe pediatric diabetic ketoacidosis. Ann Emergency Medicine 1998; 31: 41-48. PMID: 9437340
Kitabchi AE et al. Is a priming dose of insulin necessary in a low-dose insulin protocol for the treatment of diabetic ketoacidosis? Diabetes Care. 2008;31(11):2081. PMID: 18694978
Morris LR et al. Bicarbonate therapy in severe diabetic ketoacidosis. Ann Intern Med 1986;105(6):836. PMID: 3096181
Muir AB et al. Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification. Diabetes Care 2004; 27(7):1541-6. PMID: 15220225
Okuda Y et al. Counterproductive effects of sodium bicarbonate in diabetic ketoacidosis. J Clinical Endocrinology Metabolism 1996; 81: 314-320. PMID: 8550770
Savage MW et al. Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis. Diabet Med. 2011 May;28(5):508-15. PMID: 21255074
Villon A et al. Does bicarbonate therapy improve management of severe diabetic ketoacidosis? Crit Care Med 1999; 27: 2690-2693. PMID: 10628611
Decompensated hyperthyroidism is a rare, life-threatening condition. It can develop in patients with long-standing untreated hyperthyroidism and is often precipitated by another event such as an infection, surgery, or trauma.
Patients present with tachycardia, fever, altered mental status and GI symptoms. Keep thyroid storm in mind if a patient has a history of hyperthyroidism or if things just aren’t making sense with your patient, you can’t find a fever source, they have fever and new afib, things like that. You’re going to use a clinical scoring tool like the Burch-Wartofsky scoring system to make the diagnosis.
Treatment is three-fold. First treat the peripheral effects with propranolol. Then prevent further synthesis of thyroid hormone with PTU and corticosteroids. And last prevent the further release of thyroid hormone with iodine. Be sure to hold off on giving the iodine until at least 1 hour after the patient receives PTU to avoid worsening the hyperthyroid.
Akamizu T et al. Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys. Thyroid 2012; 22(7): 661-79. PMC: 3387770
Calver L et al. The safety and effectiveness of droperidol for sedation of acute behavioral disturbance in the Emergency Department. Ann Emerg Med 2015; 66(3): 230-8. PMID: 25890395
Baharoglu MI et al. Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral hemorrhage associated with anti platelet therapy (PAtCH): a randomized, open-label, phase 3 trial. Lancet 2016. ePub
Sales JC et al. The Importance of First Pass Success When Performing Orotracheal Intubation in the Emergency Department. Acad Emerg Med 2013; 20(1): 71-8. PMID: 23574475
Tran TP, Muelleman RL: Allergy, Hypersensitivity, Angioedema, and Anaphylaxis, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 119: p 1543-1560.
Grunau BE et al. Incidence of clinically important biphasic reactions in emergency department patients with allergic reactions or anaphylaxis. Ann Emerg Med 2014; 63(6): 736-44. PMID: 24239340
Grunau BE et al. Emergency Department Corticosteroid Use for Allergy or Anaphylaxis is Not Associated with Decreased Relapses. Ann Emerge Med 2015; 66(4): 381-9. PMID: 25820033
Wang RC. Managing Urolithiasis. Ann Emerg Med 2015 PMID: 26616536
References
Pathan SA et al. Delivering safe and effective analgesia for management of renal colic in the emergency department: a double-blind, multi group, randomized controlled trial. Lancet 2016. PMID: 26993881
Adams BK et al. Prolonged gastric emptying half-time and gastric hypo motility after drug overdose. Am J Emerg Med 2004; 22: 548-554. PMID: 15666259
Benson BE et al. Position paper update: gastric lavage for gastrointestinal decontamination. Clin Tox 2013; 51: 140-6. PMID: 23418938
Gude AB, Hoegberg LCG. Chapter 7. Techniques Used to Prevent Gastrointestinal Absorption. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e . New York, NY: McGraw-Hill; 2011.
Yip L. Chapter 77. Ethanol. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e. New York, NY: McGraw-Hill; 2011.
Howland M. Antidotes in Depth (A12): Physostigmine Salicylate. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e . New York, NY: McGraw-Hill; 2011.
Velez LI, Feng SY: Anticholinergics, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 150: p 1970-5.
Gorchynski J et al. The “syringe” technique: a hands-free approach for the reduction of acute nontraumatic temporomandibulardislocations in the emergency department. J Emerg Med. 2014; 47(6):676-81. PMID 25278137
Irazuzta JE et al. High-dose magnesium sulfate infusion for severe asthma in the emergency department: efficacy study. Crit Care Med 2016; 17: e29-e33. PMID: 26649938
Peterson D et al. Predictors of Failure of Empiric Outpatient Antibiotic Therapy in Emergency Department Patients with Uncomplicated Cellulitis. Acad Emerg Med 2014; 21: 526-31. PMID: 24842503
Talan DA et al. Trimethoprim-Sulfamethoxazole versus placebo for uncomplicated skin abscesses. NEJM 2016; 374(9): 823-32. PMID: 26962903
Chinnock B, Hendey GW. Irrigation of cutaneous abscesses does not improve treatment success. Ann Emerg Med 2016; 67(3): 379-83. PMID: 26416494
Nishijima DK et al. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and perjury warfarin or clopidogrel use. Ann Emerge Med 2012; 59(6): 460-8. PMID: 22626015
Menditto VG et al. Management of minor head injury in patients receiving oral anticoagulant therapy: a prospective study of a 24-hour observation protocol. Ann Emerg Med 2012; 59(6): 451-5. PMID: 22244878
Miller J et al. Delayed intracranial hemorrhage in the anticoagulated patient: a systematic review. J Trauma Acute Care Surg 2015; 79: 310-3. PMID: 26218702
Beigi, R.H. (2015). Epidemiology, clinical manifestations, and diagnosis of tuboovarian abscess. In S.J. Falk (Ed.), UpToDate. Waltham, MA, 2015.
Beigi, R.H. (2015). Management and complications of tuboovarian abscess. In S.J. Falk (Ed.), UpToDate. Waltham, MA, 2015.
Hart, D, Lipsky, A. Acute Pelvic Pain in Women. In: Marx JA, ed. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014. p. 266-272.
Lee D, Swaminathan A. Sensitivity of Ultrasound for the Diagnosis of Tubo-Ovarian Abscess: A Case Report and Literature Review. J Emerg Med. 2011 vol 40 (2): 170-5. PMID: 20466506
Schwartz DT. Section 5. Cervical Spine. In: Schwartz DT: Emergency Radiology: Case Studies. New York, NY: McGraw-Hill, 2008. http://accessemergencymedicine.mhmedical.com/ (via NYU Health Sciences Library)
Fanari Z et al. Aggressive measures to decrease “door to balloon” time and incidence of unnecessary cardiac catheterization: potential risks and role of quality improvement. Mayo Clin Proc 2015. PMID: 26549506
Del Portal DA et al. Emergency department management of shoulder dystocia. J Emerg Med. 2014 Mar;46(3):378-82. PMID: 24360351
Lew GH, Pulia MS: Emergency Childbirth, in Roberts JR, Hedges JR, Custalow CB, et al (eds): Clinical Procedures in Emergency Medicine, ed 6. Philadelphia, Saunders, 2013, Ch 56:p 1155-82.
Drugs for the Management of Uterine Atony – Roberts + Hedges
Sluga M, Ummenhofer W, Studer W, Siegemund M, Marsch SC. Rocuronium versus succinylcholine for rapid sequence induction of anesthesia and endotracheal intubation: a prospective, randomized trial in emergent cases. Anesth Analg 2005; 101:1356 – 61.
McCourt KC, Salmela L, Mirakhur RK, et al. Comparison of rocuronium and suxamethonium for use during rapid sequence induction of anaesthesia. Anaesthesia 1998;53:867–71.
Laurin EG, Sakles JC, Panacek EA, Rantapaa AA, Redd J. A comparison of succinylcholine and rocuronium for rapid-sequence intubation of emergency department patients. Acad Emerg Med 2000;7:1362–9.
Herbstritt A. BET 3: Is rocuronium as effective as succinylcholine at facilitating laryngoscopy during rapid sequence intubation. Emerg Med J 2012; 29(3): 256-9.
Taha SK et al. Effect of suxamethonium vs rocuronium on onset of oxygen desaturation during apnoea following rapid sequence induction. Anaesthesia 2010; 65: 358-61.
Tang L et al. Desaturation following rapid sequence induction using succinylcholine vs. rocuronium in overweight patients. Acta Anaesthesiol Scand 2011; 55: 203-8.
Bessman ES: Emergency Cardiac Pacing, in Roberts JR, Hedges JR, Custalow CB, et al (eds): Clinical Procedures in Emergency Medicine, ed 6. Philadelphia, Saunders, 2013, Ch 15:p 277-300.
Tibbling L et al. Effect of spasmolytic drugs on esophageal foreign bodies. Dysphagia 1995; 10(2): 126-7. PMID: 7600855
Samuel M. Pediatric appendicitis score. J Pediatr Surg 2002; 37(6): 877-81. PMID: 12037754
Ross MJ et al. Outcomes of children with suspected appendicitis and incompletely visualized appendix on ultrasound. Acad Emerg Med 2015; 21(5): 538-42. PMID: 24842505
Parienti JJ et al. Intravascular complications of central venous catheterization by insertion site. NEJM 2015. PMID: 26398070
Appleboam A et al. Postural mdodification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised trial. Lancet 2015. PMID: 26314489
Jefferson T et al. Oseltamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ 2014. PMID: 24811411
Dobson J et al. Oseltamivir treatment for influenza in adults: a meta-analysis of randomised controlled trials. Lancet 2015; 385(9979): 1729-37. PMID: 25640810
Foreign Body Aspiration
Brown JC et al. The utility of adding expiratory of decubitus chest radiographs to the radiographic evaluation of suspected pediatric airway foreign bodies. Ann Emerg Med 2013; 61: 19-26. PMID: 22841172
Foltran F et al. Foreign bodies in the airways: a meta-analysis of published papers. Int J Pediatric Otorhinolaryngol 2012; 76 Suppl 1: S12-9. PMID: 22333317
Platz, F. and Kopiez, R., “When the first impression counts: Music performers, audience, and the evaluation of stage entrance behavior”, Musicae Scientiae 17, No. 2 (2013), pp. 167-197
Acad Emerg Med. 2012 Oct;19(10):1166-72. Epub 2012 Oct 4. Predictors of parent satisfaction in pediatric laceration repair. Lowe DA, Monuteaux MC, Ziniel S, Stack AM.
Proc Natl Acad Sci U S A. 2013 Sep 3;110(36):14580-5. Epub 2013 Aug 19.
Sight over sound in the judgment of music performance. Tsay CJ.
Med Educ. 2013 Aug;47(8):842-50. Music lessons: revealing medicine’s learning culture through a comparison with that of music. Watling C, Driessen E, van der Vleuten CP, Vanstone M, Lingard L.
The New Yorker. October 3, 2011. Personal Best. Top athletes and singers have coaches. Should you? Atul Gawande.
ANZ J Surg. 2013 Jun;83(6):477-80. Epub 2013 Apr 26.
Improving the impact of didactic resident training with online spaced education. Gyorki DE, Shaw T, Nicholson J, Baker C, Pitcher M, Skandarajah A, Segelov E, Mann GB.
Psychol Sci Public Interest. 2013 Jan;14(1):4-58. Improving Students’ Learning With Effective Learning Techniques: Promising Directions From Cognitive and Educational Psychology. Dunlosky J, Rawson KA, Marsh EJ, Nathan MJ, Willingham DT.
Resuscitation. 2010 May;81(5):631. Epub 2010 Feb 26.
The use of popular audio in CPR (TUPAC)–Does music improve compliance with recommended chest compression rates? Naushaduddin M, Holdgate A, Ung S.
Science. 1965 Nov 19;150(3699):971-9. Pain mechanisms: a new theory. Melzack R, Wall PD.
http://www.dailymail.co.uk/news/article-2715109/Despite-pain-half-mothers-enjoy-childbirth-admit-differently-time.html
Pediatr Emerg Care. 2008 Dec;24(12):836-8. Emergency department waiting room stress: can music or aromatherapy improve anxiety scores? Holm L, Fitzmaurice L.
Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis.
(Hole Lancet 2015). 72 randomized trials.
Lancet. 2015 Aug 12. Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis. Hole J, Hirsch M, Ball E, Meads C.
.
Ann Emerg Med. 1991 Apr;20(4):348-50. A randomized, controlled trial of the use of music during laceration repair. Menegazzi JJ, Paris PM, Kersteen CH, Flynn B, Trautman DE.
Anaesthesia. 1992 May;47(5):438-9. The effect of music on ketamine induced emergence phenomena. Kumar A, Bajaj A, Sarkar P, Grover VK.
Cochrane Database Syst Rev. 2013 Oct 25;10:CD004843. Music for pain relief. Cepeda MS, Carr DB, Lau J, Alvarez H.
Cochrane Database Syst Rev. 2014;12:CD006902. doi: 10.1002/14651858.CD006902.pub3. Epub 2014 Dec 9. Music interventions for mechanically ventilated patients. Bradt J, Dileo C.
Read More
Episode 18.0 – Influenza Testing + Epistaxis
Oct 19, 2015
This week we discuss some information on influenza testing in the ED and management of epistaxis.
Zahed R et al. A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med 2013; 31: 1389-92. PMID: 23911102
Derkay CS et al. Posterior nasal packing. Are Intravenous antibiotics really necessary? Arch Otolaryngol 1989; 115: 439-41. PMID: 2923686
Pepper C et al. Prospective study of the risk of not using prophylactic antibiotics in nasal packing for epistaxis. J Laryng Otology 2012: 257-9. PMID: 22214602
Biggs TC et al. Should prophylactic antibiotics be used routinely in epistaxis patients with nasal packs? Ann R Coll Surg Engl 2013; 95: 40-2. PMID: 23317726
Mittal MK et al. A clinical decision rule to identify infants with apparent life-threatening event who can be safely discharged from the emergency department. Pediatr Emerg Care 2012; 28(7): 599-605. PMID: 22743742
Kaji AH et al. Apparent life-threatening event: multi center prospective cohort study to develop a clinical decision rule for admission to the hospital. Ann Emerg Med 2013; 61(4): 379-87. PMID: 23026786
Asha SE, Miers JW. A systematic review and meta-analysis of D-dimer as a rule-out test for suspected acute aortic dissection. Ann Emerg Med 2015. PMID: 25805111
Dierks DB et al. Clinical policy: critical issues in the evaluation and management of adult patients with suspected acute nontraumatic thoracic aortic dissection. Ann Emerg Med 2015; 65: 32-42. PMID: 25529153
Acid-Base Cases
Quick questions & answers:
For acute respiratory acidosis or alkalosis, how much does the pH change for every 10mm change of PCO2?
What is the Winter’s formula?
For stable chronic respiratory acidosis, for every 10 mm increase in PCO2, how much should the pH decrease by?
For each of the following cases, please analyze the acid-base status (i.e. anion gap metabolic acidosis, respiratory alkalosis, non-AG metabolic acidosis with respiratory acidosis, etc…) for further discussion in the workshop.
1) A 25 year old woman is found at home c/o thirst, shortness of breath, and spasms of her arms and legs.
Vital signs: BP 90/50 mmHg; pulse 155/min; RR 32/min; afebrile; RA O2 sat 98%.
137 84 18 274 Calcium 9.6
2.4 29 1.2
VBG: 7.66 / 25.5 / 29.1
What is the acid base abnormality?
What abnormality is responsible for her neuromuscular symptoms?
What other electrolyte abnormalities would you expect?
How should she be treated?
2) A 21 yo female presented to ED after reportedly ingesting an entire bottle of pills (drug and formulation unknown) and now complaints oftinnitus, nausea, and vomiting.
Exam: A, O x3, Pupils – dilated, reactive, Neuro – no hyperreflexia, rigidity or clonus
VS: BP 92/67, HR 100/min, RR 18/min, T 98.6, RA O2 sat 99%
135 104 12 145
3.8 11 0.9 Ca 7.8
ABG: 7.47 / 14 /109 /10
3) A 56 yo female with a past medical history of heroin use (on methadone maintenance therapy) and chronic ETOH use presents with chest pain, shortness of breath, body aches, as well as nausea, vomiting and diarrhea.
VS: BP 164/84, HR 112/min, RR 22/min, T 98, RA O2 sat 98%
MS – awake, alert and oriented x2, CV – tachycardic, RR no m, abd nl, skin nl
136 98 7 277
3.4 19 0.9
4) 53 y/o M referred to the ED for severely elevated BP of 235/135. He c/o 1 week of polydipsia, polyuria, fatigue, and some dyspnea on exertion.
No known PMH but has no doctor evaluation for many years.
VS: BP 191/94, HR 88/min, RR 18/min, T 97.4
143 89 23 253
2.3 45 1.0
ABG: 7.56 / 53.6 / 65.4 lactate 3.2
5) A 62 y/o M with h/o stage IIIa rectal ca s/p diverting ileostomy 5 months ago & currently on chemotherapy presented with 3 days of repeated vomiting, watery diarrhea, and generalized weakness.
VS: BP 80/47, HR 100/min, RR 26/min, T 95o, RA O2 sat 96%
6) 66 y/o M presented to the ED because of alcohol withdrawal.
VS: BP 144/98, HR 130/min, RR 22/min, T 98.3, RA O2 sat 97%
141 102 8 85 ABG on O2 7.45 / 24 / 136
4.3 13 0.7
7) A 32 y/o F with hx of DM x 20 yrs on canagliflozin presented to the ED c/o polyuria x 2 days, epigastric pain, and not feeling well.
VS: BP 139/77, HR 112/min, RR 32/min, T 98.5, RA O2 sat 99%
135 104 17 191
3.4 3 0.4 7.06 / 11 / 125
8) A 55 y/o M with history of asthma but non-compliant with all medications and follow up presented to the ED with asthma exacerbation over the past few days. He appears to be SOB, able to speak to you & complete his sentences. + mild accessory muscle usage, mild wheezing
VS: BP 150/90, P = 115/min, R = 30/min, T = 98 , RA O2 sat 87%
ABG: 7.22 / 85 / 55
143 102 25 99
——————————
3.8 36 1.3
9) A 70 y/o M with h/o COPD presented with 2 days of vomiting and weakness.
VS: BP 150/ 85, HR 100/min, RR 18/min , T 99, RA O2 sat 90%
136 85 28 65 7.19 / 60 / 55 bicarb 25
——————————-
4.1 25 1.4 AST/ALT 150 / 100 Alb 2.5
10) A 37 y/o M presents to the ED in a coma.
VS: BP 110/80, HR 125/min, RR 30/min, T 97, O2 sat 99% on RA
Rowh AD et al. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med 2015. 48(3):325-330. PMID: 25524455
Hagan PG et al. The international registry of acute aortic dissection (IRAD): New insights into an old disease. JAMA 2000; 283: 897-903. PMID: 10685714
Rosman HS et al. Quality of history taking in patients with aortic dissection. Chest 1998; 114(3): 793-5. PMID: 9743168
Vaillancourt S. et al. Repeated Emergency Department Visits Among ChildrenAdmitted With Meningitis or Septicemia: A Population-Based Study. Ann Emerg Med 2015; 65(6): 625-631. PMID: 25458981
Backus BE et al. Risk Scores for Patients with Chest Pain: Evaluation in the Emergency Department. Curr Card Rev 2011; 7: 2-8. PMC: 3131711
Mahler SA et al. The HEART Pathway Randomized Trial Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge. Circ Cardiovasc Qual Outcomes March 2015; 8 (2): 195 – 203. PMID: 25737484
The HEART Pathway (Mahler 2015)
Journal Update
Goldberg H et al. Oral steroids for actue radiculopathy due to a herniated disk – a randomized clinical trial. JAMA 2015; 313(19): 1915-23. PMID: 25988461
Know your local antibiogram. This is the best way to tailor your management to your patient.
Search for recent old cultures from your patients and order antibiotics based on this information.
Skin + Soft Tissue Take Home Points
Antibiotics aren’t required for most simple abscesses. I+D and if no overlying cellulitis, no antibiotics needed.
Not all abscesses need packing. If they’re small and on the extremeties, it’s reasonable to leave them unpacked.
Not all patients need MRSA coverage for cellulitis. Most cellulitis without abscess is strep.
Necrotizing Fasciitis can be tough to pick up. The LRINEC scoring system is one method to help. Most patients will be toxic but look for pain that’s out of proportion to the examination.
Episode 1.1 – Jay Lemery on Wilderness Medicine in 2015
Jun 22, 2015
This talk was given by Jay Lemery in May 2015 when he came out from Denver for Grand Rounds. Jay is an associate professor of EM at Denver Health as well as the past president of the Wilderness Medicine Society. This talk is about what Wilderness Medicine is in 2015. "Wilderness Medicine is about providing care in austere environments."
Episode 1.0 – Electrical and Lightning Injuries
May 09, 2015
This podcast highlights pearls and take home points from Chris McStay's grand rounds talk on Electrical and Lightning Injuries from our Wilderness Medicine Grand Rounds on May 6th, 2015.
Episode 0.0: Intro to the Core EM Podcast. Every Monday we'll release a podcast featuring pearls, pitfalls and critical take home messages from our weekly resident conference.
 Stay Connected
Stay Connected














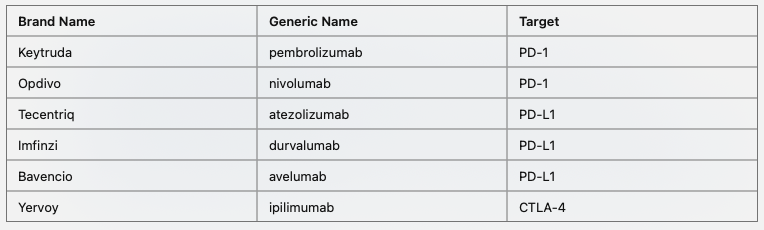
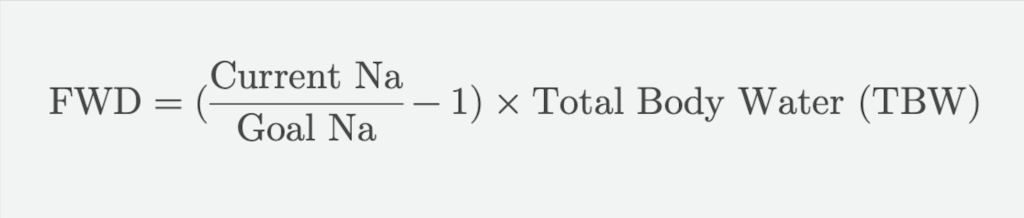

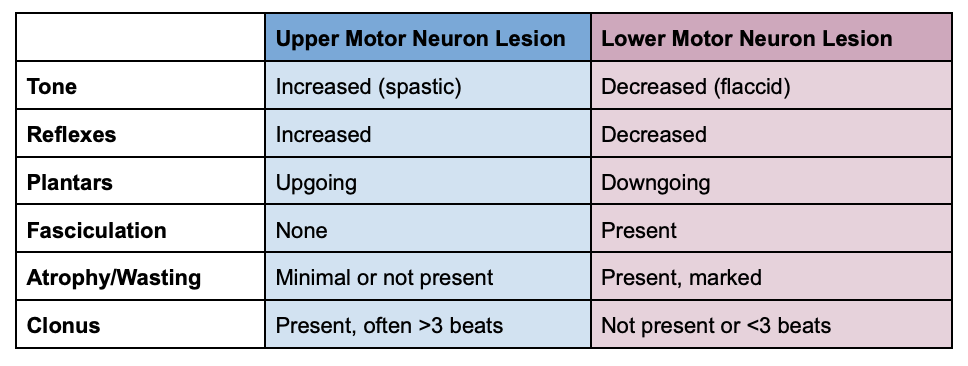
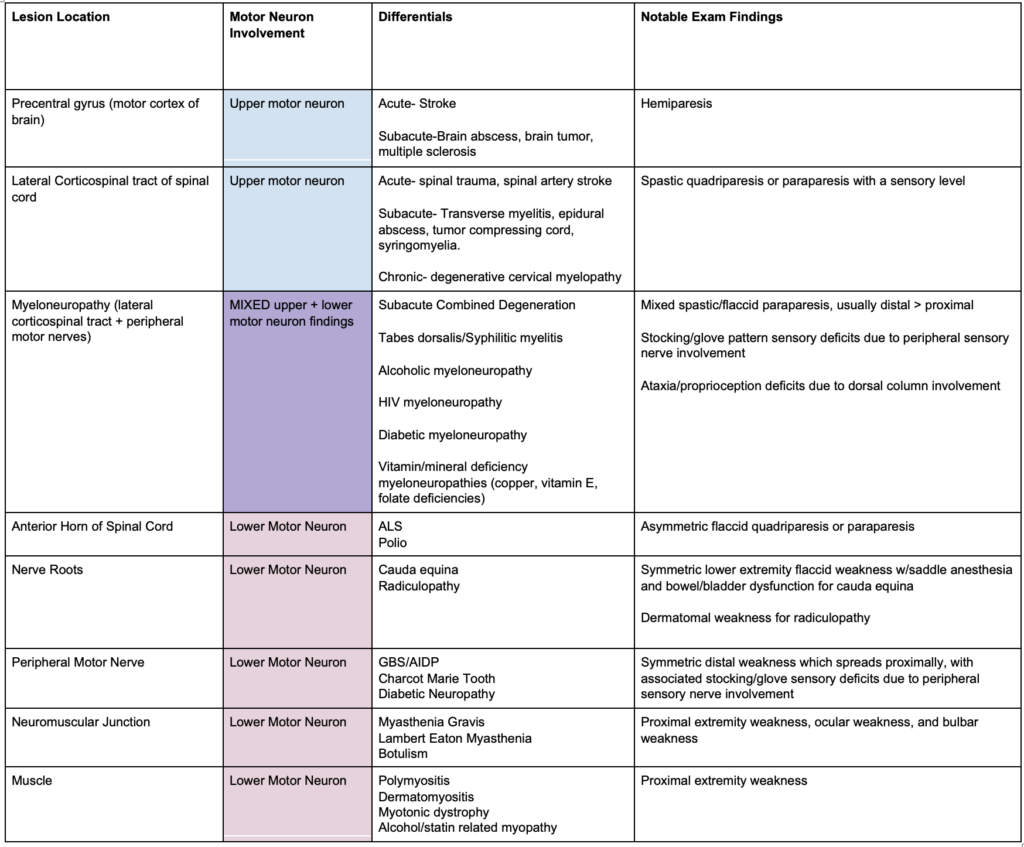


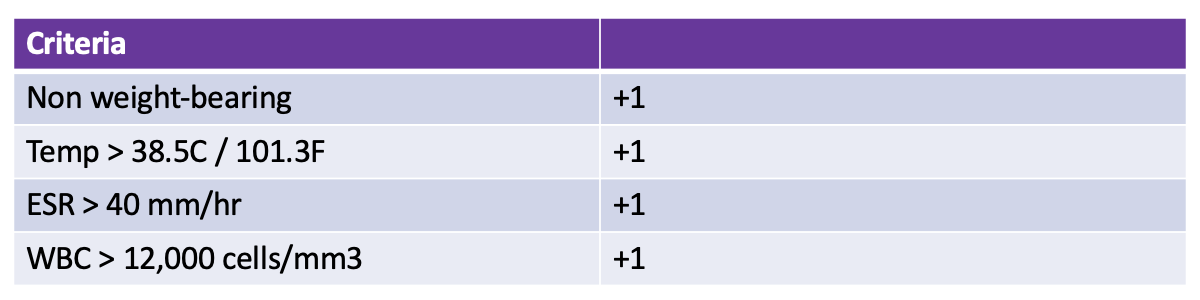
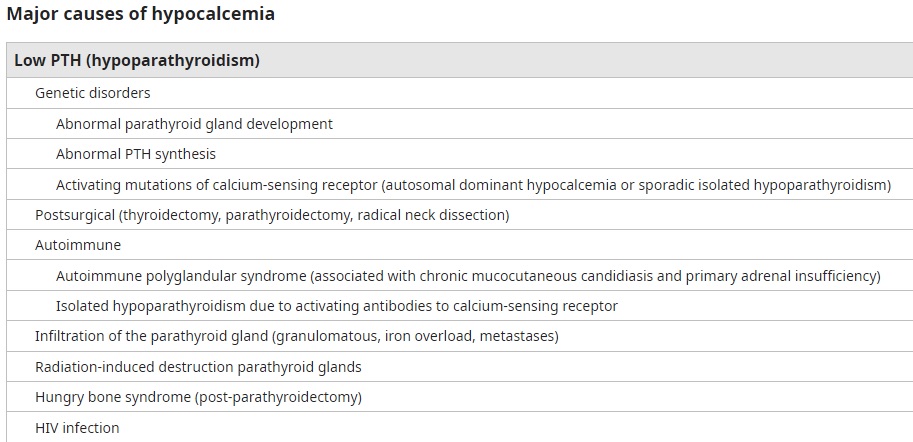
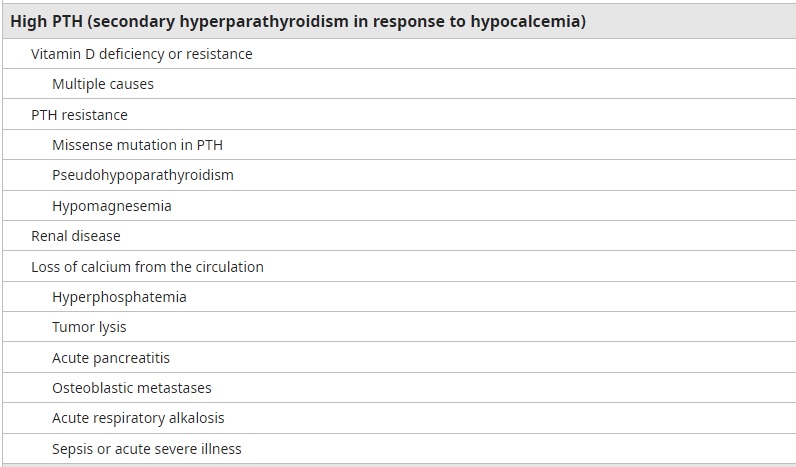
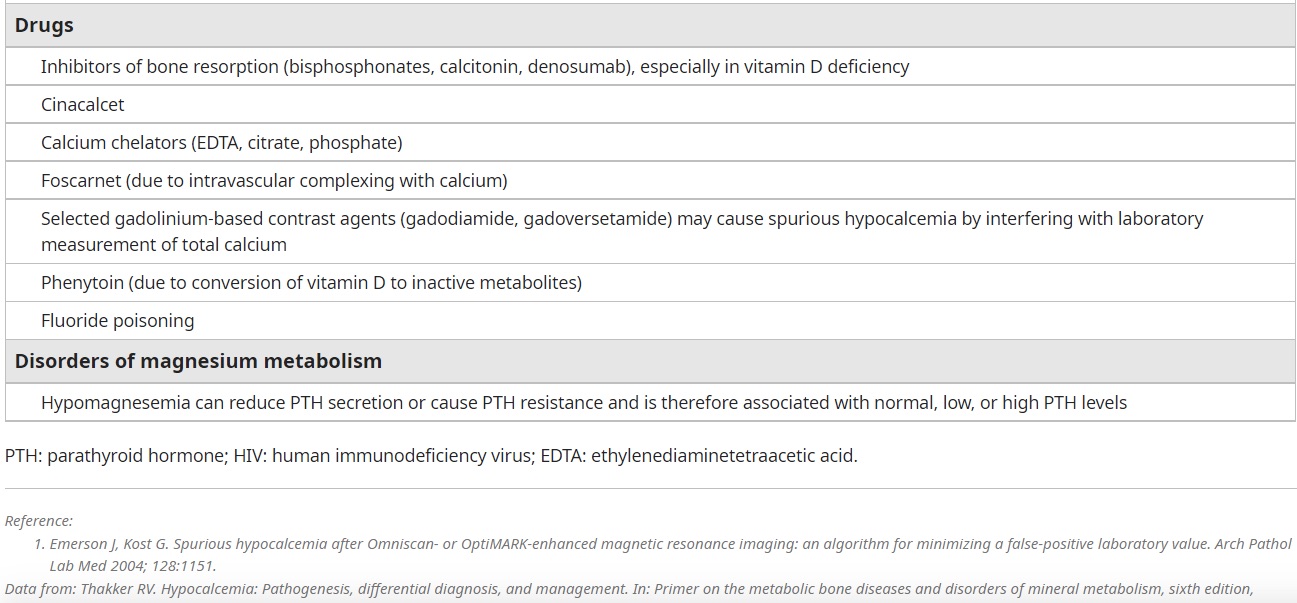

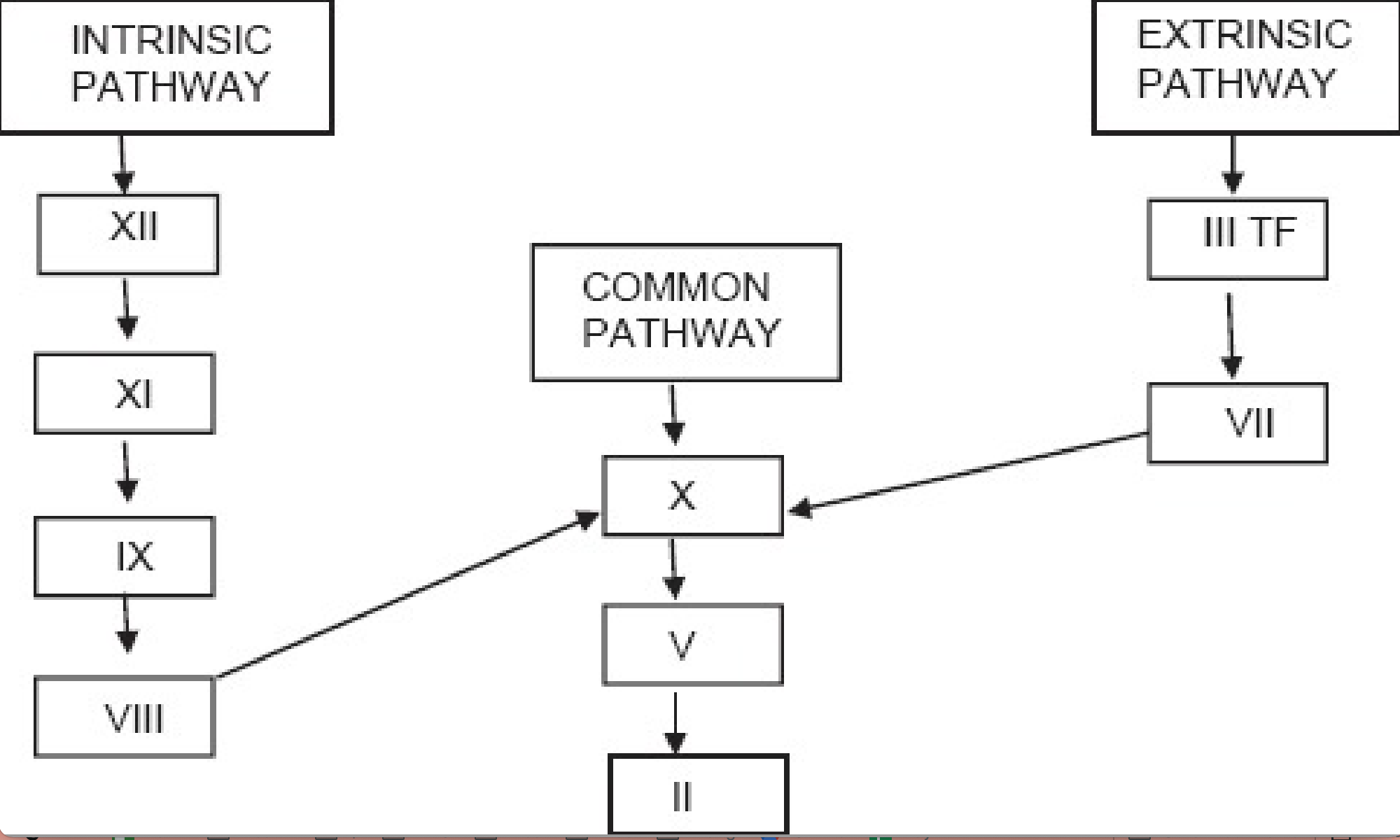
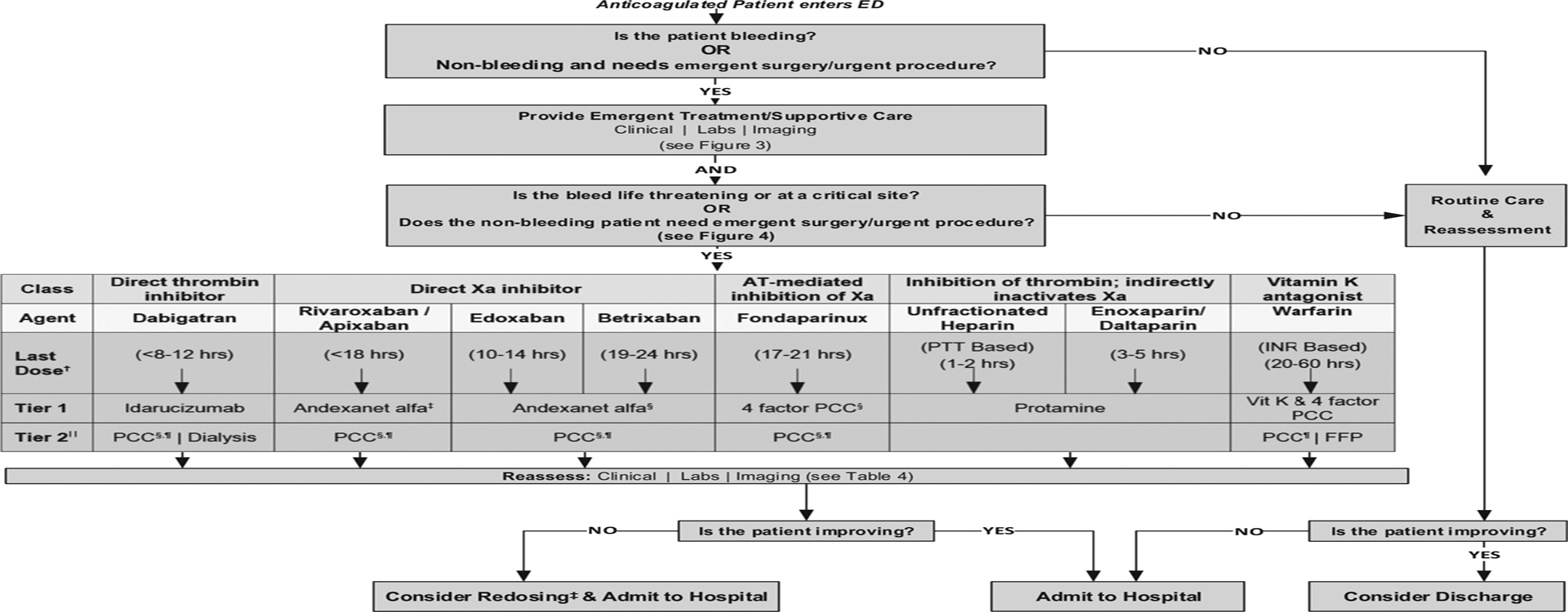
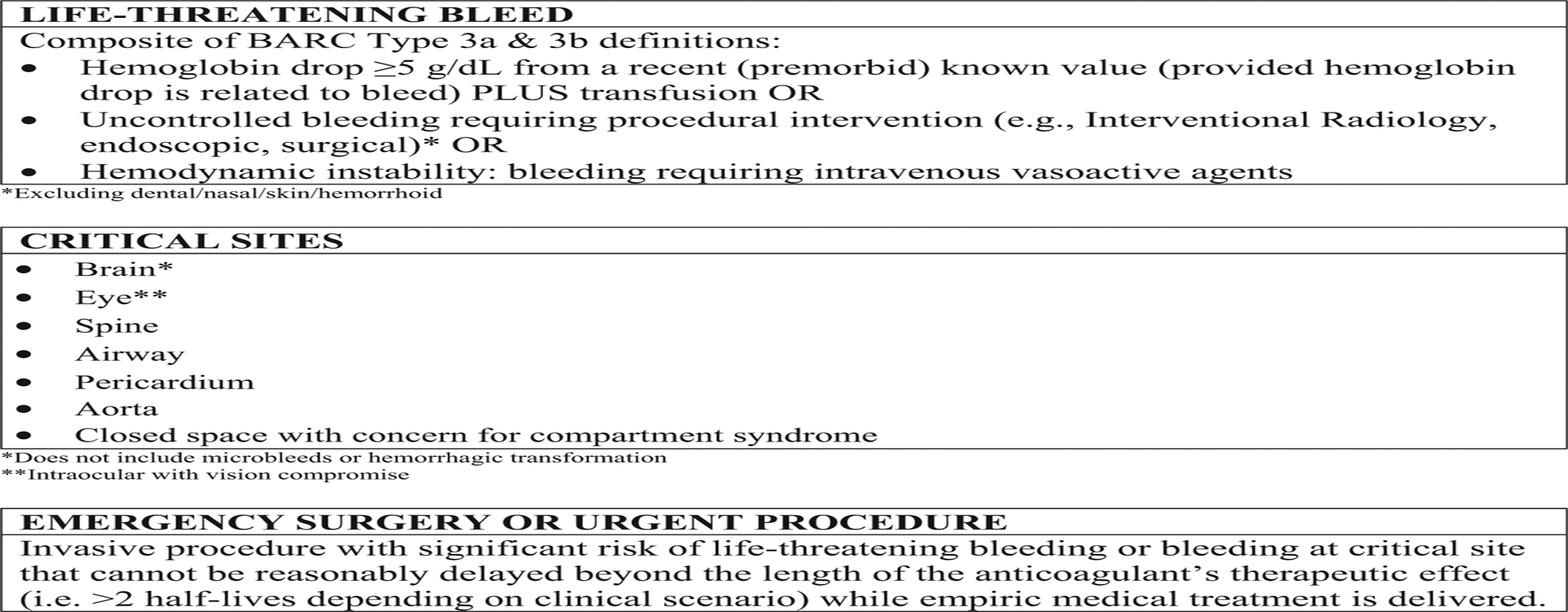
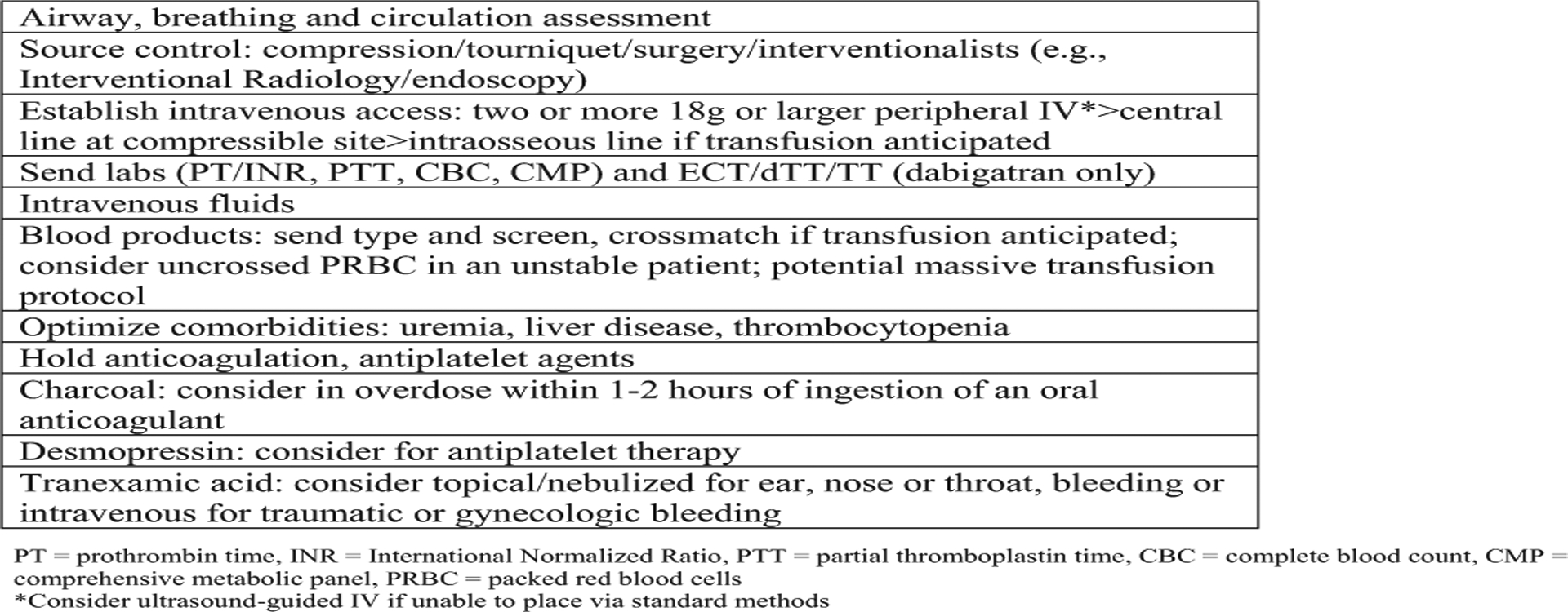

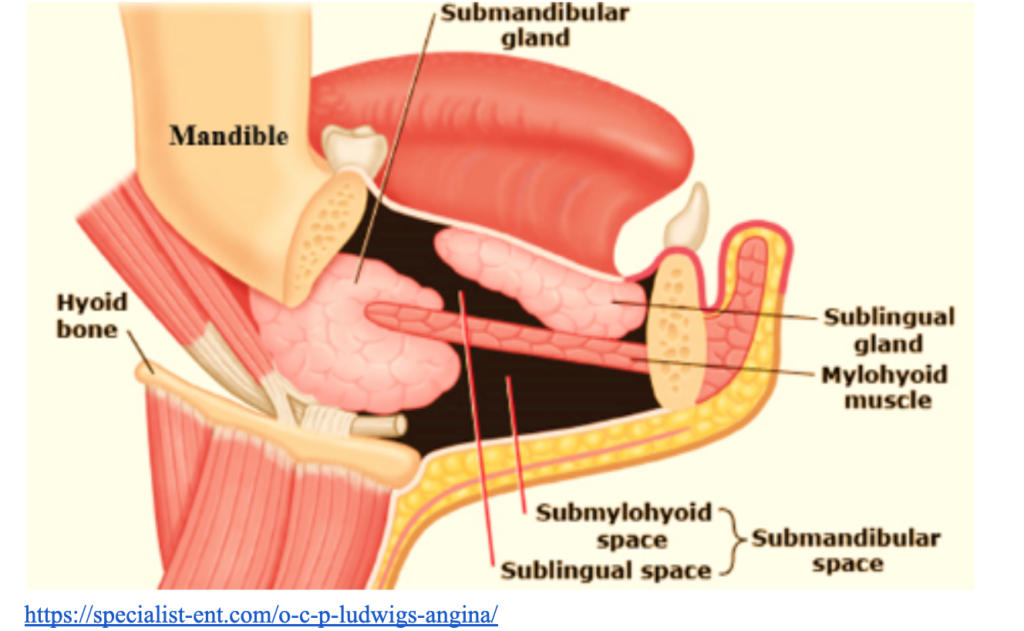

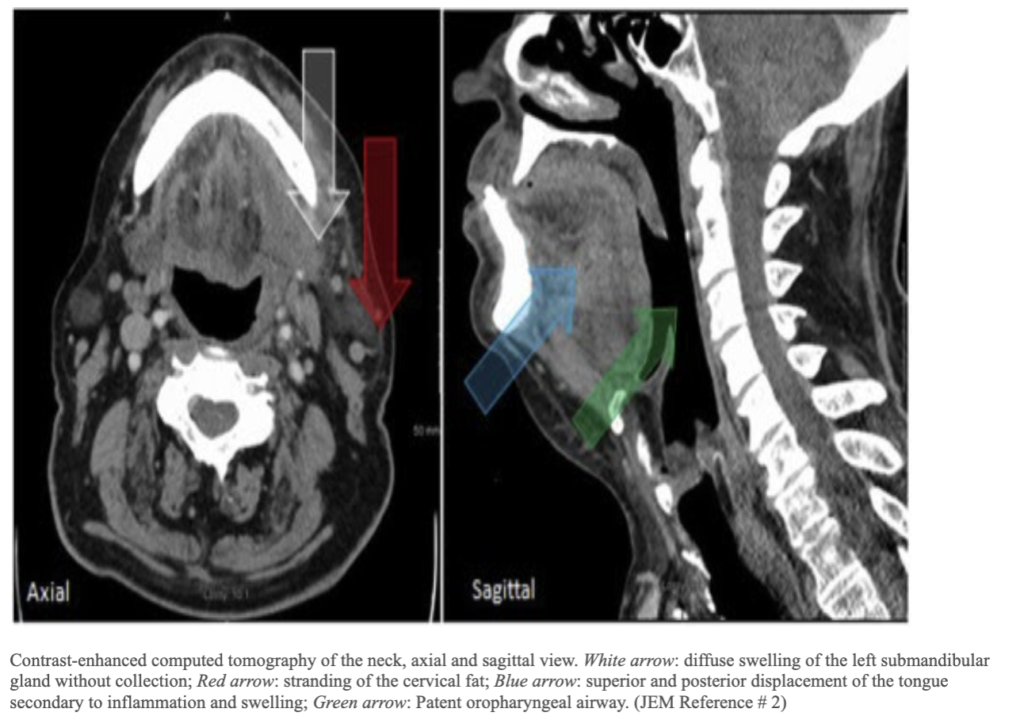
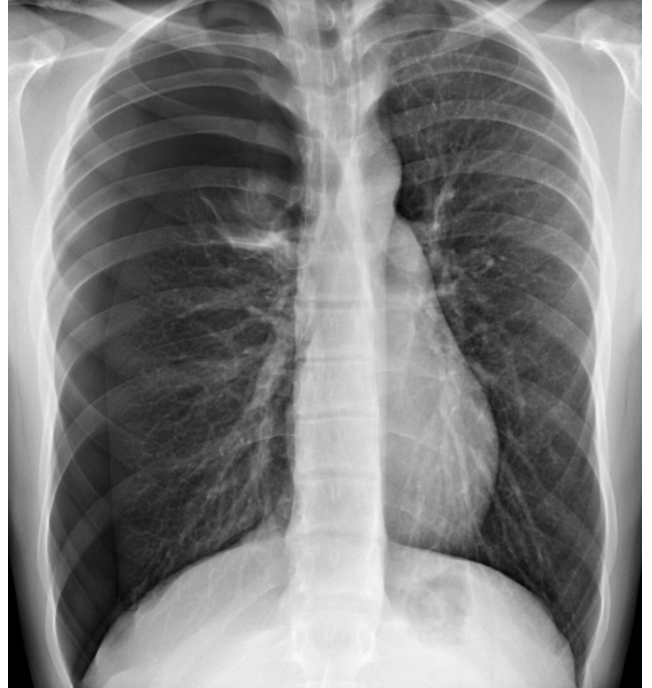
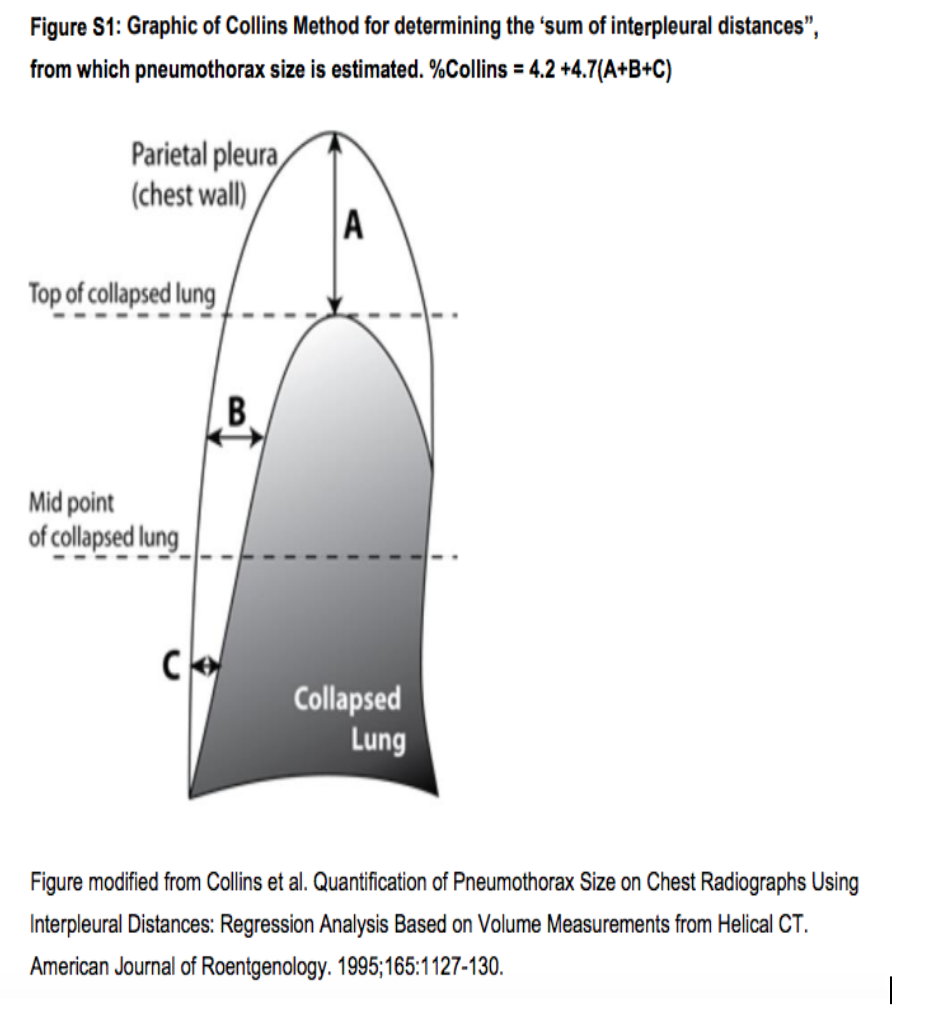
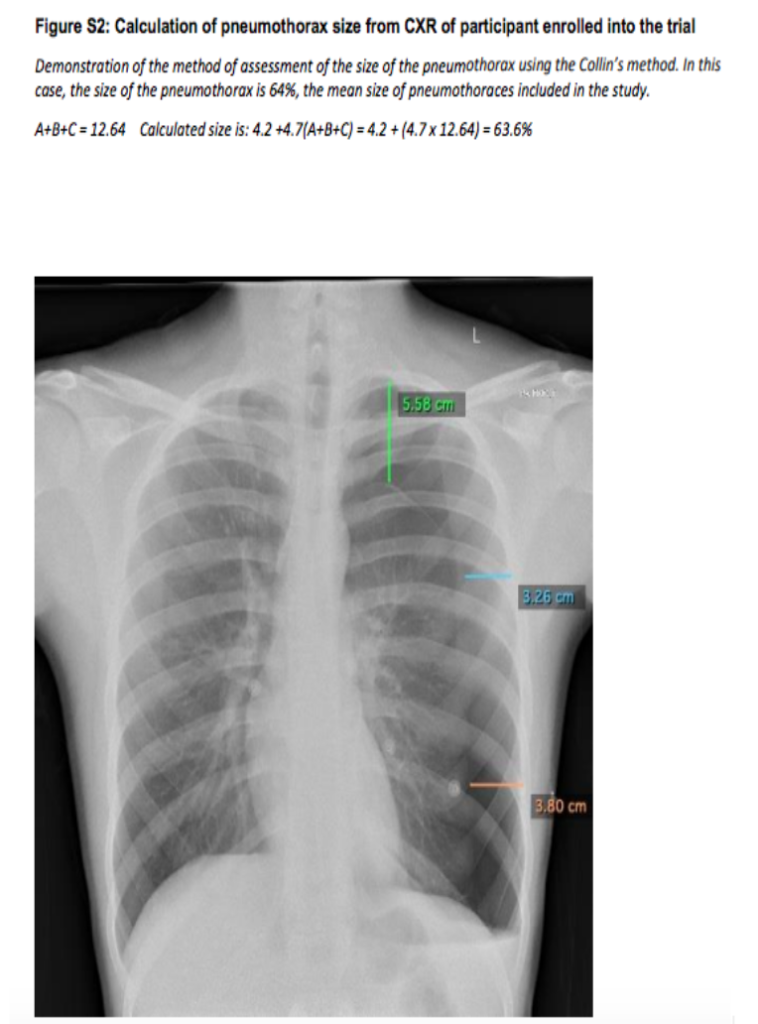
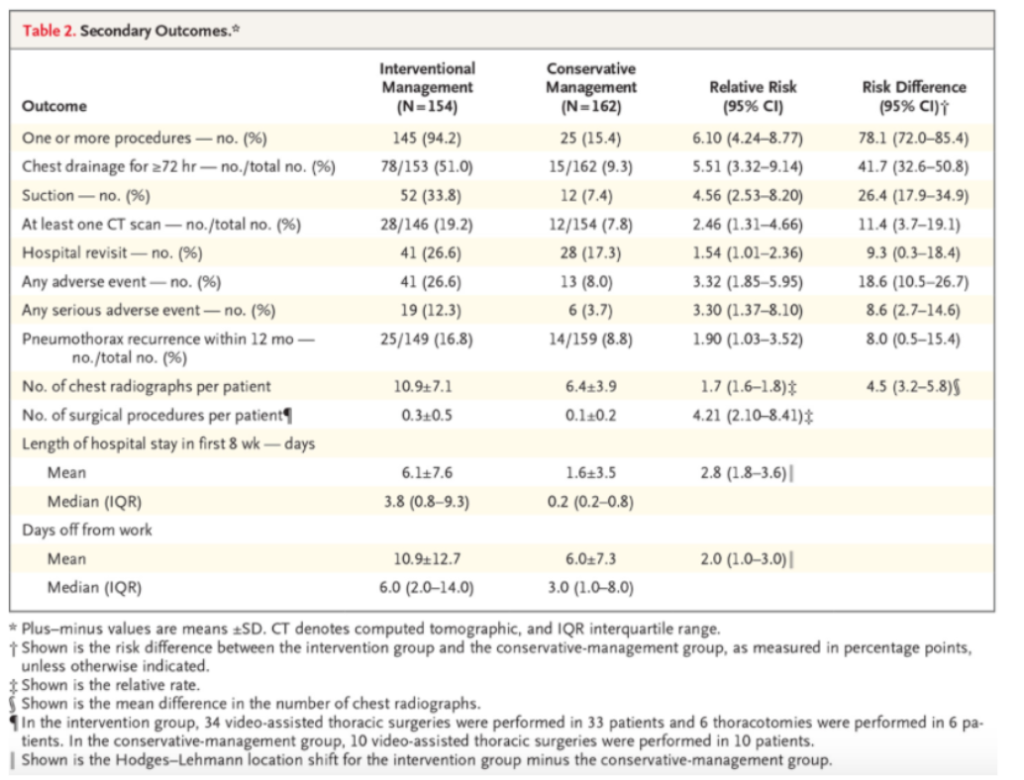
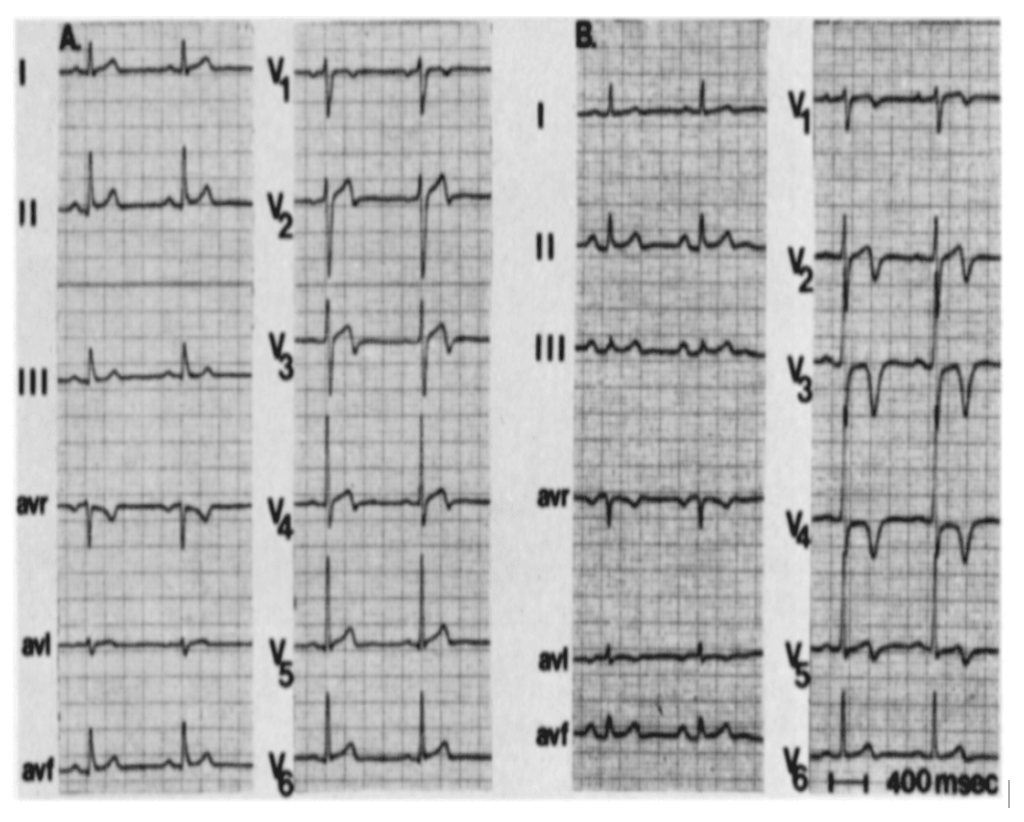
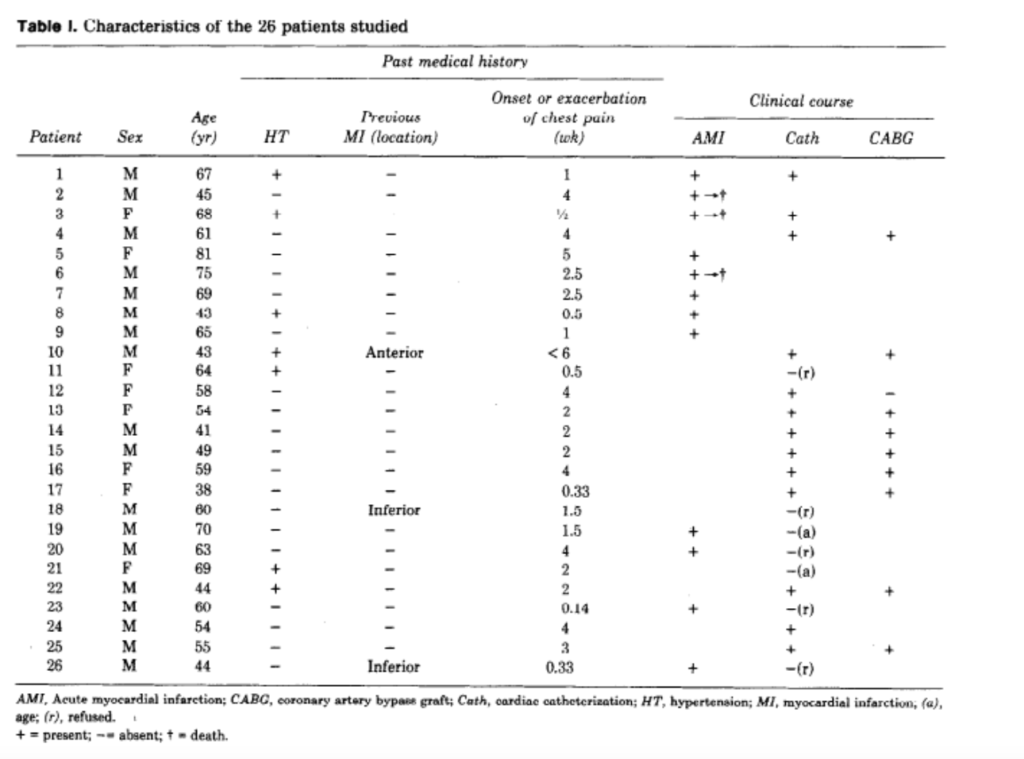
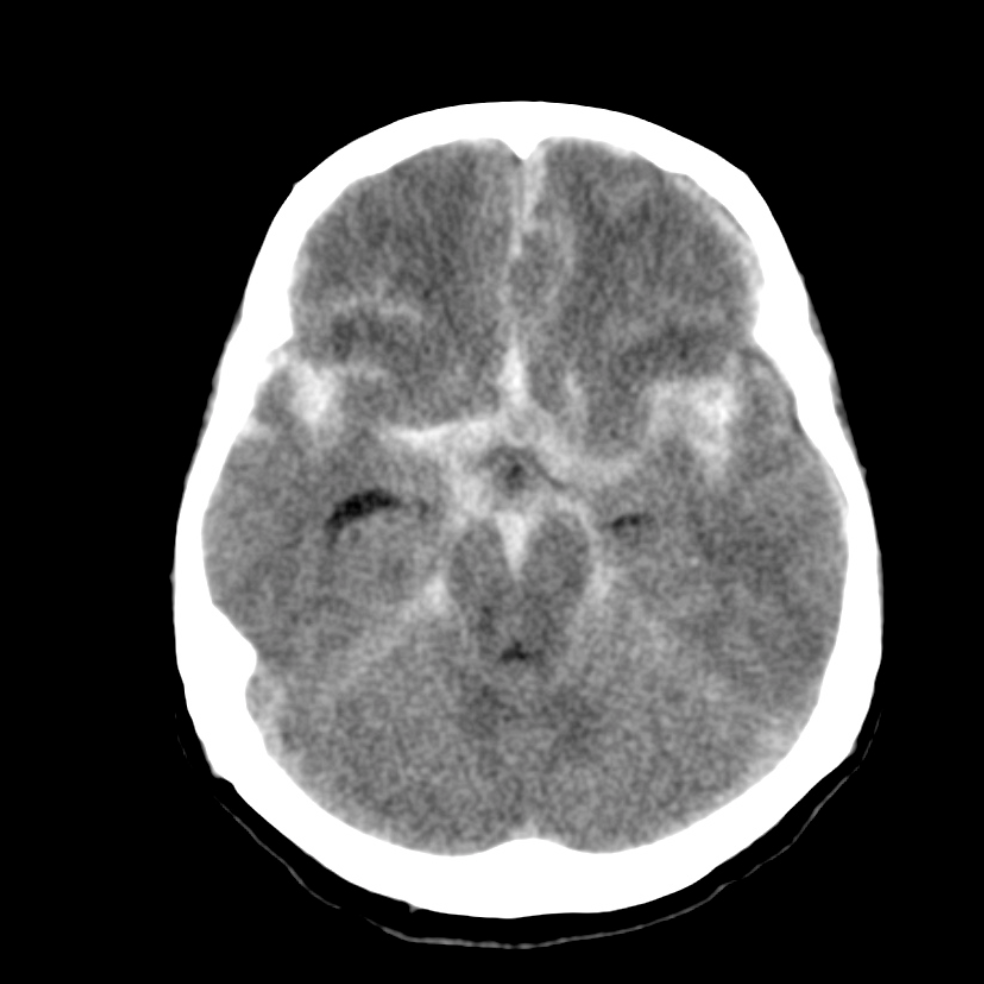
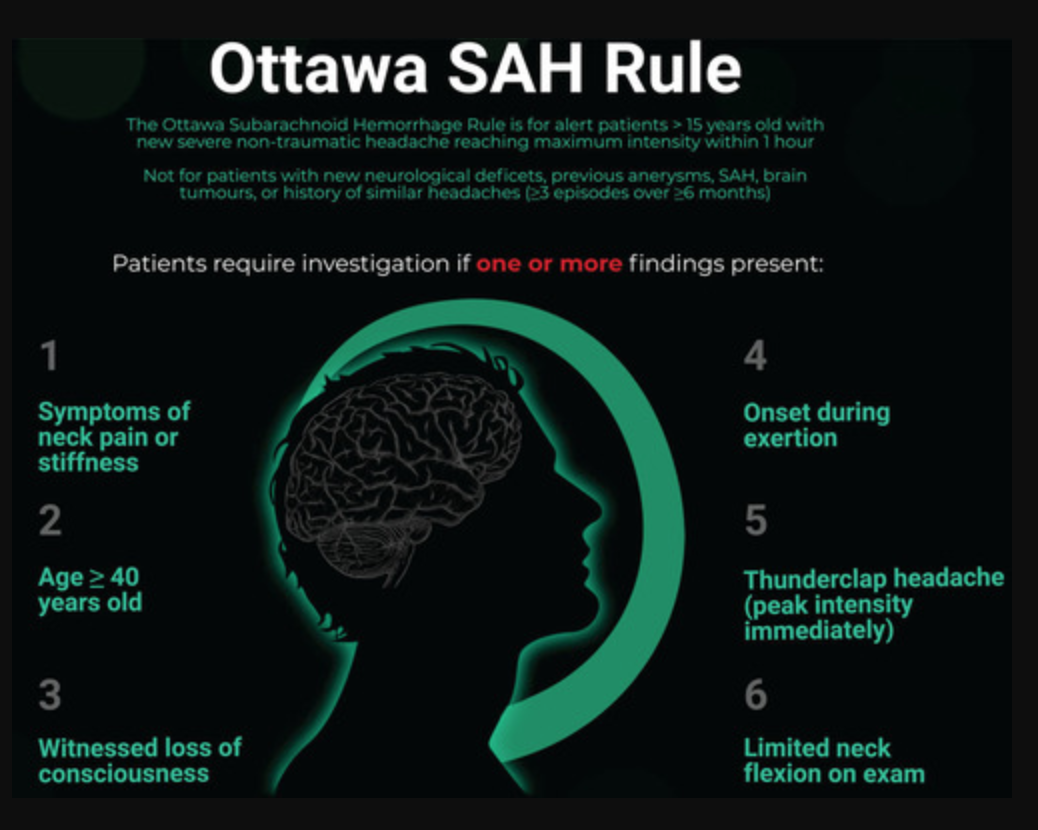

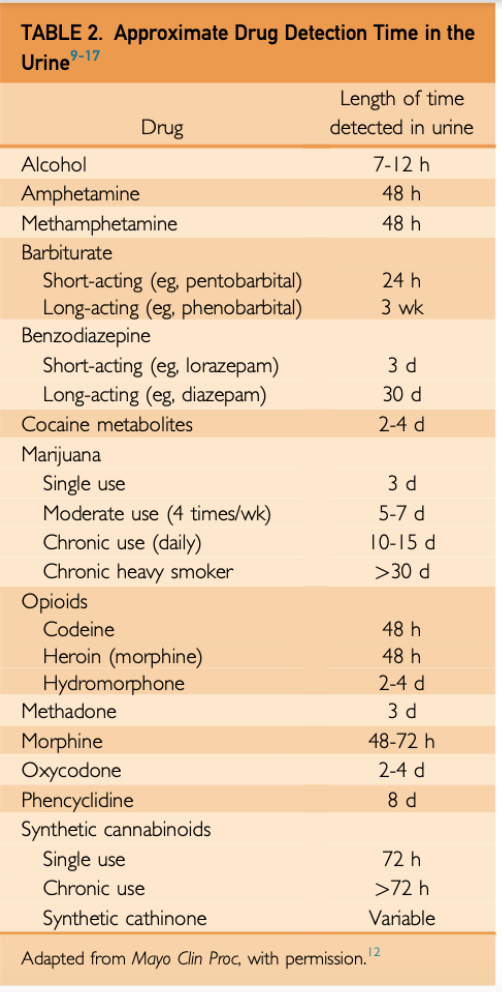
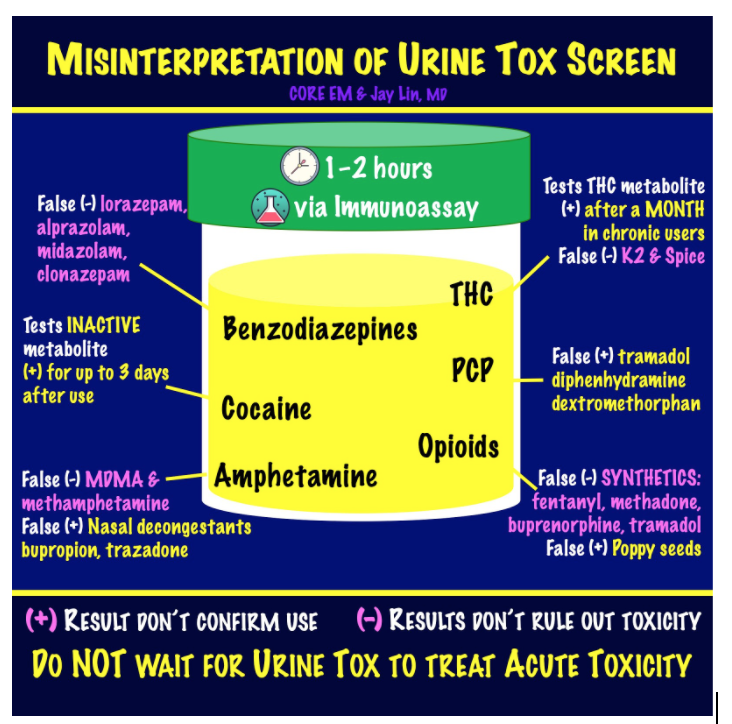
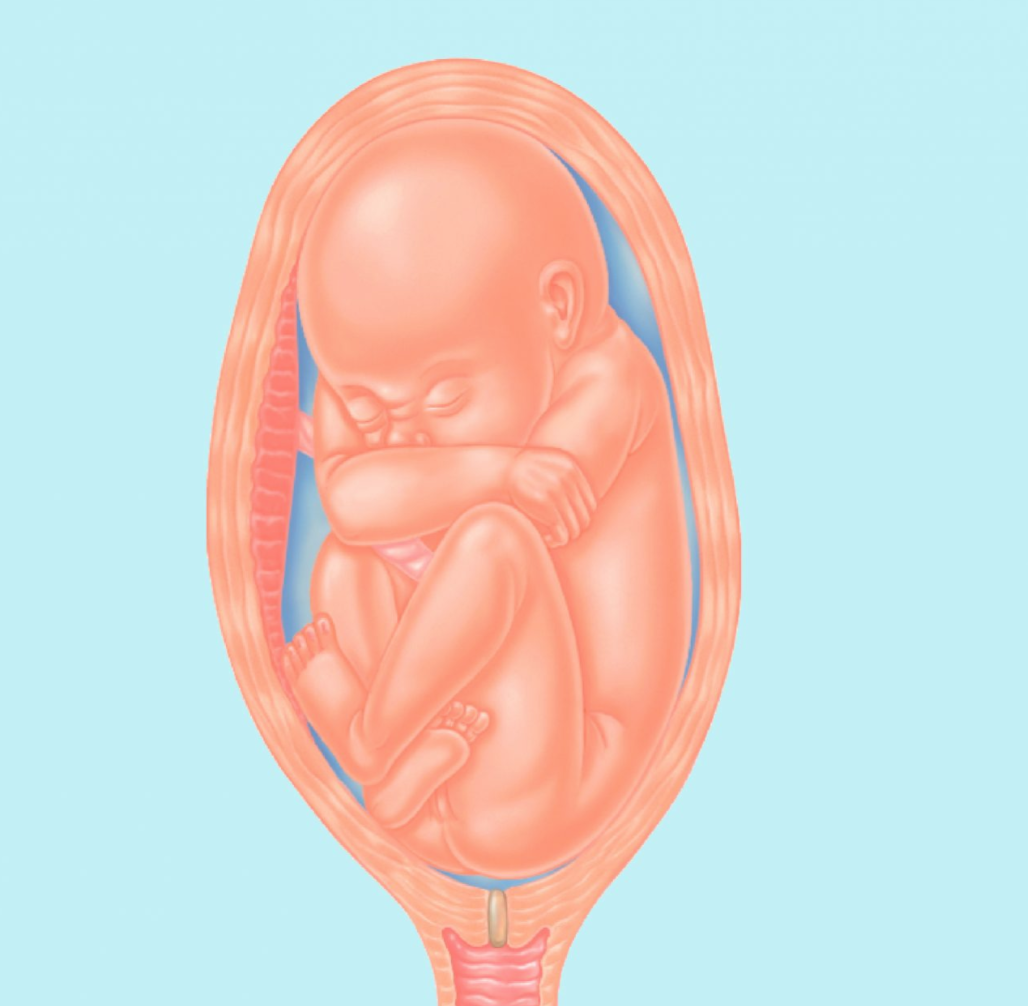
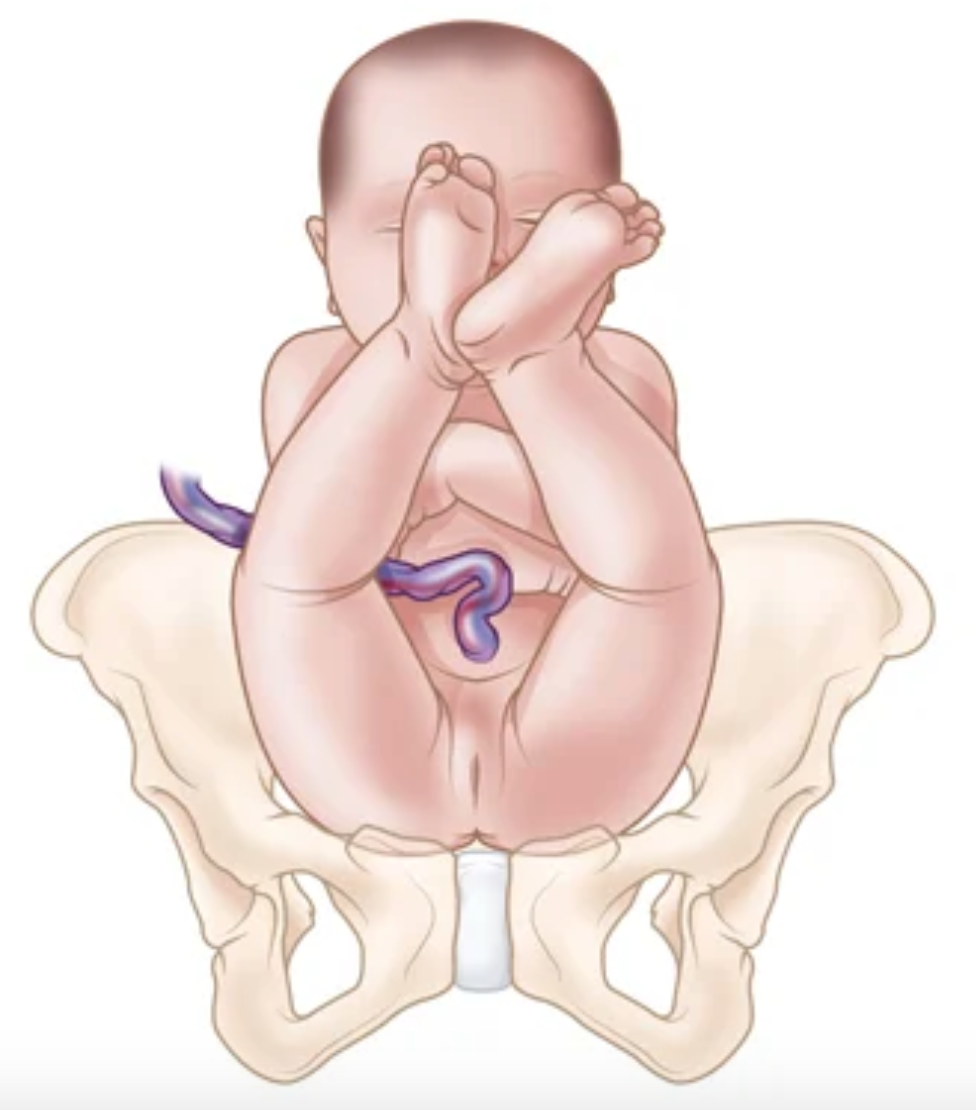
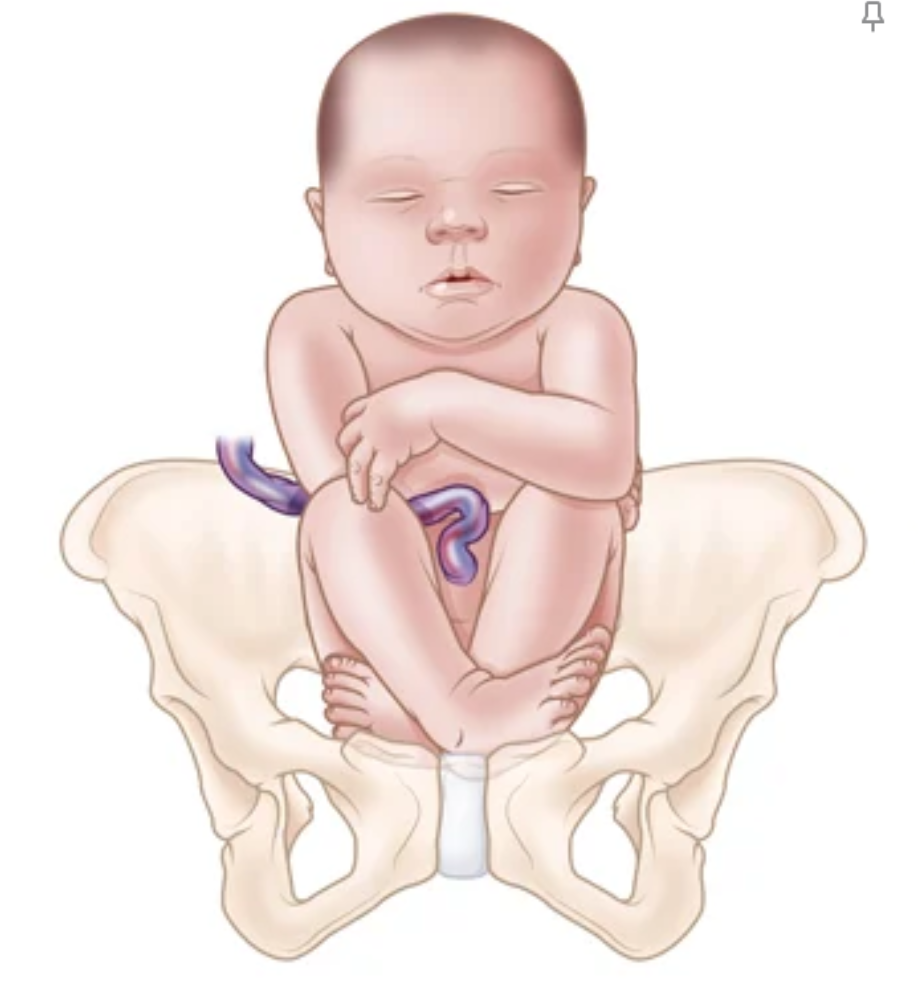

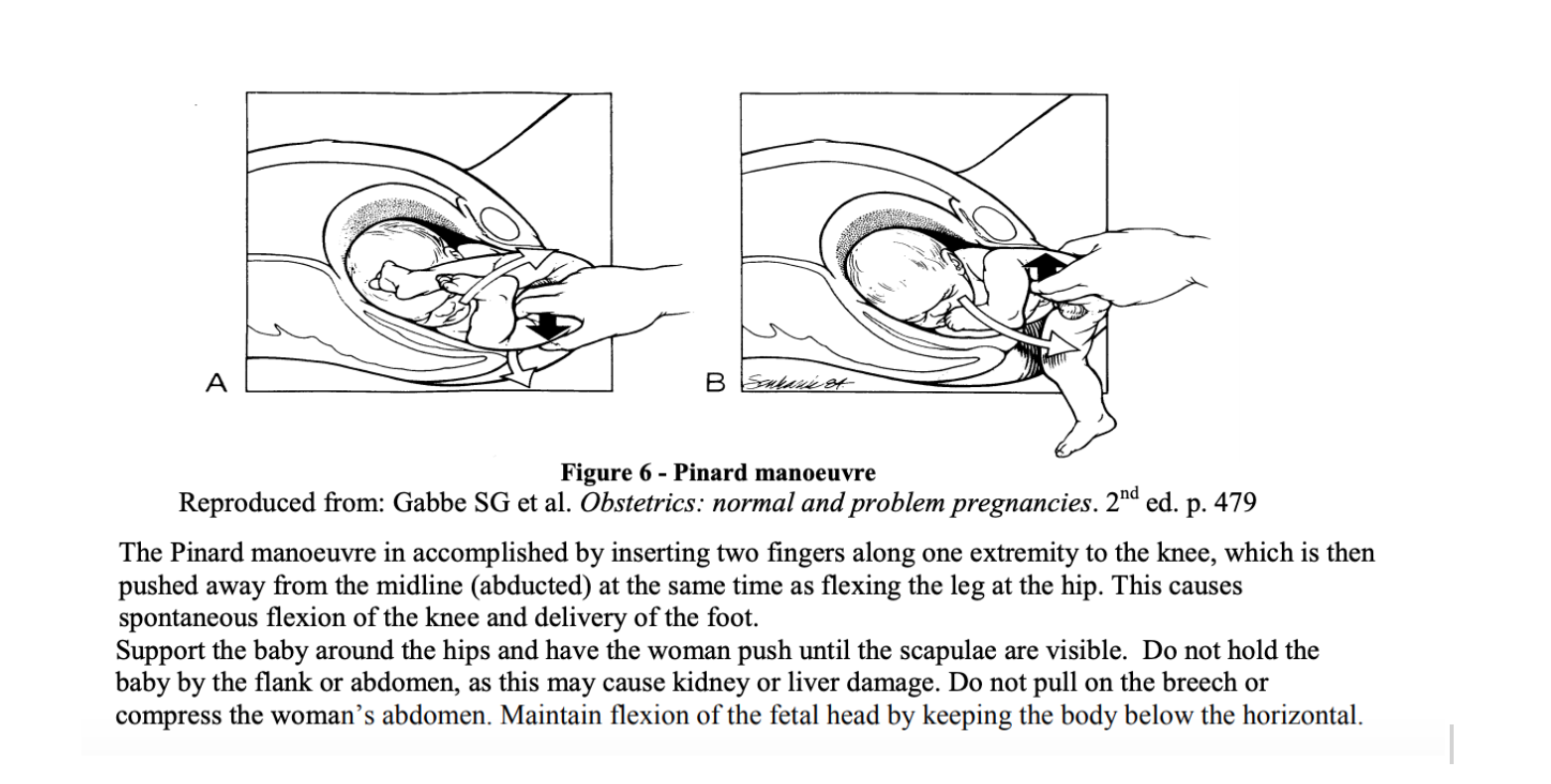
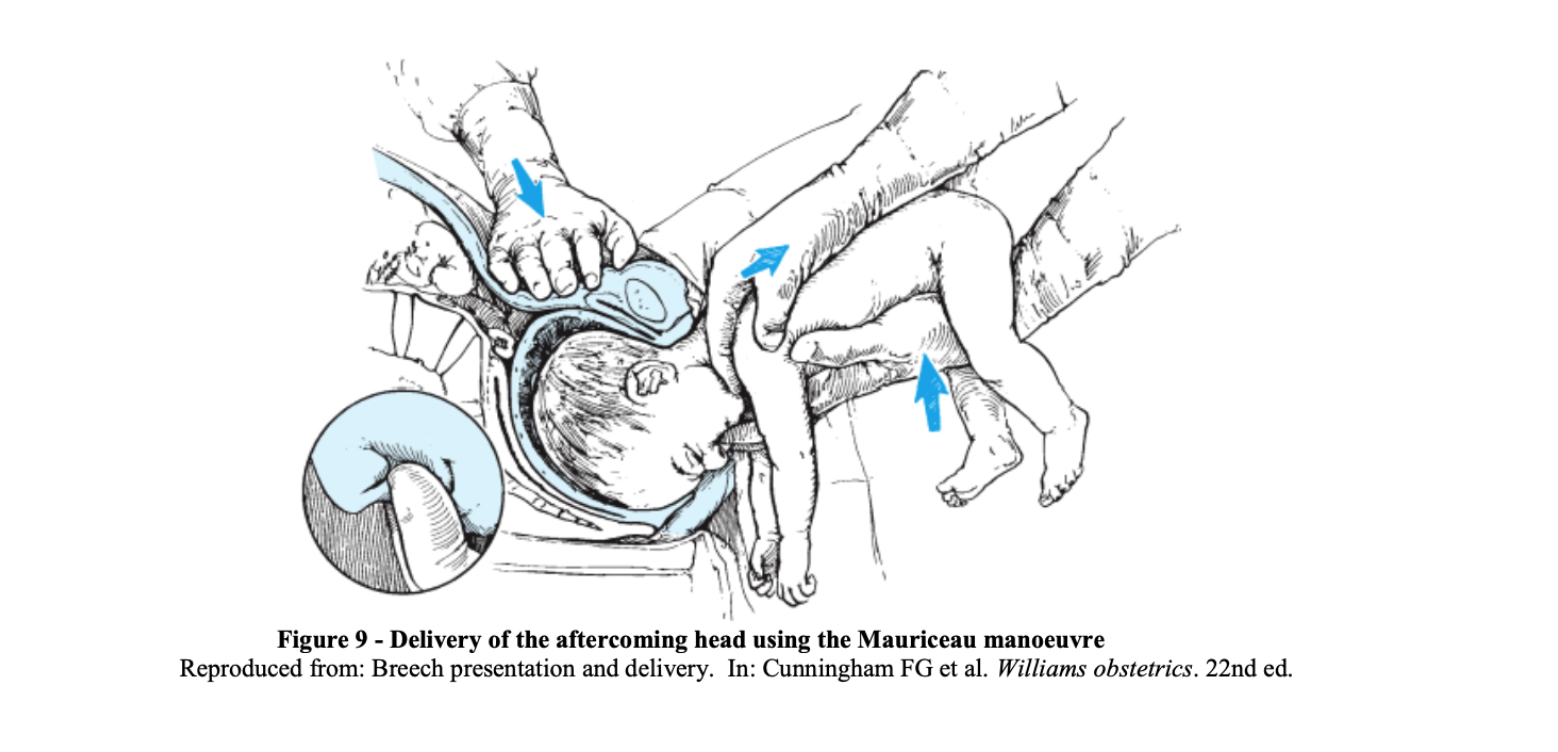
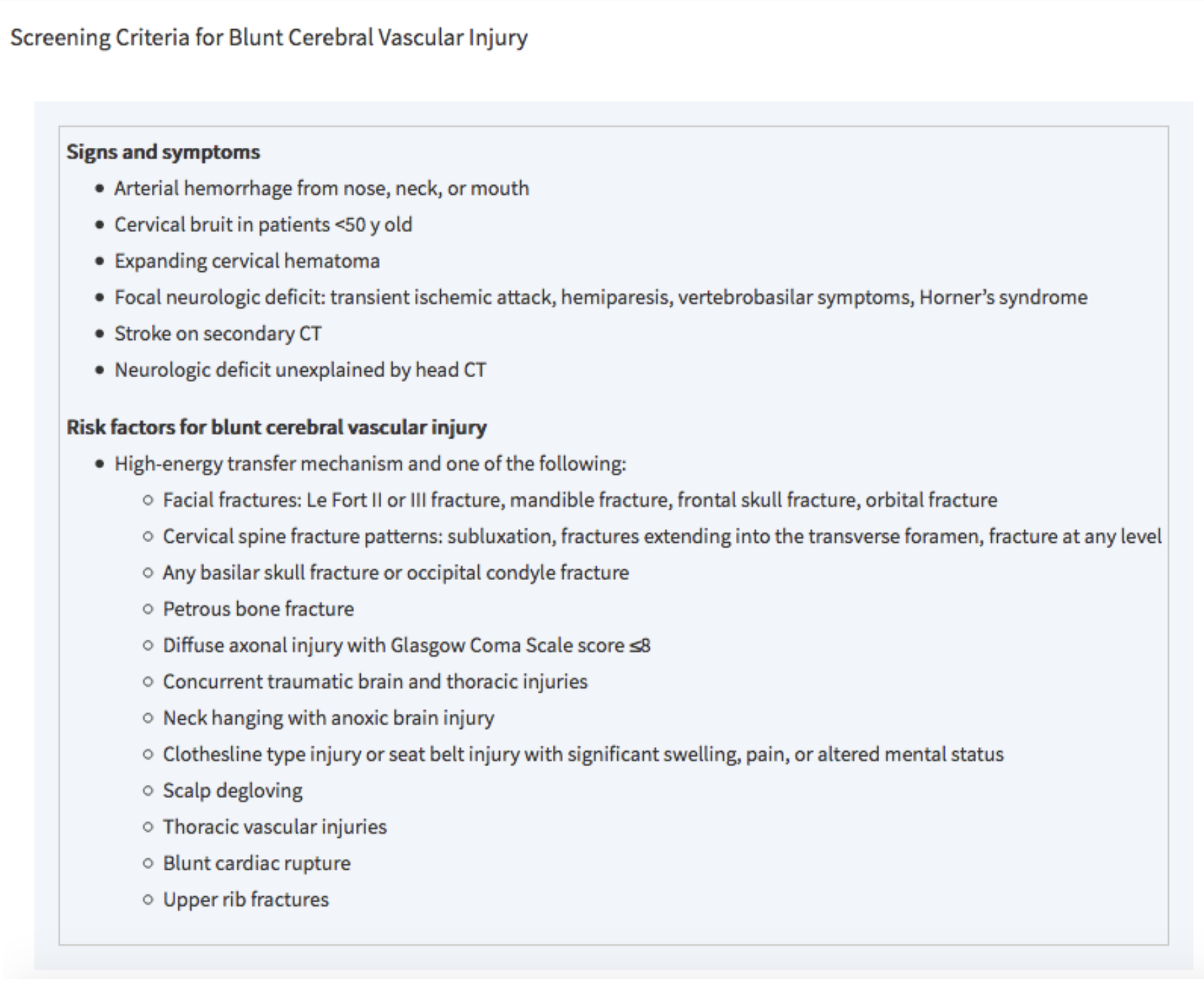
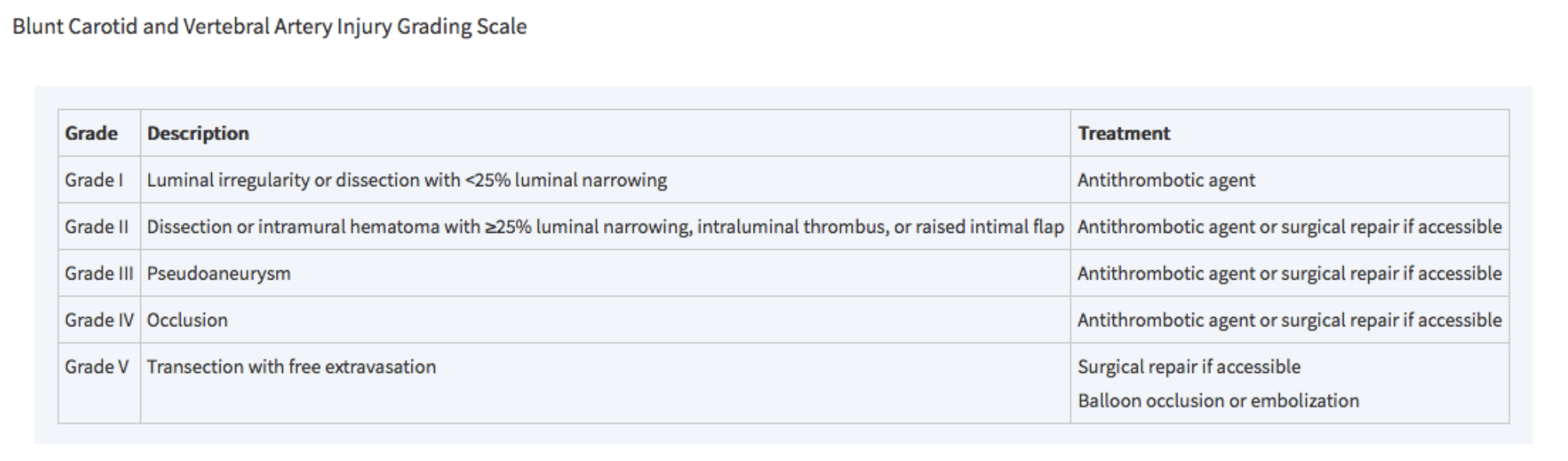
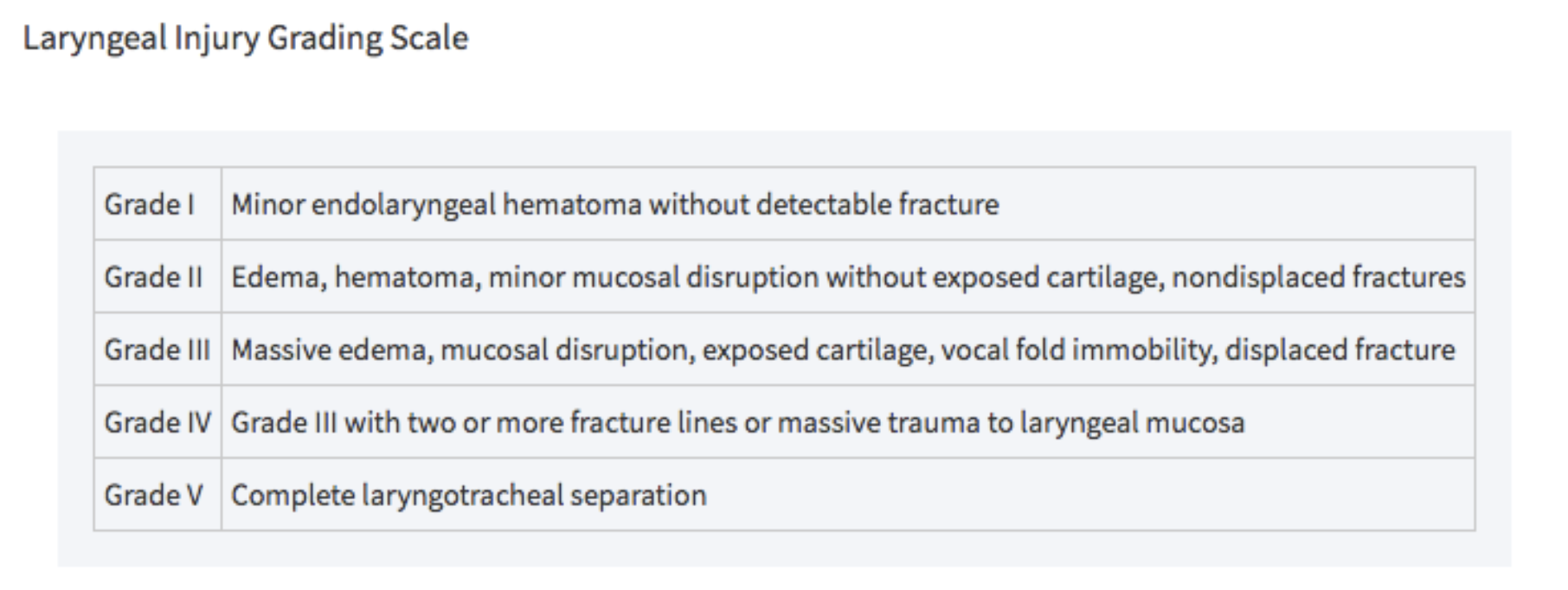 Tintinalli 2018
Tintinalli 2018